Finger Dislocations
PIP and DIP Joint Injuries | Management Algorithms | Exam Pearls
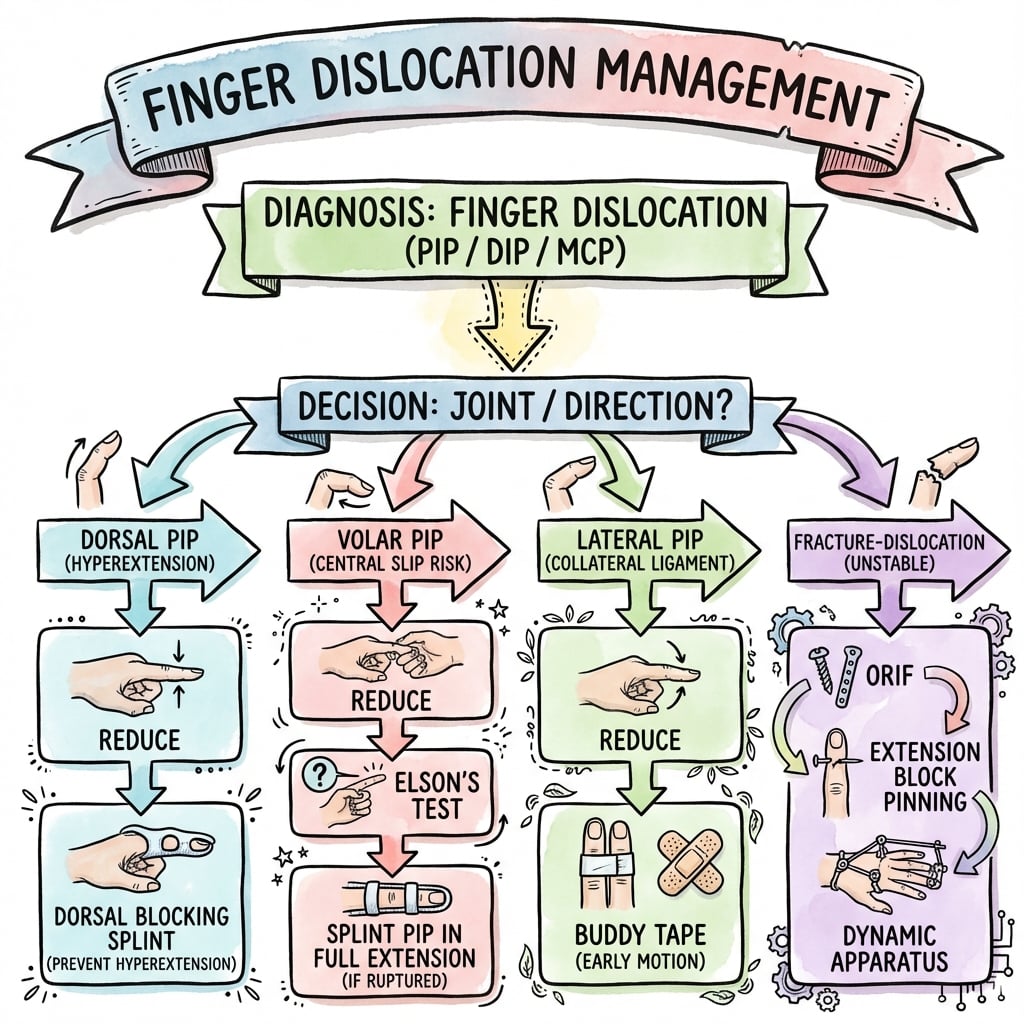
DISLOCATION TYPES
Critical Must-Knows
- Dorsal PIPJ is most common; treated with early motion and buddy taping.
- Volar PIPJ is rare but critical - central slip injury requires 6 weeks extension splint.
- V-sign on lateral X-ray indicates dorsal subluxation and joint instability.
- Digital blocks are required for reduction and comprehensive stability assessment.
