Nine Compartments | Calcaneal Fracture Association | Fasciotomy Controversy | Claw Toe Sequelae
- Foot has nine distinct compartments separated by fascial septa
- Calcaneal fractures cause compartment syndrome in up to 10 percent of cases
- Clinical diagnosis relies on pain out of proportion and pain on passive stretch
- Fasciotomy versus delayed reconstruction remains controversial
- Untreated leads to intrinsic-minus claw toes and permanent stiffness
- “Always measure pressures in calcaneal fractures with tense swelling
- “Central calcaneal compartment contains the lateral plantar nerve
- “Late claw toes result from intrinsic muscle necrosis and fibrosis
- “Fasciotomy incisions must address all nine compartments
Nine compartments: medial, lateral, superficial central, calcaneal (deep central), four interosseous, and adductor hallucis compartment in some descriptions. The calcaneal compartment communicates with the deep posterior leg compartment via the tarsal tunnel.
Calcaneal fractures (especially joint-depression types) and Lisfranc fracture-dislocations produce marked swelling within rigid fascial boundaries. Crush injuries, high-energy axial loading, and tight casts also precipitate acute compartment syndrome.
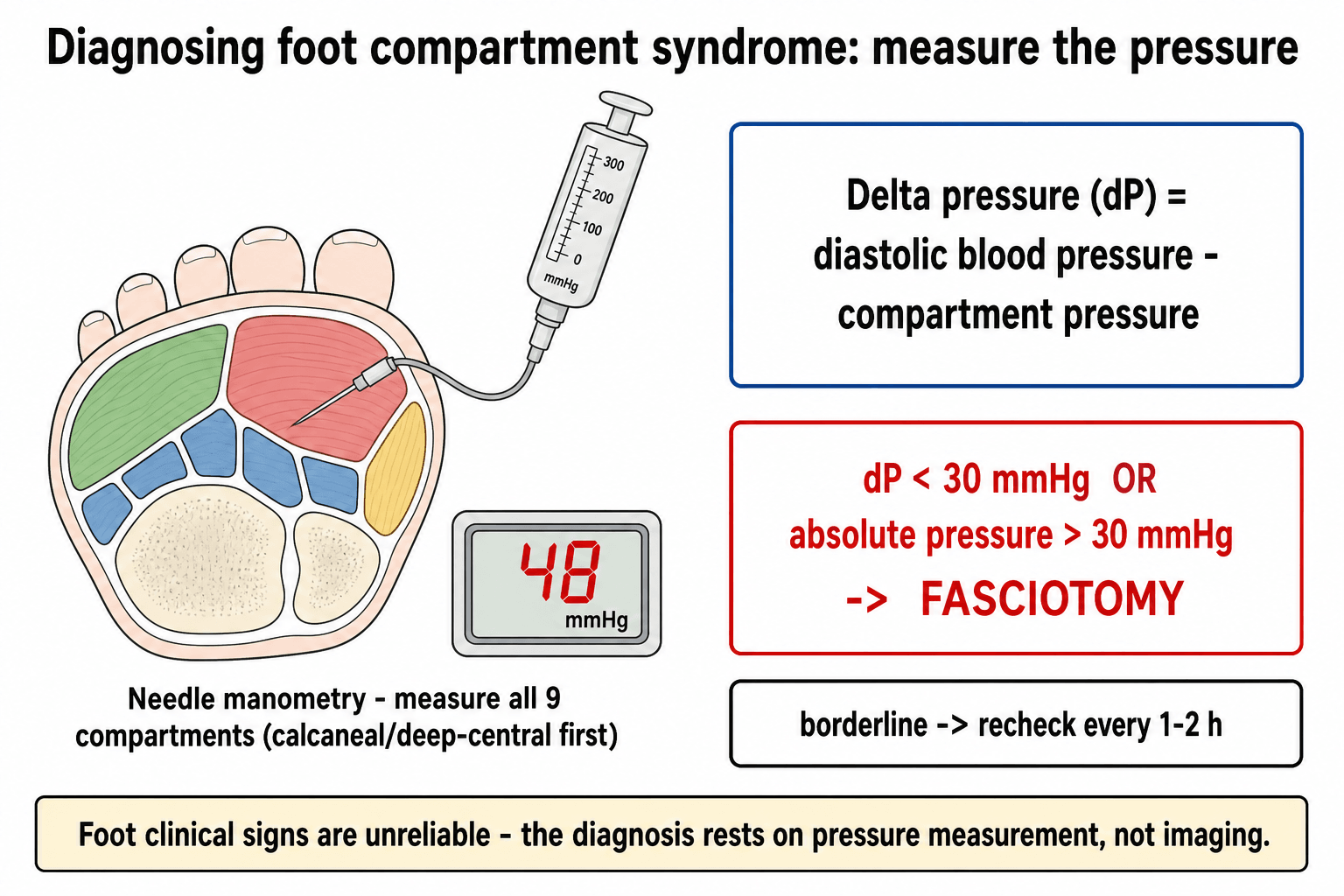
Absolute pressure greater than 30 mmHg or delta pressure (diastolic BP minus compartment pressure) less than 30 mmHg are commonly cited thresholds. Serial measurements every 1-2 hours are essential when clinical suspicion exists but pressures are borderline.
