Jones Fracture | Zone Classification | High Non-Union Risk
ZONE CLASSIFICATION (LAWRENCE & BOTTE)
Critical Must-Knows
- Zone 2 (Jones fracture) has watershed blood supply - high non-union risk
- Intramedullary screw fixation is treatment of choice in athletes
- Zone 1 (tuberosity) avulsions heal reliably with conservative treatment
- Delayed union common if conservative treatment of Zone 2
- Return to sport faster with surgical fixation (6-8 vs 12-20 weeks)
Clinical Pearls
- "Jones fracture is Zone 2 (NOT Zone 1 tuberosity avulsion)
- "Blood supply enters distally - Zone 2/3 is watershed area
- "Athletes with Zone 2 fractures should be offered surgery
- "Zone 1 avulsions rarely need surgery - peroneus brevis attachment
Clinical Imaging
Imaging Gallery

Critical Fifth Metatarsal Exam Points
Zone Classification
Zone 2 = Jones fracture at metaphyseal-diaphyseal junction. Often confused with Zone 1 tuberosity avulsion. Zone 2 has watershed blood supply and high non-union risk.
Blood Supply
Nutrient artery enters distally, retrograde flow to proximal metaphysis. Zone 2/3 is watershed area between nutrient artery and metaphyseal vessels.
Surgical Indications
Athletes with Zone 2/3 fractures should be offered surgery. Intramedullary screw fixation provides faster healing (6-8 weeks vs 12-20 weeks conservative).
Conservative Success
Zone 1 avulsions heal reliably with NWB casting 4-6 weeks. Conservative treatment of Zone 2/3 in non-athletes requires strict NWB 6-8 weeks.
Quick Decision Guide by Zone
| Zone | Location | Mechanism | Non-Union Risk | Treatment |
|---|---|---|---|---|
| Zone 1 | Tuberosity | Avulsion (inversion) | Less than 5% | Conservative - NWB cast 4-6 weeks |
| Zone 2 (Jones) | Metaphyseal-diaphyseal junction | Acute stress/trauma | 25-50% | Surgery for athletes; conservative option for non-athletes |
| Zone 3 | Proximal diaphysis | Repetitive stress | 30-50% | Surgery strongly recommended - bone graft may be needed |


JONES - JJONES - Jones Fracture Features
| J | Junction Metaphyseal-diaphyseal junction location |
| O | Orthopaedic concern High non-union rate requires careful management |
| N | Nutrient artery Watershed zone - poor blood supply |
| E | Elite athletes Surgery recommended for faster return |
| S | Screw fixation Intramedullary screw is treatment of choice |
| J | Junction Metaphyseal-diaphyseal junction location | E | Elite athletes Surgery recommended for faster return |
| O | Orthopaedic concern High non-union rate requires careful management | S | Screw fixation Intramedullary screw is treatment of choice |
| N | Nutrient artery Watershed zone - poor blood supply |
Hook:Keep JONES in mind when managing metaphyseal-diaphyseal junction fractures
ZONES - FZONES - Fifth Metatarsal Zones
| Z | Zone 1 tuberosity Avulsion - heals well conservatively |
| O | Orthopaedic junction Zone 2 Jones - high non-union risk |
| N | Need surgery Zone 2/3 Athletes should have surgery |
| E | Entry of nutrient artery Distal entry creates watershed |
| S | Stress fracture Zone 3 Proximal diaphysis - highest risk |
| Z | Zone 1 tuberosity Avulsion - heals well conservatively | E | Entry of nutrient artery Distal entry creates watershed |
| O | Orthopaedic junction Zone 2 Jones - high non-union risk | S | Stress fracture Zone 3 Proximal diaphysis - highest risk |
| N | Need surgery Zone 2/3 Athletes should have surgery |
Hook:Remember the ZONES from proximal to distal when evaluating 5th metatarsal pain
SCREW - SSCREW - Surgical Indications
| S | Sports athlete Competitive or professional athletes |
| C | Complete fracture Displaced or complete Zone 2/3 fracture |
| R | Recurrent fracture Previous fracture or delayed union |
| E | Elite performance needs Faster return required |
| W | Widened fracture line Evidence of chronic stress reaction |
| S | Sports athlete Competitive or professional athletes | E | Elite performance needs Faster return required |
| C | Complete fracture Displaced or complete Zone 2/3 fracture | W | Widened fracture line Evidence of chronic stress reaction |
| R | Recurrent fracture Previous fracture or delayed union |
Hook:Use a SCREW when any of these indications are present
CAST - CCAST - Conservative Management Criteria
| C | Compliant patient Will adhere to NWB protocol |
| A | Acute Zone 1 fracture Tuberosity avulsion - best candidate |
| S | Sedentary or low-demand Non-athlete with lower expectations |
| T | Time available Can accept 12-20 week recovery |
| C | Compliant patient Will adhere to NWB protocol | S | Sedentary or low-demand Non-athlete with lower expectations |
| A | Acute Zone 1 fracture Tuberosity avulsion - best candidate | T | Time available Can accept 12-20 week recovery |
Hook:Only CAST when all these criteria are met for Zone 2/3 fractures
Overview and Epidemiology
Fifth metatarsal fractures are common foot injuries with significant variation in prognosis based on anatomical zone. The proximal fifth metatarsal is the most commonly fractured metatarsal.