- Complications include permanent fusiform thickening and chronic stiffness.
Clinical Pearls
- "Early motion for dorsal; strict extension for volar. Mismanaging volar causes Boutonnière.
- "Assess collateral stability in 30° of flexion after successful reduction.
- "Irreducible dislocations usually implicate volar plate or FDP tendon entrapment.
- "Check for 'Volar Plate Sign' - small avulsion fragment from middle phalanx base.
Clinical Imaging
Imaging Gallery


Critical Exam Points: PIPJ Dislocations
Dorsal vs Volar Distinction
Crucial Distinction:
- Dorsal: Volar plate avulsion. Treat with early motion (buddy tape) to prevent stiffness.
- Volar: Central slip rupture. Treat with static extension splint (6 weeks) to prevent Boutonnière deformity.
The 'V-Sign' Instability
On lateral X-ray, dorsal subluxation creates a V-shaped joint space. This indicates instability and often requires extension block splinting or surgical intervention.
Stiffness and Swelling
Fusiform swelling and stiffness persist for months. Early mobilization is key for stable (dorsal) dislocations. Always warn patients about permanent finger thickening.
At a Glance
Finger Fracture-Dislocation Patterns
| Pattern | Mechanism | Stability | Treatment |
|---|---|---|---|
| Simple Dorsal | Hyperextension | Stable | Buddy tape / Early motion |
| Volar Dislocation | Rotational / Volar force | Unstable (Central Slip) | Extension splint 6 weeks |
| Complex Fracture | Articular greater than 40% | Unstable | Surgical Fixation |
| Lateral | Collateral stress | Stable | Buddy tape 4 weeks |
Mnemonics
DORALDorsal vs Volar Distinction
| D | Dorsal Most common direction |
| O | Open Often associated with skin tears (DIPJ) |
| R | Reduction Traction and flexion |
| A | Active Early active motion is key |
| L | Lithgow Lithgow criteria for stability |
| D | Dorsal Most common direction | A | Active Early active motion is key |
| O | Open Often associated with skin tears (DIPJ) | L | Lithgow Lithgow criteria for stability |
| R | Reduction Traction and flexion |
Hook:Dorsal dislocations are the 'Typical' type - keep 'em moving!
VOLARVolar Dislocation Management
| V | Volar Middle phalanx volar to proximal |
| O | Obligatory Central slip injury is mandatory |
| L | Look Check for boutonniere (delayed) |
| A | Avoid Avoid flexion for 6 weeks |
| R | Rigid Rigid extension splinting |
| V | Volar Middle phalanx volar to proximal | A | Avoid Avoid flexion for 6 weeks |
| O | Obligatory Central slip injury is mandatory | R | Rigid Rigid extension splinting |
| L | Look Check for boutonniere (delayed) |
Hook:Volar = Volatile behavior of the central slip. Splint it!
VSIGNThe V-Sign of Instability
| V | V-shaped Gap on lateral X-ray |
| S | Subluxation Dorsal subluxation of joint |
| I | Incongruent Joint surfaces are not parallel |
| G | Grip Unstable grip on the phalanx |
| N | Next Next step: Extension block splinting |
| V | V-shaped Gap on lateral X-ray | G | Grip Unstable grip on the phalanx |
| S | Subluxation Dorsal subluxation of joint | N | Next Next step: Extension block splinting |
| I | Incongruent Joint surfaces are not parallel |
Hook:See the V? Think instability!
Overview and Epidemiology
Finger dislocations are among the most common hand injuries seen in both primary care and emergency departments. The Proximal Interphalangeal (PIPJ) joint is the most frequently affected, earning its reputation as the "workhorse" joint of the finger.
Mechanism of Injury
- Hyperextension: Most common mechanism for dorsal PIPJ dislocations.
- Axial Loading: Often seen in "jammed finger" sports injuries.
- Rotational Stress: Results in lateral dislocations and collateral ligament disruption.