Early fasciotomy remains standard for confirmed acute compartment syndrome. However, many centres now favour selective fasciotomy with close monitoring because late reconstruction of claw toes and contractures can be performed electively with reasonable functional outcomes.
- Diagnosis
- Compartment pressure greater than 30 mmHg or delta P less than 30
- Treatment
- Urgent fasciotomy of all nine compartments
- Key Pearl
- Measure pressures before and after fracture fixation
- Diagnosis
- Pain on passive toe stretch, tense plantar arch
- Treatment
- Serial pressure monitoring, fasciotomy if thresholds met
- Key Pearl
- Central calcaneal compartment most commonly elevated
- Diagnosis
- Intrinsic muscle fibrosis, fixed deformities
- Treatment
- Delayed reconstruction: tendon transfers, osteotomies
- Key Pearl
- Prevent with early recognition in high-energy fractures
MLSCIAINine Foot Compartments
Hook:MLSCIAI - nine compartments that must all be released in foot compartment syndrome!
DELTA30Pressure Measurement Thresholds
Hook:DELTA30 guides fasciotomy decision - never rely on a single pressure reading!
Overview and Epidemiology
Foot compartment syndrome is a limb-threatening emergency that is frequently underdiagnosed in association with calcaneal fractures and Lisfranc injuries. The foot's nine rigid fascial compartments leave little room for swelling, and delayed diagnosis leads to irreversible muscle necrosis, intrinsic-minus claw toes, chronic pain, and in severe cases amputation. Early pressure measurement and timely fasciotomy remain the only means of preventing these sequelae, yet controversy persists regarding the necessity of fasciotomy in every case meeting pressure thresholds.