Epidemiology:
- Peak incidence in 20-40 year age group
- Male predominance, especially in athletes
- Common in basketball, football, soccer, and running sports
- Associated with pes cavus foot type
- Increased risk with tight gastrocnemius and varus hindfoot
Historical context:
- First described by Sir Robert Jones in 1902 (his own injury during dancing)
- Original Jones fracture was Zone 2 location
- Term often incorrectly applied to Zone 1 avulsion fractures
- Torg classification (1984) refined understanding of healing potential
Terminology Clarity
A true Jones fracture is a Zone 2 fracture at the metaphyseal-diaphyseal junction - NOT a tuberosity avulsion (Zone 1). Sir Robert Jones sustained his injury while dancing, and it was at the proximal diaphysis, not the tuberosity.
Pathophysiology and Mechanisms
Fifth metatarsal anatomy:
- Most lateral metatarsal, articulates with cuboid proximally
- Styloid process (tuberosity) projects proximally and laterally
- Insertion of peroneus brevis on tuberosity
- Peroneus tertius inserts on dorsal shaft
Zone anatomy (Lawrence and Botte):
Tuberosity (Avulsion Zone):
- Proximal tip of styloid process
- Site of peroneus brevis insertion
- Well-vascularized from metaphyseal vessels
- Cancellous bone - heals readily
- Mechanism: Inversion injury, peroneus brevis avulses fragment
Excellent healing potential due to good blood supply.
Blood supply:
- Nutrient artery enters distal third of metatarsal shaft
- Blood flows retrograde (distally to proximally)
- Metaphyseal vessels supply proximal tuberosity
- Watershed zone at Zone 2 where supplies meet
- Limited periosteal blood supply in proximal diaphysis
Vascular Watershed
The metaphyseal-diaphyseal junction (Zone 2) represents a watershed zone between the nutrient artery and metaphyseal vessels. This explains the high non-union rate despite adequate fracture reduction.
Blood Supply Key
The nutrient artery enters distally and flows retrograde. Zone 2 is the watershed zone where nutrient artery territory meets metaphyseal vessels. This anatomical fact explains why Zone 2/3 fractures have such high non-union rates compared to Zone 1.
Classification Systems
Lawrence and Botte Zone Classification (1993) - Standard for exam
| Zone | Location | Characteristic | Treatment | Prognosis |
|---|---|---|---|---|
| Zone 1 | Tuberosity | Avulsion fracture | Conservative | Excellent |
| Zone 2 | Metaphyseal-diaphyseal junction | Jones fracture | Surgical for athletes | Guarded |
| Zone 3 | Proximal diaphysis | Stress fracture | Surgical | Poor if delayed |
This is the most clinically useful classification system.
History
Key history points:
- Acute trauma vs insidious onset (stress fracture)
- Mechanism: inversion, direct blow, repetitive stress
- Previous foot injuries or fractures
- Training changes (mileage, intensity, surface)
- Shoe wear and orthotics
- Sport and activity level
Risk factors for stress fracture:
- Rapid training increases
- Change in running surface
- Improper footwear
- Pes cavus foot type
- Previous fifth metatarsal fracture
- Female athlete triad
- Vitamin D deficiency
Thorough history helps distinguish acute injury from chronic stress reaction.