- Volar Displacement: Occurs with a palm-directed force on a flexed finger, rupturing the central slip.
Anatomy & Joint Stabilisers
The PIPJ is a bicondylar hinge joint stabilised by a three-sided ligamentous "box". Understanding which wall fails dictates the direction of dislocation and the entire treatment pathway.
The PIPJ "Box":
- Volar: Volar plate (fibrocartilage) — resists hyperextension; thick distal attachment to the middle phalanx base, thin membranous proximal attachment (check-rein ligaments).
- Lateral: Proper and accessory collateral ligaments.
- Dorsal: Extensor mechanism — central slip inserts on the dorsal base of the middle phalanx; lateral bands run laterally.
Injury correlates:
- Dorsal dislocation → volar plate avulses distally (+/- small bony fragment, the "volar plate sign").
- Volar dislocation → central slip ruptures (obligatory, hence boutonnière risk).
- Lateral dislocation → collateral ligament disruption.
Systematic Review: Treatment of Acute PIPJ Fractures & Fracture-Dislocations
- 37 studies, 471 patients, 480 fingers reviewed (Level III).
- Volar plate arthroplasty achieved the greatest postoperative PIPJ arc (90.6 degrees); dynamic external fixation the lowest (79.7 degrees).
- Recurrent pain and osteoarthritis were highest after extension block pinning (38.5% and 46.2%); ORIF had the highest revision rate (19.7%).
- Closed reduction with percutaneous pinning and volar plate arthroplasty gave good outcomes with the lowest complication rates.
Hemi-Hamate Autograft for Unstable Dorsal PIPJ Fracture-Dislocations
- 13 consecutive patients; mean middle phalangeal volar lip involvement 60% (range 40-80%).
- Size-matched dorsal/distal hamate osteoarticular autograft secured with miniscrews reconstructs the cup-shaped middle phalanx base.
- Mean PIPJ arc 85 degrees; grip 80% of the uninjured side; bony union in all patients.
- Recommended when greater than 50% of the volar base is fractured, or when the joint stays unstable despite a smaller fragment.
Hemi-Hamate Arthroplasty: 10-Year Outcomes
- 12 patients (acute and chronic), mean follow-up 10.7 years.
- Mean active PIPJ arc 76.6 degrees; mean QuickDASH 12.7, mean VAS pain 1; grip and pinch comparable to the uninjured hand.
- Radiographic osteoarthritis in 7 of 12 patients and graft resorption in 3, both associated with reduced motion; union rate 91.6%.
- Despite degenerative change, subjective outcomes and strength remained satisfactory at a decade.
Dynamic (Syringe) External Fixation for Comminuted Intra-Articular Hand Fractures
- 27 patients, 29 MCP/PIP joint injuries treated with a low-cost fixator built from a 1-mL syringe and K-wires.
- Dynamic fixation at the PIPJ gave a mean active arc of 80 degrees (static 64 degrees; static-to-dynamic 66 degrees).
- Low complication profile: 3 pin-site infections and 2 loose pins.
- Ligamentotaxis maintains reduction while permitting early motion in highly comminuted patterns.
Extensor (Zone III) Injuries at the PIPJ: Central Slip & Elson Test
- Acute closed central slip injuries are diagnosed clinically with the Elson test once bony injury is excluded.
- Overlooked central slip injury produces a boutonnière deformity within 1-2 weeks (PIPJ extension lag, DIPJ hyperextension).
- Non-displaced central slip avulsions are treated by extension splinting; displaced or complex injuries are surgical.
- Volar PIPJ dislocation should be managed as an acute central slip injury to prevent fixed deformity.
Volar Plate Arthroplasty (Classification & Technique)
- Described advancement of the volar plate into the articular defect for dorsal PIPJ fracture-dislocations.
- Restores a stable concave gliding surface for the proximal phalanx condyles.