- Calcaneal fractures: Axial loading produces massive swelling within the calcaneal and central compartments
- Lisfranc fracture-dislocations: Tarsometatarsal disruption causes bleeding into multiple interosseous and central compartments
- Crush injuries: Industrial or motor-vehicle trauma directly compresses the plantar compartments
- Tight casting: Circumferential casts applied to swollen feet create iatrogenic compartment syndrome
- High-energy axial load: Falls from height or motorcycle accidents
- Muscle necrosis: Intrinsic muscles die within 4-6 hours of critical ischaemia
- Claw toe deformity: Fibrosis of intrinsics produces intrinsic-minus posture
- Chronic pain: Persistent plantar neuropathic pain from nerve compression
- Stiffness: Global foot rigidity limits gait and shoe wear
- Amputation: Up to 10 percent of severe untreated cases progress to below-knee amputation
Pathophysiology
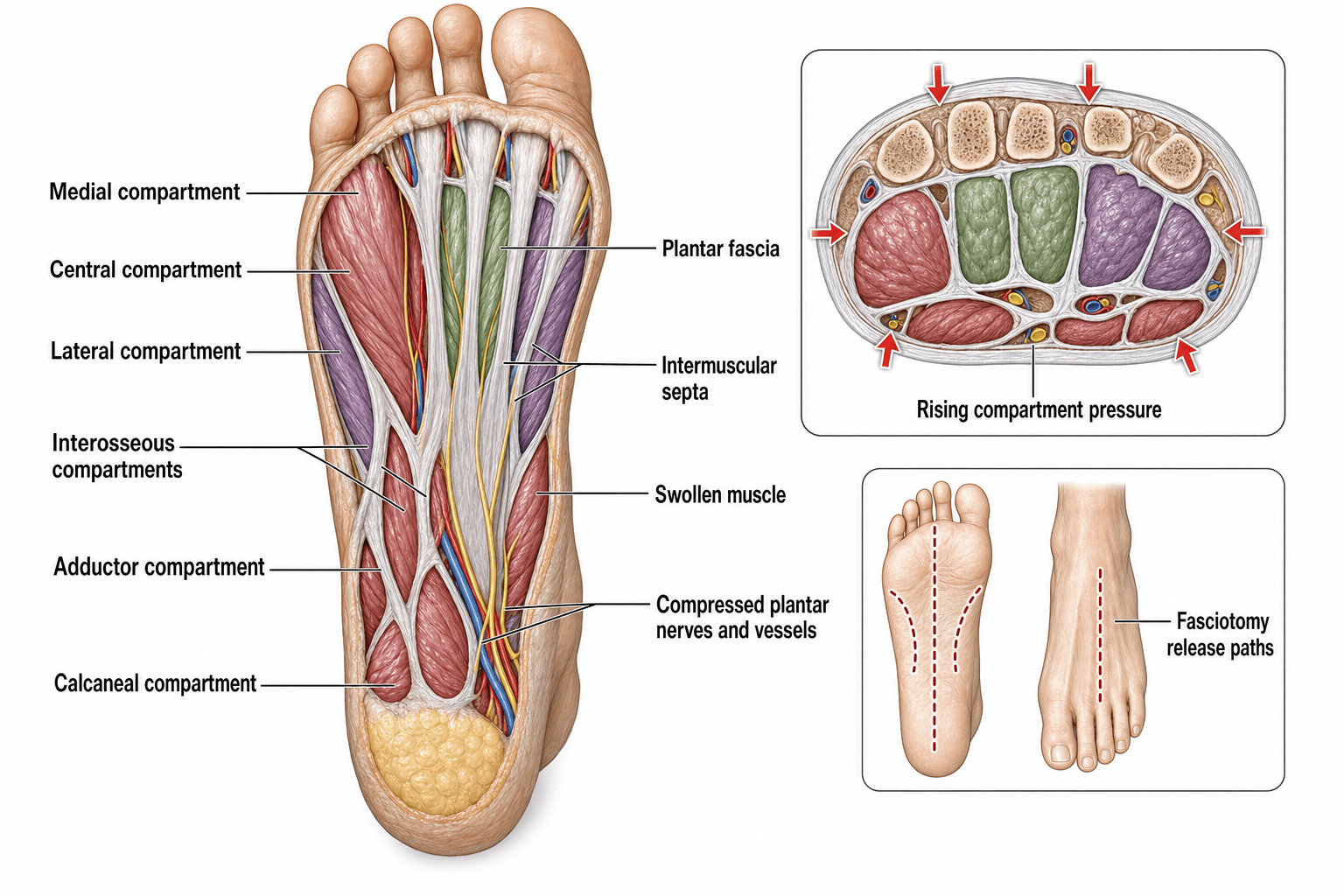
The foot is divided into nine distinct compartments by tough fascial septa arising from the plantar aponeurosis and intermetatarsal ligaments. The medial compartment contains abductor hallucis. The lateral compartment houses abductor digiti minimi. The central compartment is subdivided into superficial (flexor digitorum brevis) and deep calcaneal (quadratus plantae and lateral plantar neurovascular bundle) layers. Four separate interosseous compartments exist between the metatarsals, and the adductor hallucis occupies its own transverse and oblique head compartment. The calcaneal compartment communicates proximally with the deep posterior compartment of the leg through the tarsal tunnel, allowing pressure transmission in both directions.
