Regenerating Bone, Cartilage and Tendon
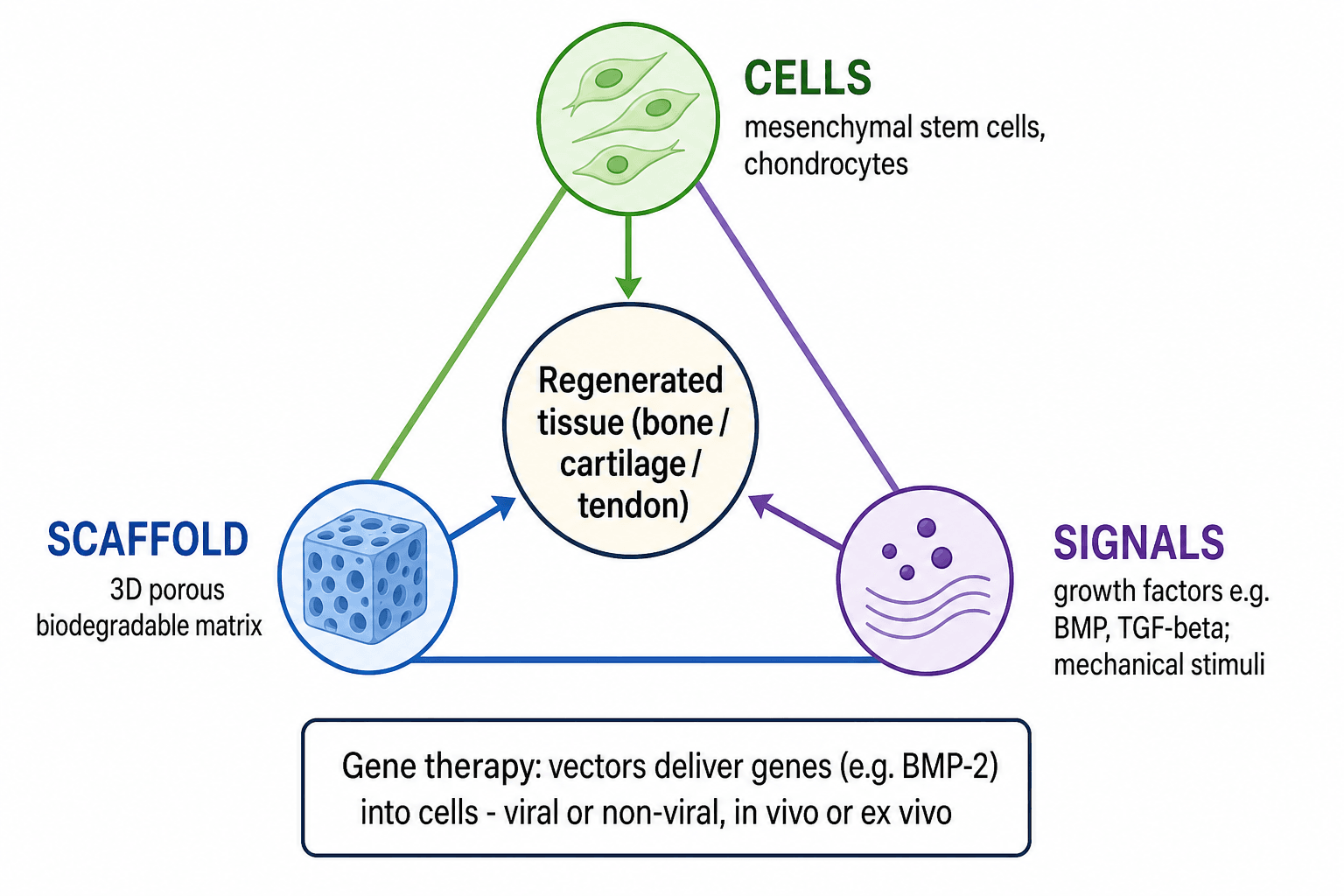
- TISSUE ENGINEERING aims to regenerate musculoskeletal tissue using a TRIAD (the 'tissue-engineering triangle'): (1) CELLS - most often MESENCHYMAL STEM CELLS (from marrow or adipose) or differentiated cells such as chondrocytes/osteoblasts; (2) a SCAFFOLD - a 3D, porous, biodegradable matrix (natural like collagen/hyaluronan/hydrogels, or synthetic like PLGA/PCL/ceramics/nanofibres) that is osteoconductive and guides tissue formation; and (3) SIGNALS - growth factors (BMPs, TGF-beta, PDGF, VEGF) and mechanical stimuli that direct differentiation.