- Best suited to acute or chronic injuries with volar lip involvement up to ~40-50% without a reconstructable fragment.
- Remains a recognised option alongside hemi-hamate reconstruction for non-fixable volar base fractures.
PIPJ Stability Criteria (Articular Surface Rule)
- Volar lip fractures involving less than 30% of the articular surface are usually stable after reduction.
- Fractures involving greater than 50% of the articular surface are usually unstable and subluxate.
- The 30-50% range is a 'grey zone' requiring stress testing/fluoroscopy to define the stable arc.
- Foundation for the modern conservative-versus-surgical treatment algorithm.
Differential Diagnosis
The swollen, deformed or "jammed" finger has several mimics. The key discriminators are the direction of deformity, active extension capacity, joint congruity on a true lateral film, and whether a mechanical block to reduction is present.
Differentiating the Injured PIPJ/DIPJ
| Diagnosis | Key clinical sign | Radiograph | Distinguishing feature |
|---|---|---|---|
| Dorsal PIPJ dislocation | Hyperextended, shortened finger; reduces easily | Middle phalanx dorsal; +/- small volar lip fragment | Volar plate avulsion; stable after reduction |
| Volar PIPJ dislocation | PIPJ flexed, cannot actively extend | Middle phalanx volar | Obligatory central slip rupture (boutonniere risk) |
| Lateral PIPJ / collateral sprain | Angular/rotational deformity, opens to stress | Often congruent; may show condylar avulsion | Collateral instability without overt dislocation |
| PIPJ fracture-dislocation | Persistent dorsal subluxation tendency | V-sign; volar lip fragment sized on lateral | Stability depends on fragment size (30/50 rule) |
| Acute boutonniere (closed central slip) | Extension lag at PIPJ, no dislocation | Normal or small dorsal base avulsion | Positive Elson test, joint located |
| Mallet finger (terminal extensor) | DIPJ extension lag, droop | +/- dorsal distal phalanx fragment | DIPJ not dislocated; PIPJ normal |
| Complex (irreducible) MCPJ dislocation | Skin puckering over palm, MCP hyperextended | Sesamoid in joint; parallel surfaces | Volar plate buttonholed around metacarpal head |
| Phalangeal/condylar fracture (no dislocation) | Focal bony tenderness, deformity | Fracture line, joint located | No frank dislocation; assess rotation |
Exam Viva Point
Two radiographic signs that change your plan:
- V-sign (dorsal V-shaped widening on the true lateral) means dorsal subluxation/instability and triggers extension block splinting or surgery.
- Parallel articular surfaces mean volar plate (or tendon) interposition and an irreducible joint, so proceed to open reduction rather than forcing closed reduction.
Classification
Classification by Direction
PIPJ Dislocations:
- Dorsal: Middle phalanx dorsal to proximal (most common)
- Volar: Middle phalanx volar to proximal (rare, central slip injury)
- Lateral: Collateral ligament disruption (rotatory component)
By Joint Involvement:
- Simple dislocation (soft tissue only)
- Fracture-dislocation (bony avulsion)
Classification Summary
| Type | Injured Structure | Stability |
|---|---|---|
| Dorsal simple | Volar plate | Usually stable post-reduction |
| Dorsal fracture-dislocation | Volar plate + bone | Depends on fragment size |
| Volar | Central slip | Requires extension splinting |
| Lateral | Collateral ligament | May have rotatory instability |
Clinical Assessment
History
Mechanism:
- Hyperextension injury (dorsal dislocation)
- Rotational force (lateral or volar)
- Ball sports most common (basketball, football, cricket)
Key Questions:
- Time since injury
- Previous reduction attempts
- Hand dominance and occupation
Examination
Inspection:
- Obvious deformity (dorsally or volarly displaced)
- Swelling and bruising
- Skin integrity (open injuries common in DIPJ)