- Key Structures
- Abductor hallucis, medial plantar nerve
- Clinical Consequence if Necrotic
- Loss of great toe abduction, medial foot pain
- Release Incision
- Medial hindfoot incision
- Key Structures
- Abductor digiti minimi, lateral plantar nerve branch
- Clinical Consequence if Necrotic
- Little toe abduction loss, lateral foot pain
- Release Incision
- Lateral hindfoot incision
- Key Structures
- Quadratus plantae, lateral plantar nerve and vessels
- Clinical Consequence if Necrotic
- Intrinsic-minus clawing, plantar numbness
- Release Incision
- Plantar central deep release
- Key Structures
- Dorsal and plantar interossei, metatarsal arteries
- Clinical Consequence if Necrotic
- Metatarsal head necrosis, web-space pain
- Release Incision
- Dorsal intermetatarsal incisions
Normal resting pressure: 0-8 mmHg Critical ischaemia threshold: compartment pressure greater than 30 mmHg or delta pressure less than 30 mmHg for greater than 4-6 hours Calcaneal fractures: pressures often exceed 40-60 mmHg within the calcaneal compartment due to bleeding from the bone and surrounding soft tissues Lisfranc injuries: interosseous and central compartments most affected by haemorrhage tracking along the tarsometatarsal joints
Rigid fascial boundaries: nine separate envelopes with minimal compliance Dependent position: gravity increases hydrostatic pressure in the foot Limited collateral flow: single dominant posterior tibial artery contribution Communication with leg: tarsal tunnel allows pressure to rise from leg compartments or transmit distally Small volume: even modest bleeding produces rapid pressure elevation
Mechanism of Ischaemia: The Arteriovenous Gradient
A core basic-science point the rest of the topic assumes: compartment syndrome does not cause ischaemia by occluding the main arteries. The pathology is at the capillary level.
- Rising interstitial (tissue) pressure within the rigid fascial envelope first collapses the thin-walled veins, obstructing venous outflow. This raises venous pressure and reduces the local arteriovenous (AV) pressure gradient that drives capillary perfusion.
- As the gradient falls, capillary perfusion fails and the tissue becomes hypoxic - a self-amplifying cycle, because congestion raises pressure further.
- The large arteries carry a far higher pressure, so distal pulses are typically preserved until very late. Palpable dorsalis pedis and posterior tibial pulses therefore do NOT exclude compartment syndrome - a classic trap.
- This is why the delta (perfusion) pressure - diastolic blood pressure minus compartment pressure - is used: perfusion fails as tissue pressure rises towards diastolic, so a delta under 30 mmHg signals critical hypoperfusion even with a normal systolic pressure and present pulses.
Compartment syndrome is a capillary perfusion failure from a collapsed arteriovenous gradient (venous outflow obstruction), not large-artery occlusion - so pulses and capillary refill are normal until late. Never be reassured by a palpable pulse. The delta pressure (diastolic minus compartment, under 30 mmHg) captures this perfusion deficit better than the absolute pressure alone.
Classification and Types
Classification by Associated Injury
- Compartment Risk
- Calcaneal and central compartments highest
- Typical Pressures
- Often greater than 40 mmHg
- Fasciotomy Rate
- Up to 10 percent require fasciotomy
- Compartment Risk
- Interosseous and central compartments
- Typical Pressures
- 30-50 mmHg common
- Fasciotomy Rate
- Selective, 5-15 percent
- Compartment Risk
- Multiple compartments simultaneously
- Typical Pressures
- Variable, often all nine elevated
- Fasciotomy Rate
- High fasciotomy rate
- Compartment Risk
- Global elevation possible
- Typical Pressures
- Reversible if cast removed early
- Fasciotomy Rate
- Rare if recognised promptly
High-energy calcaneal fractures remain the strongest predictor of foot compartment syndrome and should trigger routine pressure monitoring in the first 24-48 hours.