Examination
Physical examination:
Inspection:
- Swelling location (lateral midfoot)
- Ecchymosis
- Foot alignment (pes cavus, hindfoot varus)
- Weight-bearing posture
Palpation:
- Point tenderness over base of 5th metatarsal
- Zone 1 vs Zone 2 vs Zone 3 location
- Comparison to contralateral side
Special tests:
- Weight bearing tolerance
- Single leg hop test (stress fracture screening)
- Gastrocnemius/soleus flexibility
- Ankle ROM and stability
Precise localization of tenderness helps determine zone involvement.
Investigations
X-ray:
- AP, lateral, and oblique foot views
- Acute fracture: visible fracture line
- Stress reaction: periosteal reaction, cortical thickening
- Chronic: medullary sclerosis, widened fracture line
- Compare to contralateral foot for subtle findings
CT scan:
- Assess fracture healing
- Evaluate medullary canal sclerosis
- Preoperative planning for screw sizing
- Detect occult stress fractures
MRI:
- Early stress reaction detection (bone marrow edema)
- Soft tissue assessment
- Evaluate for associated injuries
- Most sensitive for occult fractures
Imaging Choice
X-ray is first-line for acute injury. MRI is most sensitive for early stress reaction (before cortical break). CT is useful for assessing healing and preoperative planning.
Management Algorithm
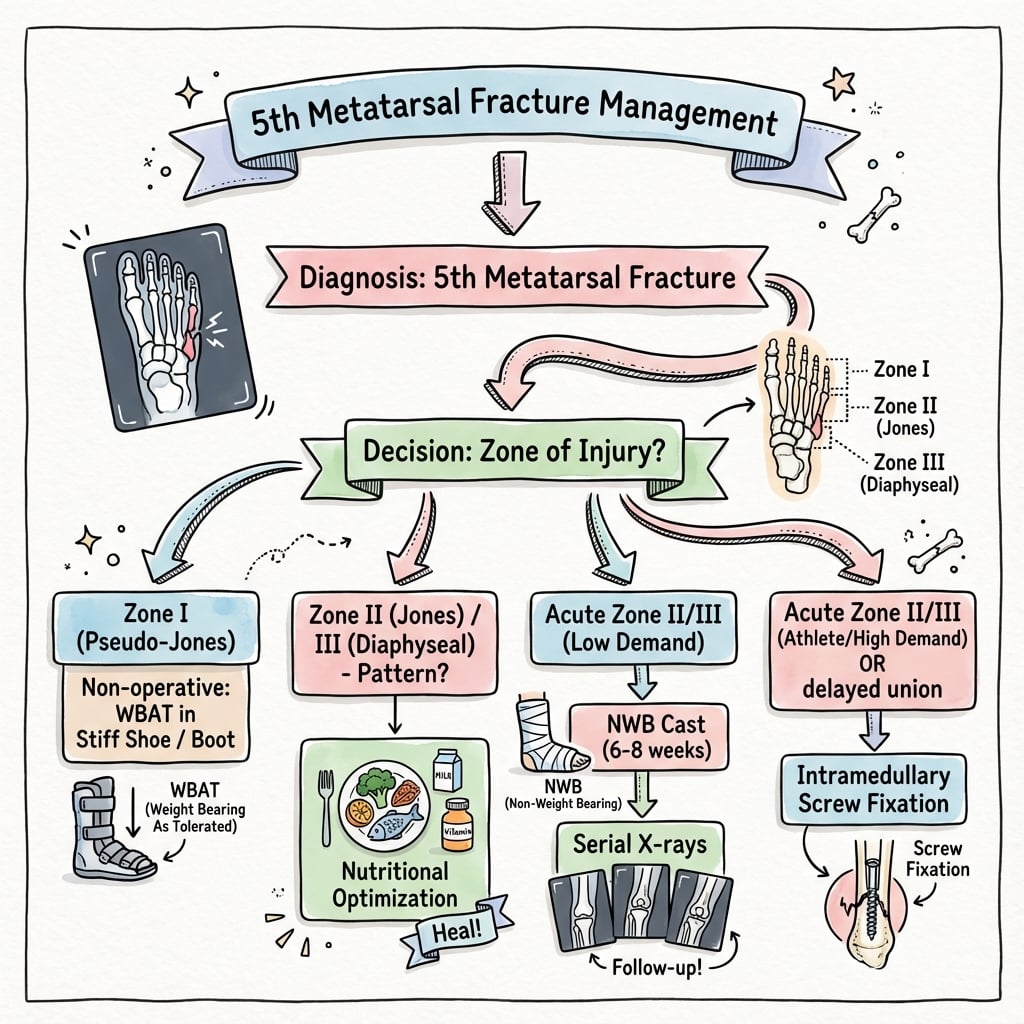
Conservative treatment (standard):
Non-displaced (most common):
- Hard-soled shoe or short leg walking boot
- Weight bearing as tolerated
- 4-6 weeks immobilization
- Activity progression when pain-free
Displaced fractures:
- Short leg non-weight bearing cast 4-6 weeks
- Followed by walking boot 2-4 weeks
- Surgery rarely needed unless significant displacement
Surgical indications (rare):
- Displacement greater than 2mm
- Large fragment with significant articular involvement
- Failed conservative treatment
Zone 1 avulsions heal reliably due to excellent blood supply.