Palpation and Assessment:
- Point tenderness
- Neurovascular status (capillary refill, sensation)
- Active ROM after reduction
Clinical Signs by Dislocation Type
| Type | Appearance | Key Finding |
|---|---|---|
| Dorsal PIPJ | Finger shortened, hyperextended posture | Volar plate avulsion on X-ray |
| Volar PIPJ | PIPJ flexed, DIP extended | Cannot actively extend PIPJ |
| Lateral | Ulnar/radial deviation | Rotational malalignment |
Investigations
Radiographic Assessment
Standard Views:
- AP, lateral, and oblique of affected finger
- TRUE lateral is essential for classification
Pre-Reduction X-ray:
- Confirm dislocation direction
- Identify associated fractures
- Assess joint congruity
Post-Reduction X-ray:
- Confirm concentric reduction
- Check for V-sign (dorsal subluxation)
- Assess fracture fragment position
X-ray Findings
| Finding | Significance | Action |
|---|---|---|
| Volar plate avulsion | Small fragment common in dorsal dislocation | Usually conservative if stable |
| V-sign | Dorsal subluxation indicating instability | Extension block splinting or surgery |
| Parallel articular surfaces | Volar plate interposition | Open reduction required |
Management Algorithm
Management
Treatment by Dislocation Type
Dorsal PIPJ (Most Common):
- Digital block anaesthesia
- Reduction: Longitudinal traction + flexion
- Assess stability through ROM
- If stable: Buddy taping, early motion
- If unstable: Extension block splinting
Volar PIPJ (Central Slip at Risk):
- Reduction: Traction + extension
- Test active PIPJ extension
- Static extension splint for 6 weeks
- Active DIP flexion exercises during immobilisation
DIPJ Dislocation:
- Usually dorsal, often open injury
- Digital block, irrigate if open
- Reduce and splint for 2-3 weeks
Treatment Algorithm
| Type | Stable | Unstable |
|---|---|---|
| Dorsal PIPJ | Buddy tape + early motion | Extension block splint |
| Volar PIPJ | Extension splint 6 weeks | Open repair if needed |
| Fracture-dislocation | Extension block if less than 30% | Surgery if greater than 40% |
Surgical Technique
Open Reduction Techniques
Indications for Surgery:
- Irreducible dislocation
- Fracture-dislocation greater than 40% articular surface
- Chronic dislocation
- Failed closed treatment
Surgical Approaches:
- Volar (Bruner) - preferred for volar plate extraction
- Dorsal - for central slip repair
- Lateral - for collateral ligament repair
Volar Approach Steps:
- Bruner zigzag incision over PIPJ
- Identify and protect neurovascular bundles
- Retract flexor tendons
- Identify interposed volar plate
- Extract and reduce joint
- Repair volar plate to bone (suture anchors)
Surgical Options
| Procedure | Indication | Key Points |
|---|---|---|
| ORIF | Large fragment fracture-dislocation | Screws, plate, or K-wires |
| Volar plate arthroplasty | Comminuted volar lip | Advance volar plate into defect |
| Hemihamate graft | Chronic defect greater than 50% | Autograft from hamate |
Complications
Common Complications
Stiffness (Most Common):
- Fusiform swelling persists for months
- Warn patients about permanent finger thickening
- Prevention: Early protected motion in dorsal dislocations
Boutonnière Deformity:
- PIPJ flexion with DIPJ hyperextension
- Results from untreated central slip injury
- Common after incorrectly mobilised volar dislocation
Swan Neck Deformity:
- PIPJ hyperextension with DIPJ flexion
- Results from volar plate laxity
- May follow chronic dorsal subluxation
Complication Summary
| Complication | Cause | Prevention |
|---|---|---|
| Stiffness | Prolonged immobilisation | Early motion (dorsal type) |
| Boutonnière | Central slip rupture | Extension splint 6 weeks (volar) |
| Swan neck | Volar plate laxity | Proper treatment of volar plate injury |
| Chronic instability | Inadequate healing | Appropriate splinting duration |