Clinical Assessment
- Mechanism: High-energy axial load, calcaneal fracture, Lisfranc injury, crush
- Timing: Onset of severe pain relative to injury or cast application
- Pain character: Deep, burning, out of proportion to visible injury
- Analgesia requirement: Escalating opioid needs despite fracture stabilisation
- Sensory change: Numbness in plantar distribution (lateral plantar nerve)
- Inspect: Tense, shiny plantar skin, loss of skin wrinkles, massive swelling
- Palpate: Rock-hard compartments, especially calcaneal and central
- Passive stretch: Severe pain on passive toe flexion or extension (most sensitive sign)
- Active movement: Weak or absent intrinsic function
- Neurologic: Diminished plantar sensation, two-point discrimination greater than 6 mm
- Vascular: Dorsalis pedis and posterior tibial pulses usually preserved until late
Technique: Stabilise the ankle and gently extend or flex the toes while observing patient response. Pain out of proportion or disproportionate guarding indicates rising compartment pressure. Interpretation: Positive in greater than 90 percent of confirmed cases before neurologic deficit appears. Pitfall: In the multiply injured or sedated patient this sign may be masked; rely on pressure measurement and serial examination. Key point: Never wait for the five P's (pain, pallor, paraesthesia, paralysis, pulselessness) - these are late, irreversible signs.
- Distinguishing Feature
- Pain on passive stretch, tense compartments
- Pressure Measurement
- Elevated greater than 30 mmHg or delta less than 30
- Management Difference
- Fasciotomy of all nine compartments
- Distinguishing Feature
- Heel pain, swelling, no disproportionate pain
- Pressure Measurement
- Normal or mildly elevated
- Management Difference
- Fracture management, elevation, monitoring
- Distinguishing Feature
- Erythema, warmth, systemic signs
- Pressure Measurement
- Normal pressures
- Management Difference
- Antibiotics, possible drainage
- Distinguishing Feature
- Calf swelling, Homan sign positive
- Pressure Measurement
- Normal foot pressures
- Management Difference
- Anticoagulation, vascular consult
Investigations
Diagnostic Protocol
Indications: Any calcaneal fracture with tense swelling, Lisfranc injury with severe pain, crush injury, or clinical suspicion. Technique: Use a handheld manometer or arterial-line transducer. Measure all nine compartments through separate needle insertions. Record absolute pressure and calculate delta pressure using diastolic blood pressure. Thresholds: Absolute pressure greater than 30 mmHg or delta pressure less than 30 mmHg warrants strong consideration of fasciotomy. Serial measurements every 1-2 hours if borderline.
Views: AP, lateral, oblique, and Harris heel views of the foot and ankle. Purpose: Identify calcaneal fracture pattern (Essex-Lopresti or Sanders classification), Lisfranc displacement, or other bony injury that may require fixation in the same sitting as fasciotomy. Clinical correlation: Fracture classification does not predict compartment pressures; measure pressures regardless of fracture type.
CT: Useful for surgical planning of calcaneal fracture fixation after fasciotomy decision is made. MRI: Rarely required acutely; may show muscle oedema but delays intervention and is not used for diagnosis of compartment syndrome. Key point: Imaging confirms the fracture but the diagnosis of compartment syndrome is made by pressure measurement and clinical correlation.
Always measure the calcaneal (deep central) compartment first in calcaneal fractures - it is the most commonly elevated and contains the lateral plantar nerve. If pressures are borderline, repeat after 30-60 minutes of observation or after fracture reduction. Document both absolute and delta pressures in the notes before proceeding to fasciotomy.
Management Algorithm
Acute Compartment Syndrome Requiring Fasciotomy
Goal: Release all nine compartments through minimal incisions while protecting neurovascular structures and allowing subsequent fracture fixation.
Surgical Protocol
Position: Supine with bump under ipsilateral hip, foot at end of table. Tourniquet: Use only if needed for fracture fixation; avoid prolonged tourniquet time before fasciotomy. Equipment: Handheld manometer confirmation in theatre, fine scissors, retractors, skin-marking pen.
Medial incision: 6 cm incision along medial foot from navicular to calcaneal tuberosity, releasing medial and superficial central compartments. Lateral incision: 6 cm incision along lateral foot parallel to plantar surface, releasing lateral and interosseous compartments. Plantar central: Connect or separate incision to release calcaneal (deep) compartment and protect lateral plantar nerve. Dorsal intermetatarsal: Two or three dorsal incisions between metatarsals to release all four interosseous compartments and adductor hallucis.