Surgical Technique
Surgical indications:
Absolute:
- Competitive athletes with Zone 2/3 fractures
- Torg Type III non-unions
- Failed conservative management
Relative:
- Torg Type II delayed unions
- High-demand recreational athletes
- Patient preference for faster return
Contraindications:
- Active infection
- Severe peripheral vascular disease
- Medical comorbidities precluding surgery
Surgical treatment offers faster, more reliable healing for active patients.
Complications
Non-union (most common complication):
Risk factors:
- Zone 2/3 location
- Conservative treatment of high-risk fractures
- Torg Type II or III at presentation
- Non-compliance with weight-bearing restrictions
- Smoking
Management:
- Revision surgery with debridement
- Bone grafting (autograft preferred)
- Larger diameter screw
- Consider low-intensity pulsed ultrasound (LIPUS)
Outcomes:
- Union rate 90%+ with bone graft
- Return to sport typically possible
- May require extended rehabilitation
Non-union is common with Zone 2/3 fractures and requires aggressive treatment.
Postoperative Care
Standard postoperative protocol after intramedullary screw fixation:
Immediate postoperative:
- Posterior splint or CAM boot
- Non-weight bearing
- Elevation and ice for swelling
- Wound care at 10-14 days
- Pain management
Activity:
- Upper body and core exercises allowed
- Ankle ROM exercises in boot
- No weight bearing on operative foot
Initial protection allows fracture healing to begin.
Conservative Recovery
Conservative treatment of Zone 2/3 fractures requires 12-20 weeks for return to sport compared to 6-8 weeks with surgical treatment. This significant difference drives the recommendation for surgery in athletes.
Outcomes and Prognosis
Outcomes by zone and treatment:
| Zone | Treatment | Union Rate | Time to Union | Return to Sport |
|---|---|---|---|---|
| Zone 1 | Conservative | 95%+ | 6-8 weeks | 8-10 weeks |
| Zone 2/3 | Conservative | 70-75% | 12-20 weeks | 15-25 weeks |
| Zone 2/3 | Surgical (screw) | 90-95% | 6-8 weeks | 8-10 weeks |
| Non-union | Surgery + graft | 90-95% | 10-14 weeks | 12-16 weeks |
Factors affecting outcome:
- Zone of fracture (Zone 1 best, Zone 3 worst)
- Chronicity at presentation (acute better than chronic)
- Treatment selection (surgery better for athletes)
- Compliance with rehabilitation
- Underlying biomechanical factors
Long-term outcomes:
- Majority return to pre-injury sport level
- Recurrence more common with conservative treatment
- Hardware symptoms may require screw removal
- Addressing biomechanics reduces recurrence
Prognosis Summary
Zone 1 fractures have excellent prognosis with conservative treatment. Zone 2/3 fractures in athletes should have surgical treatment for faster, more reliable union. Established non-unions require bone grafting with 90%+ success.