Postoperative Care
Rehabilitation Protocol
Dorsal Dislocation (Stable):
- Buddy taping to adjacent finger
- Immediate active motion exercises
- Full ROM expected by 4-6 weeks
- Protect during sports for 6-8 weeks
Volar Dislocation:
- Static extension splint (PIPJ in full extension)
- Allow DIP flexion exercises
- Maintain for 6 weeks minimum
- Progressive PIPJ flexion after 6 weeks
Post-Surgical:
- Extension block splinting 2-3 weeks
- Hand therapy referral essential
- Progressive extension by 10°/week
- Full motion by 6-8 weeks
Rehabilitation Timeline
| Phase | Dorsal (Stable) | Volar | Post-Surgery |
|---|---|---|---|
| Week 1-2 | Buddy tape, active ROM | Extension splint only | Extension block splint |
| Week 3-4 | Full motion, buddy tape sports | Extension splint, DIP exercises | Progressive extension |
| Week 5-6 | Return to sport | Begin gentle PIPJ flexion | Full ROM goals |
Outcomes
Expected Outcomes
Simple Dorsal Dislocation:
- Excellent prognosis with early motion
- Greater than 90% achieve functional ROM
- Residual stiffness common but usually mild
- Return to sport within 4-6 weeks
Volar Dislocation:
- Good outcomes if splinted correctly
- Higher complication rate than dorsal
- Boutonnière risk with improper treatment
- Full recovery may take 3-6 months
Fracture-Dislocation:
- Outcomes depend on articular involvement
- Less than 30% fragment: good prognosis
- Greater than 50% fragment: guarded prognosis
- Post-traumatic arthritis risk increases with severity
Outcome Summary
| Type | Good Result Rate | Main Risk |
|---|---|---|
| Dorsal simple | Greater than 90% | Stiffness |
| Volar | 80-85% | Boutonnière deformity |
| Fracture-dislocation | 60-80% | Arthritis, stiffness |
Evidence, Controversies & Areas of Uncertainty
The evidence base for PIPJ fracture-dislocations is almost entirely Level III-IV; there are no randomised trials comparing surgical techniques, so management remains opinion- and series-driven. Examiners reward candidates who can articulate these grey areas rather than quote a single dogmatic threshold.
Key Debates
| Controversy | Argument A | Argument B | Pragmatic position |
|---|---|---|---|
| Surgical threshold (% articular surface) | Operate at greater than 30-40% (subluxation risk) | Many 40-50% fragments are stable in flexion and do well with extension block | Decide on dynamic stability (stable arc), not the percentage alone |
| Extension block splinting vs pinning vs ORIF | Closed methods avoid surgical morbidity | Open fixation restores articular congruity in large/displaced fragments | Reserve open surgery for fragments that are reconstructable and unstable through the functional arc |
| Hemi-hamate vs volar plate arthroplasty | Hemi-hamate restores bony contour for greater than 50% defects | Volar plate arthroplasty avoids donor site, good for moderate defects | Choose by defect size, comminution and reconstructability |
| Dynamic external fixation | Allows early motion with ligamentotaxis | Pin-site morbidity and lower final arc in some series | Useful for comminuted, non-reconstructable patterns |
| Timing for chronic injuries | Early reconstruction limits contracture/arthritis | Selected chronic cases tolerate delayed reconstruction | Beyond ~3-6 weeks expect open treatment and counsel on stiffness |
What the literature does NOT settle
- No single articular-surface percentage reliably predicts instability; dynamic testing of the stable arc is more useful than any fixed cut-off.
- Comparative outcome data between hemi-hamate, volar plate arthroplasty, dynamic fixation and ORIF are retrospective and confounded by injury severity selection bias.
- Long-term hemi-hamate series show acceptable function but frequent radiographic osteoarthritis, so "good clinical outcome" does not equal "normal joint".