- The established CLINICAL example is AUTOLOGOUS CHONDROCYTE IMPLANTATION (ACI/MACI), where the patient's own chondrocytes are expanded and re-implanted (on a membrane in MACI) to repair cartilage defects; recombinant BMP-2/BMP-7 (delivered on a collagen carrier) is used clinically in spinal fusion and tibial nonunion - examples of the signals/scaffold approach (recombinant protein, not gene therapy).
- GENE THERAPY delivers a GENE encoding a therapeutic protein (e.g. BMP-2/7 for bone, IGF-1/TGF-beta for cartilage, anti-inflammatory genes for osteoarthritis) into cells so they MANUFACTURE the protein, giving more SUSTAINED local expression than a single dose of recombinant protein.
- Gene delivery uses VECTORS that are VIRAL (adenovirus, adeno-associated virus, lentivirus/retrovirus) - EFFICIENT but with safety concerns (immunogenicity; insertional mutagenesis with integrating retro/lentiviruses) - or NON-VIRAL (plasmid DNA, lipofection) - SAFER but LESS efficient; the gene can be delivered IN VIVO (vector applied directly to the site) or EX VIVO (cells harvested, genetically modified, then re-implanted, often on a 'gene-activated matrix').
- CHALLENGES limit translation: vector SAFETY (immune response to viral vectors, insertional mutagenesis, controlled/sustained but not unlimited expression), VASCULARISATION of large constructs, achieving the right cell-scaffold-signal combination, manufacturing/scale-up, COST and regulatory hurdles - so most gene therapy and large-scale tissue engineering remain EXPERIMENTAL/preclinical.
- Practically, regenerative orthopaedics today is a spectrum: ACI/MACI and recombinant BMP carriers are in clinical use, orthobiologics (PRP, marrow concentrate) are used adjunctively, while gene therapy and engineered whole-tissue constructs are mostly investigational - candidates should understand the principles and the gap between promise and current clinical reality.
- “Tissue-engineering TRIAD = cells (MSCs/chondrocytes) + scaffold (porous biodegradable matrix) + signals (BMP/TGF-beta, mechanical).
- “Established clinical examples: ACI/MACI (cartilage); recombinant BMP-2/7 on collagen carrier (spine fusion, tibial nonunion).
- “Gene therapy: viral (efficient, safety concerns) vs non-viral (safer, less efficient); in vivo vs ex vivo (gene-activated matrix). Mostly experimental - vector safety, vascularisation, cost.
Cells + Scaffold + Signals. Established example: ACI/MACI (cartilage); recombinant BMP on a collagen carrier (fusion/nonunion).
Viral (efficient, safety concerns) vs non-viral (safer, less efficient); in vivo (direct) vs ex vivo (modify cells then re-implant). Mostly experimental.
The Tissue-Engineering Triad
Tissue engineering combines three elements to regenerate tissue. CELLS provide the regenerative capacity - mesenchymal stem cells from marrow or adipose tissue (multipotent, can become bone/cartilage/fat) or differentiated chondrocytes/osteoblasts. The SCAFFOLD is a 3D, porous, biodegradable matrix that supports cell attachment and guides new-tissue architecture - natural materials (collagen, hyaluronan, hydrogels) or synthetic polymers/ceramics (PLGA, PCL, calcium phosphates, nanofibres) - ideally osteoconductive and resorbing as new tissue forms. SIGNALS instruct the cells - growth factors such as the BMPs (osteoinductive), TGF-beta (chondrogenic), PDGF and VEGF - together with mechanical stimulation (and bioreactors in the lab). Getting the right combination, and vascularising larger constructs, is the central engineering challenge.
From Bench to Clinic
- Autologous chondrocyte implantation (ACI/MACI): the patient's chondrocytes are harvested, expanded and re-implanted into a cartilage defect (in MACI seeded on a collagen membrane) - the established clinical example of cell-based tissue engineering.
- Recombinant BMPs: BMP-2 and BMP-7 delivered on a collagen carrier are used clinically for spinal fusion and tibial nonunion (a signals-plus-scaffold approach using recombinant protein, not a gene).