Complete fascial division: Ensure each compartment is fully released from proximal to distal. Protect neurovascular bundles: Identify and preserve medial and lateral plantar nerves during central compartment release. Debride necrotic muscle: Any obviously dead muscle should be excised at the index procedure. Leave wounds open: Plan for delayed primary closure or skin grafting at 5-7 days.
Elevation: Strict elevation for 48 hours to reduce oedema. Wound care: Negative-pressure dressing or moist gauze, return to theatre in 48-72 hours for inspection and possible closure. Fracture fixation: Perform ORIF of calcaneal or Lisfranc injury once swelling allows, usually 7-14 days later. Rehabilitation: Early active toe motion, progressive weight-bearing once wounds stable.
The calcaneal compartment must be released through a separate deep plane because it lies beneath the superficial central compartment. Failure to release the calcaneal compartment leaves the quadratus plantae and lateral plantar nerve compressed, resulting in persistent clawing and plantar numbness despite release of the other eight compartments.
CLAWTOELate Sequelae Management
Hook:CLAWTOE reminds you of the devastating late consequences of missed foot compartment syndrome!
Complications
Complications arise both from a missed or late-treated compartment syndrome (ischaemic sequelae) and from the fasciotomy required to treat it.
- Claw-toe deformity of the lesser toes - the hallmark late deformity, from ischaemic contracture of the intrinsic (interosseous and lumbrical) muscles
- Fixed cavus / clawing and forefoot deformity with painful, stiff toes
- Sensory loss and dysaesthesia in the medial and lateral plantar nerve distributions
- Chronic pain, weakness and stiffness with difficulty in push-off and shoe wear
- Open wounds requiring delayed closure or split-skin grafting, with attendant scarring
- Wound infection and dehiscence, especially with associated open fractures
- Incomplete release - missing the deep calcaneal compartment is a classic cause of persistent ischaemia and ongoing deformity
- Need to delay calcaneal ORIF until fasciotomy wounds heal, prolonging recovery
The deep calcaneal compartment is the most frequently elevated and the most commonly under-released compartment. An apparently "complete" fasciotomy that misses it can still leave the patient with ischaemic clawing - which is why the medial (Henry) approach, which reliably reaches the calcaneal compartment, is emphasised.
Systemic Sequelae: Rhabdomyolysis and Reperfusion
The foot is small, but extensive or crush-related muscle necrosis - and the reperfusion that follows fasciotomy or restored flow - can cause systemic harm that the local picture hides.
- Ischaemic and necrotic muscle releases myoglobin, potassium, phosphate and creatine kinase when reperfused. This is rhabdomyolysis; with a large enough muscle load it becomes crush syndrome.
- The dangers are hyperkalaemia (arrhythmia, cardiac arrest), myoglobinuric acute kidney injury (pigment nephropathy), metabolic acidosis and hypocalcaemia.
- Monitor creatine kinase, urea and electrolytes, and an ECG; check the urine for myoglobin (tea-coloured urine that is dipstick-positive for blood without red cells).
- Management is aggressive intravenous crystalloid to maintain a brisk urine output, prompt treatment of hyperkalaemia, and renal support if acute kidney injury develops (urinary alkalinisation is sometimes used but is debated).
Necrotic muscle reperfused after fasciotomy or restored flow releases potassium and myoglobin - causing hyperkalaemia (arrhythmia) and myoglobinuric acute kidney injury. Check CK, urea and electrolytes and an ECG, give generous IV fluids to protect the kidneys, and treat hyperkalaemia urgently. This systemic risk is one reason very late fasciotomy of frankly necrotic muscle is approached with caution - debriding dead muscle may be safer than reperfusing it.
Outcomes and Prognosis
- Muscle Viability
- Greater than 90 percent viable
- Claw Toe Rate
- Less than 10 percent
- Return to Work
- 80-90 percent at 3-6 months
- Muscle Viability
- 70-80 percent viable
- Claw Toe Rate
- 20-30 percent
- Return to Work
- 60-70 percent at 6 months
- Muscle Viability
- Less than 50 percent viable
- Claw Toe Rate
- Greater than 70 percent
- Return to Work
- Less than 40 percent, many require late surgery
Best prognosis: Early diagnosis (less than 6 hours), complete nine-compartment release, young patient, low-energy mechanism, compliant rehabilitation. Poor prognosis: Delayed presentation (greater than 24 hours), incomplete release (especially calcaneal compartment), high-energy crush, associated open fracture or vascular injury, smoking, diabetes. Key threshold: 6 hours from onset of critical pressure elevation - muscle necrosis becomes irreversible beyond this window in most patients.