Evidence Base
Mologne RCT: Early Screw Fixation vs Casting for Acute Jones Fractures
- Cast group: 8 of 18 (44%) treatment failures (5 non-unions, 1 delayed union, 2 refractures)
- Screw group: 1 of 19 a treatment failure
- Median union and return to sport: 7.5 and 8.0 weeks (screw) vs 14.5 and 15.0 weeks (cast)
- Difference statistically significant for both endpoints (P less than 0.01)
Porter: 5.5 mm vs 4.5 mm Cannulated Screw for Jones Fracture
- 5.5 mm group: 96.7% average radiographic healing, 100% clinical healing
- Mean return to sport 9.3 weeks; three re-injuries managed in a boot
- No significant difference demonstrated between 5.5 mm and 4.5 mm screws
- Authors could not conclude a larger screw is more effective with the numbers available
Glasgow & Torg: Why Surgical Jones Fracture Treatment Fails
- Failures split between intramedullary screw fixation (6) and inlaid corticocancellous graft (5)
- For screw fixation, using other than a 4.5 mm ASIF malleolar screw correlated with failure
- For bone graft, undersized grafts and incomplete medullary reaming correlated with failure
- Early return to vigorous activity contributed to delayed union and refracture
Torg: Original Classification of Base of Fifth Metatarsal Fractures
- Three types defined: acute (narrow line, no sclerosis), delayed union, and non-union (medullary obliteration)
- Acute fractures in a non-weight-bearing toe-to-knee cast: 14 of 15 healed (mean 7 weeks)
- Acute fractures treated with weight-bearing methods: only 4 of 10 united
- Non-unions treated with medullary curettage and bone graft: 8 of 9 healed (mean 3 months)
Wright: Refracture After Intramedullary Screw Fixation in Athletes
- Athletes released to full activity at a mean of 8.5 weeks (range 5.5-12)
- Three footballers refractured within one day of returning to full activity
- Two footballers re-fixed with larger screws returned to play the same season
- Authors advise larger-diameter screws for high-body-mass athletes plus bracing or orthoses for return to play
O'Malley: Operative Treatment of Jones Fractures in the NBA
- Percutaneous fixation augmented with bone marrow aspirate concentrate; 3 had primary open bone grafting
- Average radiographic healing 7.5 weeks; return to play 9.8 weeks
- Three athletes refractured; the refracture group had the highest metatarsus adductus angles
- Most players were pes planus with a curved, prominent fifth metatarsal base
Buskova & Rammelt: Critical Analysis Review of Base of Fifth Metatarsal Fractures
- Proximal fifth metatarsal fractures account for 61% to 78% of all foot fractures
- Lawrence and Botte three-zone scheme is the most widely accepted classification
- Zone 1 avulsions generally heal with non-operative functional treatment
- Zone 3 diaphyseal stress fractures are preferentially treated operatively, especially with delayed union
Polzer: Systematic Review and Refined Treatment Recommendations
- All Zone 1 tuberosity avulsions healed well with functional treatment, even when displaced or intra-articular
- A short leg cast significantly delayed return to pre-injury level versus functional treatment
- Zone 3 meta-diaphyseal fractures had significantly higher non-operative failure than Zone 1/2
- Early intramedullary screw fixation shortened time to union and return to sport
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Professional Footballer with Jones Fracture
"A 25-year-old professional footballer presents with an acute Jones fracture (Zone 2) after a twisting injury. X-ray shows a sharp fracture line without sclerosis. He has an important match in 8 weeks. How would you manage this patient?"
Scenario 2: Zone 1 Avulsion in Recreational Athlete
"A 40-year-old recreational tennis player presents after an inversion injury with pain at the base of the fifth metatarsal. X-ray shows a 4mm displaced avulsion of the tuberosity (Zone 1). How would you manage this?"
Scenario 3: Non-Union After Conservative Treatment
"A 28-year-old amateur footballer was treated conservatively for a Jones fracture 4 months ago. He continues to have pain and X-ray shows a widened fracture line with medullary sclerosis. How would you manage this non-union?"
MCQ Practice Points
MCQ Focus: Nerve Injury
Q: Which nerve is most commonly injured during the approach for 5th metatarsal screw fixation? A: Dorsolateral Branch of the Sural Nerve. It runs along the lateral aspect of the foot and is at risk with lateral dissection or drill guide placement.
MCQ Focus: Watershed Area
Q: Which arterial supply is deficient at the Zone 2/3 junction? A: The area is a watershed vascular zone between the intramedullary nutrient artery (diaphyseal) and the metaphyseal/periosteal vessels.
MCQ Focus: Screw Position
Q: What is the optimal starting point for an intramedullary screw in the 5th metatarsal? A: High and Inside (Dorsal and Medial) on the base. This aligns the screw with the straight distal segment of the canal.
MCQ Focus: Torg Classification
Q: What defines a Torg Type II fracture? A: Widened fracture line with intramedullary sclerosis. Type I has no sclerosis. Type III has complete canal obliteration.
MCQ Focus: Healing Time
Q: How long does conservative treatment typically take for union in a Zone 3 stress fracture? A: 12-20 weeks (3-5 months). This prolonged time is why surgical fixation (6-8 weeks) is preferred for athletes.