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Dorsal PIPJ Dislocation
"A goalkeeper presents with a swollen middle finger. Lateral X-ray shows a dorsal dislocation of the PIPJ with a small avulsion fracture at the base of the middle phalanx. Reduction was easy. How do you treat him?"
Scenario 2: Volar PIPJ Dislocation - Central Slip Injury
"A 28-year-old basketball player presents to the emergency department 2 hours after jamming his index finger. Examination shows the PIPJ held in slight flexion with the fingertip pointing volarly. Lateral X-ray confirms volar dislocation of the middle phalanx relative to the proximal phalanx. The ED resident asks you about the best treatment approach. What do you tell them?"
Scenario 3: Irreducible PIPJ Dislocation
"A 35-year-old presents with a dorsal PIPJ dislocation of his ring finger sustained 4 hours ago. Multiple attempts at closed reduction in the emergency department have failed. X-rays show the middle phalanx remains dorsally dislocated with the PIPJ joint surfaces parallel to each other rather than overlapping. There is no fracture. What is your assessment and management?"
MCQ Practice Points
Clinical Pearl
Q: What is the mechanism and treatment of dorsal PIP dislocation?
A: Mechanism: Hyperextension injury with axial load, disrupting the volar plate. Most common finger dislocation. Proximal phalanx displaces dorsally relative to middle phalanx. Reduction: Digital block, longitudinal traction with gentle flexion. Post-reduction: Assess stability through ROM; If stable to 30° flexion: Buddy taping with early mobilization. If unstable: Extension block splinting (blocking last 20-30° of extension) for 2-3 weeks, progressive extension.
Clinical Pearl
Q: What is a volar PIP dislocation and why is it more concerning than dorsal?
A: Volar PIP dislocation: Middle phalanx displaces volarly; Less common but higher complication rate. Mechanism: Rotatory force or direct blow to extended finger. Central slip disruption is common (risk of boutonniere deformity). Reduction often more difficult (may require open reduction). Post-reduction: Splint PIP in full extension for 6 weeks to protect central slip (opposite of dorsal dislocation protocol). Earlier mobilization risks boutonniere deformity.
Clinical Pearl
Q: What is an irreducible PIP dislocation and what causes it?
A: Irreducible dislocation: Cannot achieve closed reduction due to interposed tissue. Causes: Volar plate interposition (flips proximally, blocks reduction); FDP entrapment (tendon wraps around condyle); Lateral band interposition; Button-holing of condyle through volar plate. Clinical clue: Failed gentle reduction attempts, palpable block to reduction. Treatment: Open reduction through volar or dorsal approach, extraction of interposed tissue, volar plate repair.
Clinical Pearl
Q: How do you assess and manage PIP fracture-dislocations?
A: Assess stability: Lateral X-ray - measure percentage of volar articular surface (middle phalanx) fractured. Less than 30%: Usually stable after reduction - extension block splinting. 30-50%: Borderline stable - may require surgical fixation (hemihamate arthroplasty, volar plate arthroplasty, dynamic external fixator). Greater than 50%: Unstable, high subluxation risk - requires surgical stabilization. V-sign (incongruent joint on lateral view) indicates instability requiring intervention.
Clinical Pearl
Q: What is the treatment for MCP joint dislocation and what makes it complex?
A: Dorsal MCP dislocation: Proximal phalanx dorsal to metacarpal head. Simple: Reducible closed with wrist flexion, MCP hyperextension then flexion. Complex (irreducible): Volar plate interposition, often with metacarpal head button-holed through flexor tendons/lumbricals. Clinical sign: Skin puckering over MCP. Complex dislocation contraindication: Repeated forceful reduction attempts (can further tighten noose). Requires open reduction (dorsal or volar approach).
Guidelines, Registries & Global Practice
Global epidemiology:
- Finger and hand injuries are among the most common presentations to emergency and acute care worldwide; the PIPJ is the most frequently dislocated digital joint, with dorsal dislocation by far the commonest pattern.