Guidelines, Registries & Global Practice
- Calcaneal fractures account for 1-2 percent of all fractures worldwide and are the leading cause of foot compartment syndrome
- Incidence of compartment syndrome after calcaneal fracture ranges from 4-10 percent in published series across trauma centres
- High-energy axial loading mechanisms predominate in industrial and motor-vehicle settings globally
- Missed diagnosis remains a significant source of litigation in foot and ankle trauma worldwide
- High-resource centres: routine pressure monitoring with handheld manometers, dedicated foot and ankle trauma lists, negative-pressure wound therapy for open fasciotomy wounds
- Limited-resource settings: reliance on clinical signs and serial examination, improvised fasciotomy incisions, delayed wound closure with skin grafts when available
- Universal principle: outcome depends on early recognition and complete release of all nine compartments regardless of available technology
- Surgery: late reconstruction expertise is concentrated in specialist foot and ankle units globally
- Diagnosis emphasis
- Pressure measurement in all high-risk calcaneal and Lisfranc injuries
- Acute treatment
- Fasciotomy when absolute greater than 30 mmHg or delta less than 30 mmHg
- Late reconstruction
- Tendon transfers and osteotomies for established claw toes
- Diagnosis emphasis
- High index of suspicion, serial clinical examination, selective pressure measurement
- Acute treatment
- Early fasciotomy for confirmed cases, close monitoring for borderline
- Late reconstruction
- Multidisciplinary foot and ankle reconstruction pathways
- Diagnosis emphasis
- Compartment pressure monitoring as standard in calcaneal fracture protocols
- Acute treatment
- Complete nine-compartment release through described incisions
- Late reconstruction
- Staged reconstruction after soft-tissue recovery
- Diagnosis emphasis
- Awareness of tarsal tunnel communication with leg compartments
- Acute treatment
- Individualised decision-making integrating pressure and clinical data
- Late reconstruction
- Emphasis on prevention and early referral to specialist units
No dedicated international registry tracks foot compartment syndrome outcomes. Evidence is derived from small prospective series and expert consensus. The trend toward selective rather than routine fasciotomy reflects recognition that many patients with moderately elevated pressures recover without surgery, while those who develop fixed claw toes can still achieve useful function with delayed reconstruction. Documentation of pressure measurements and clinical rationale for or against fasciotomy is essential for medicolegal protection worldwide.
Controversies & Areas of Uncertainty
Absolute pressure thresholds (greater than 30 mmHg) have driven routine fasciotomy in many centres, yet recent series suggest selective monitoring is safe when delta pressure remains above 25-30 mmHg and clinical signs are improving. No randomised trial exists to settle the question.
Classic teaching requires four separate incisions to release all nine compartments reliably. Some surgeons advocate three-incision techniques with acceptable release rates, but cadaveric studies show incomplete deep central release when incisions are minimised.
Indwelling catheter systems provide continuous readings but add cost, infection risk, and potential for measurement error. Intermittent handheld manometry remains the global standard; no high-quality evidence demonstrates superiority of continuous systems in the foot.
Traditional teaching delays ORIF 7-14 days until swelling subsides. Some centres now perform acute fixation at the time of fasciotomy using minimally invasive techniques, but wound complication rates and long-term outcomes require further study.
MCQ Practice Points
Q: How many compartments does the foot have and which is most clinically important in calcaneal fractures? A: The foot has nine compartments. The calcaneal (deep central) compartment is most clinically important in calcaneal fractures because it contains the quadratus plantae and the lateral plantar neurovascular bundle; its release is frequently incomplete if not specifically addressed through a deep plane.
Q: What are the pressure thresholds for fasciotomy in foot compartment syndrome? A: Absolute compartment pressure greater than 30 mmHg or delta pressure (diastolic blood pressure minus compartment pressure) less than 30 mmHg. Serial measurements are essential when values are borderline, and the decision integrates both pressure data and clinical signs.