Guidelines, Registries & Global Practice
Global epidemiology:
| Metric | Figure | Source |
|---|---|---|
| Share of all foot fractures (proximal fifth metatarsal) | 61% to 78% | Buskova/Rammelt, JBJS Rev 2021 (PMID 34673663) |
| Most common fractured metatarsal | Fifth (proximal) | Cheung & Lui, Arch Trauma Res 2016 (PMID 28144601) |
| Highest-risk zone for non-union | Zone 2/3 (meta-diaphyseal) | Polzer, Injury 2012 (PMID 22465516) |
There is no dedicated international registry for fifth metatarsal fractures (unlike arthroplasty registries such as AOANJRR or NJR). The evidence base is therefore built on a single Level I RCT (Mologne, PMID 15888715) plus systematic reviews and athlete case series, which drives the practice variation below.
Side-by-side guidance and consensus (no single global guideline exists):
| Body / source | Position on Zone 1 | Position on Zone 2/3 in athletes | Evidence level |
|---|---|---|---|
| Polzer systematic review (EFORT-region, Injury 2012) | Functional treatment for all tuberosity avulsions | Early IM screw fixation for meta-diaphyseal fractures | Systematic review (Level II) |
| JBJS critical analysis review 2021 | Non-operative; functional | IM fixation to reduce healing time / expedite RTS | Review (Level III) |
| AOFAS / sports surgeon consensus (USA) | Symptomatic, weight-bear as tolerated | IM screw fixation, often with biologic augmentation | Expert consensus + RCT |
| BOA / BOFAS practice (UK) | Functional bracing, early mobilisation | Surgery for elite/high-demand; non-op acceptable in low-demand | Expert consensus |
Practice variation:
- North American sports practice favours early fixation plus bone marrow aspirate concentrate in elite athletes (O'Malley, PMID 26781131).
- European practice (Polzer) emphasises functional treatment for metaphyseal fractures and reserves fixation for true Zone 3 meta-diaphyseal fractures.
- Screw size remains debated: Porter (PMID 19176182) found no proven advantage of 5.5 mm over 4.5 mm, while failure analyses (Glasgow/Torg, PMID 8863022) link undersized fixation to failure.
Australian context:
- Common in Australian Rules Football, rugby league, soccer and basketball, with peaks during pre-season loading.
- Sports physicians and orthopaedic surgeons co-manage elite athletes; AFL and NRL medical units have structured early-detection and return-to-sport protocols and frequently proceed to in-season surgical fixation.
- Good MRI access supports early stress-reaction detection; bone-health screening, training-load monitoring and orthotic assessment are used for prevention.
Australian Sport Context
Fifth metatarsal stress fractures are common in Australian Rules Football due to the cutting, pivoting and rapid acceleration demands. AFL medical teams have structured protocols for early detection and often proceed directly to surgical fixation for in-season fractures.
Fifth Metatarsal Stress Fractures
Clinical summary
Zone Classification
- •Zone 1: Tuberosity avulsion - excellent prognosis
- •Zone 2: Jones fracture (metaphyseal-diaphyseal junction) - high non-union
- •Zone 3: Proximal diaphyseal stress fracture - highest non-union risk
- •True Jones = Zone 2, NOT Zone 1
Blood Supply
- •Nutrient artery enters distally - retrograde flow
- •Zone 2 is watershed zone
- •Poor blood supply = high non-union rate
- •Metaphyseal vessels supply tuberosity (Zone 1)
Torg Classification
- •Type I (acute): Sharp margins, no sclerosis
- •Type II (delayed): Widened line, some sclerosis
- •Type III (non-union): Wide gap, complete sclerosis
- •Sclerosis indicates need for surgery
Treatment by Zone
- •Zone 1: Conservative - NWB cast 4-6 weeks
- •Zone 2/3 athletes: Surgery - IM screw fixation
- •Zone 2/3 non-athletes: Conservative option with monitoring
- •Non-union: Surgery + bone graft
Surgical Technique
- •Entry point: most proximal/lateral tuberosity
- •Largest diameter screw (5mm or greater preferred)
- •Headless compression screw
- •Pitfall: entry too medial = varus angulation
Outcomes
- •Zone 1 conservative: 95% union, 8-10 weeks RTS
- •Zone 2/3 surgical: 90-95% union, 6-8 weeks RTS
- •Zone 2/3 conservative: 70-75% union, 12-20 weeks RTS
- •Surgery offers faster, more reliable healing