- Peak incidence is in young, active adults; ball and contact sports (basketball, football/soccer, rugby, cricket, volleyball, handball) dominate the mechanism across regions.
- Most simple dorsal dislocations are reduced and managed by emergency physicians or primary care, with specialist hand referral reserved for volar dislocations, irreducible joints and fracture-dislocations.
Guidance & Principles Across Settings
| Theme | Common ground (AAOS / BOA / AO principles) | Practical note |
|---|---|---|
| First-line for stable dorsal | Closed reduction + early protected motion (buddy strapping / dorsal block splint) | Avoid prolonged rigid immobilisation |
| Volar dislocation | Treat as central slip injury: extension splinting ~6 weeks | Early flexion mobilisation causes boutonniere |
| Fracture-dislocation triage | Assess stable arc + fragment size on true lateral | No fixed percentage cut-off is universally endorsed |
| Local anaesthesia | Digital block with plain lidocaine for reduction | Document neurovascular status before and after |
| Rehabilitation | Early supervised hand therapy improves motion | Access varies by health system |
Registry and outcome notes: Unlike arthroplasty of large joints, finger dislocations are not tracked in national joint registries; the evidence base is institutional case series and systematic reviews rather than registry data, which is itself a recognised limitation.
High- vs limited-resource practice variation:
- High-resource settings: ready access to fluoroscopy, hand surgeons, dedicated hand therapy, and implants (suture anchors, mini-screws, dynamic fixators, hemi-hamate reconstruction).
- Limited-resource settings: emphasis on closed reduction, buddy strapping and improvised dynamic external fixation (for example a syringe-and-K-wire construct) which provides comparable function at minimal cost; early motion and patient education remain the highest-value, lowest-cost interventions everywhere.
References
Evidence verified against PubMed.
- Gianakos AL, Yingling J, Athens CM, Barra AE, Capo JT. Treatment for Acute Proximal Interphalangeal Joint Fractures and Fracture-Dislocations: A Systematic Review. J Hand Microsurg. 2020. PMID 33335365. doi:10.1055/s-0040-1713323
- Williams RM, Kiefhaber TR, Sommerkamp TG, Stern PJ. Treatment of unstable dorsal proximal interphalangeal fracture/dislocations using a hemi-hamate autograft. J Hand Surg Am. 2003;28(5):856-65. PMID 14507519. doi:10.1016/s0363-5023(03)00304-6
- Mazhar FN, Noei RR, Zareie B, et al. Long-Term Clinical and Radiological Results of Hemi-Hamate Arthroplasty for PIP Fracture Dislocation. J Hand Surg Am. 2026. PMID 41528296. doi:10.1016/j.jhsa.2025.11.020
- Fleury CM, Yousaf IS, Miles MR, et al. The Syringe External Fixator for Comminuted Intra-Articular Fractures of the Hand. J Hand Surg Am. 2021. PMID 34602335. doi:10.1016/j.jhsa.2021.07.036
- Pillukat T, Windolf J, Schadel-Hopfner M, Fuhrmann RA, van Schoonhoven J. Extensor tendon injuries at the level of the PIP joint. Unfallchirurg. 2021;124(4):265-274. PMID 33616682. doi:10.1007/s00113-021-00984-x
- Eaton RG, Malerich MM. Volar plate arthroplasty of the proximal interphalangeal joint (classic technique). J Hand Surg Am. 1980. (Classic reference)
- Kiefhaber TR, Stern PJ. Fracture-dislocations of the proximal interphalangeal joint: stability criteria. J Hand Surg Am. 1998. (Classic reference)
Finger Dislocation Quick Reference
Clinical summary
Direction
- •Dorsal: Volar plate injury → Early Motion
- •Volar: Central Slip injury → Splint Extension (6w)
Irreducible?
- •Volar Plate interposition
- •FDP tendon entrapment (rare)
- •Condyle buttonholing