Q: What late deformity occurs if foot compartment syndrome is missed? A: Intrinsic-minus claw toe deformity. Necrosis of the intrinsic muscles (especially quadratus plantae and interossei) removes their opposition to the long flexors and extensors, producing hyperextension at the metatarsophalangeal joints and flexion at the interphalangeal joints.
Q: What incisions are required for complete nine-compartment release? A: Medial hindfoot incision (medial and superficial central compartments), lateral hindfoot incision (lateral and interosseous compartments), separate deep central release for the calcaneal compartment, and two to three dorsal intermetatarsal incisions for the four interosseous compartments and adductor hallucis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old roofer falls 4 metres onto his right heel. He has a closed Sanders type III calcaneal fracture with massive foot swelling. Six hours after injury he complains of severe burning plantar pain despite opioid analgesia. The foot is tense, especially over the medial arch. What is your assessment and management?”
“A 35-year-old man sustained a crush injury to his foot 8 weeks ago that was treated non-operatively elsewhere. He now presents with fixed clawing of all lesser toes, loss of plantar sensation, and inability to wear normal shoes. The foot is stiff and painful. How would you manage this?”
Key Anatomy
- Nine compartments: medial, lateral, superficial central, calcaneal (deep central), four interosseous, adductor hallucis
- Calcaneal compartment contains quadratus plantae and lateral plantar neurovascular bundle
- Tarsal tunnel communication allows pressure transmission between leg and foot
- Intrinsic muscles (especially quadratus plantae) are critical for toe balance
Diagnosis
- Pain out of proportion and pain on passive toe stretch are most sensitive clinical signs
- Pressure thresholds: absolute greater than 30 mmHg or delta (diastolic minus compartment) less than 30 mmHg
- Measure all nine compartments serially when suspicion exists
- Calcaneal fractures and Lisfranc injuries carry highest risk
Treatment Algorithm
- Acute confirmed compartment syndrome: urgent nine-compartment fasciotomy
- Medial, lateral, plantar central, and dorsal intermetatarsal incisions required
- Selective monitoring acceptable in borderline cases with close observation
- Late claw toes treated with FHL transfer, osteotomies, and joint fusions
Critical Thresholds
- Absolute pressure greater than 30 mmHg = consider fasciotomy
- Delta pressure less than 30 mmHg = consider fasciotomy
- Time window for reversible muscle ischaemia approximately 4-6 hours
- Delayed presentation (greater than 24 hours) shifts focus to late reconstruction
Sequelae & Prevention
- Missed compartment syndrome produces intrinsic-minus claw toe deformity
- Late reconstruction improves but rarely normalises function
- Best outcome achieved by early recognition and complete release
- Always document pressure measurements and clinical rationale in high-risk fractures
Evidence Base and Key Trials
Compartment syndromes of the foot after calcaneal fractures
- Approximately 10% of calcaneal fractures develop a foot compartment syndrome, and about half of those go on to clawing of the lesser toes, stiffness and neurovascular dysfunction
- Tense swelling and severe pain are the hallmarks; diagnosis confirmed by multistick catheterisation, particularly of the calcaneal compartment in the hindfoot
- Recommended immediate fasciotomy to prevent ischaemic contracture, with calcaneal ORIF delayed until the fasciotomy wounds are closed
Experimental decompression of the fascial compartments of the foot--the basis for fasciotomy in acute compartment syndromes
- In 40 paired fresh cadaver feet, compared a double-incision dorsal fasciotomy with a single medial longitudinal approach using slit-catheter pressure monitoring
- Both approaches satisfactorily decompressed the compartments, but pressures normalised more slowly after the dorsal approach (11 min vs 1 min, p<0.01)
- The double-incision dorsal approach is easier to perform and may be preferred when forefoot fractures also require internal fixation
Foot compartment syndrome
- Review of diagnosis and management emphasizing clinical signs and pressure thresholds
- Highlighted calcaneal compartment as most frequently elevated in trauma
Compartment syndrome of the foot after calcaneal fracture
- Case report of compartment syndrome following calcaneal fracture
- Stressed importance of early recognition and fasciotomy in emergency setting