- Orthobiologics: PRP, bone-marrow aspirate concentrate and demineralised bone matrix are used adjunctively (see our Orthobiologics topic).
- Investigational: engineered bone/cartilage/meniscus/tendon constructs and gene therapy remain largely preclinical or early-clinical.
Gene Therapy Principles
Gene therapy delivers a gene encoding a therapeutic protein into cells so they produce the protein themselves, giving more sustained local expression than a single dose of recombinant protein. Targets include BMP-2/7 (bone), IGF-1/TGF-beta (cartilage) and anti-inflammatory genes (osteoarthritis).
- Vectors - viral vs non-viral: VIRAL vectors (adenovirus, adeno-associated virus, lentivirus/ retrovirus) are efficient but carry safety concerns (immunogenicity; insertional mutagenesis with integrating retro/lentiviruses). NON-VIRAL vectors (plasmid DNA, lipofection) are safer but less efficient.
- Strategy - in vivo vs ex vivo: IN VIVO delivers the vector directly to the target site; EX VIVO harvests the patient's cells, modifies them genetically, then re-implants them - often on a scaffold as a gene-activated matrix.
Translation is limited by vector safety (immune reactions to viral vectors, the risk of insertional mutagenesis with integrating vectors, and achieving controlled, sustained but not uncontrolled expression), the difficulty of vascularising large engineered constructs, the challenge of selecting the right cell- scaffold-signal combination, and manufacturing, cost and regulatory hurdles. Candidates should know the principles and be honest that, apart from ACI/MACI and recombinant BMP carriers, most gene therapy and whole-tissue engineering in orthopaedics is investigational rather than routine practice.
What Makes a Good Scaffold: The Design Requirements
- Biocompatibility: no toxic or excessive immune reaction, and non-toxic degradation by-products (a recognised weakness of PLGA, whose acidic by-products can cause local inflammation).
- Porosity and interconnected architecture: high porosity with interconnected pores (broadly around 100 to 500 microns) to allow cell migration, matrix deposition and - critically - vascular ingrowth.
- Matched mechanical properties: stiffness/strength close to the host tissue, able to bear or share load during healing without stress-shielding or collapsing.
- A degradation rate matched to new-tissue formation: the scaffold should resorb as tissue forms - degrade too fast and it loses support before the tissue matures, too slow and it impedes remodelling.
- Surface for cells, and able to carry signals: an osteoconductive surface chemistry/topography for attachment, proliferation and differentiation, ideally functionalised with growth factors or genes (a growth-factor-loaded or gene-activated matrix). (The osteoconduction/osteoinduction/osteogenesis framework is developed in our Bone Grafts topic.)
- Manufacturable and reproducible: scalable, sterilisable, and increasingly 3D-printed to a patient-specific geometry.
An ideal scaffold is biocompatible (non-toxic degradation by-products), highly and interconnectedly porous (around 100 to 500 microns for cells and vessels), mechanically matched to the host, with a degradation rate matched to new-tissue formation, an osteoconductive cell-friendly surface that can carry signals (gene-activated matrix), and is reproducibly manufacturable/3D-printable.
The Central Bottleneck: Vascularising the Construct
- The diffusion limit: cells survive only within roughly 150 to 200 microns of a capillary (the oxygen/nutrient diffusion distance), so beyond that distance the core of a thick construct becomes hypoxic and necrotic. This is why thin, relatively avascular tissues (cartilage) are far easier to engineer than thick, vascular ones (a large bone segment), and why large constructs fail without a blood supply.
- Strategies to overcome it: load the scaffold with angiogenic growth factors (VEGF, with PDGF for vessel maturation); pre-vascularise in vitro by co-culturing endothelial cells to form capillary networks before implantation; design scaffold architecture with channels and high interconnected porosity to invite host-vessel ingrowth; use bioreactor perfusion to nourish the construct during culture; and the in vivo "bioreactor"/prefabrication approach - implant the construct around a vascular pedicle (or in a well-vascularised bed) to vascularise it before transfer, or use a vascularised flap/free transfer surgically.
- The corollary: matching the scaffold's pore architecture and angiogenic signalling to the host's capacity to grow vessels in is as important as the cells and the growth factors themselves.
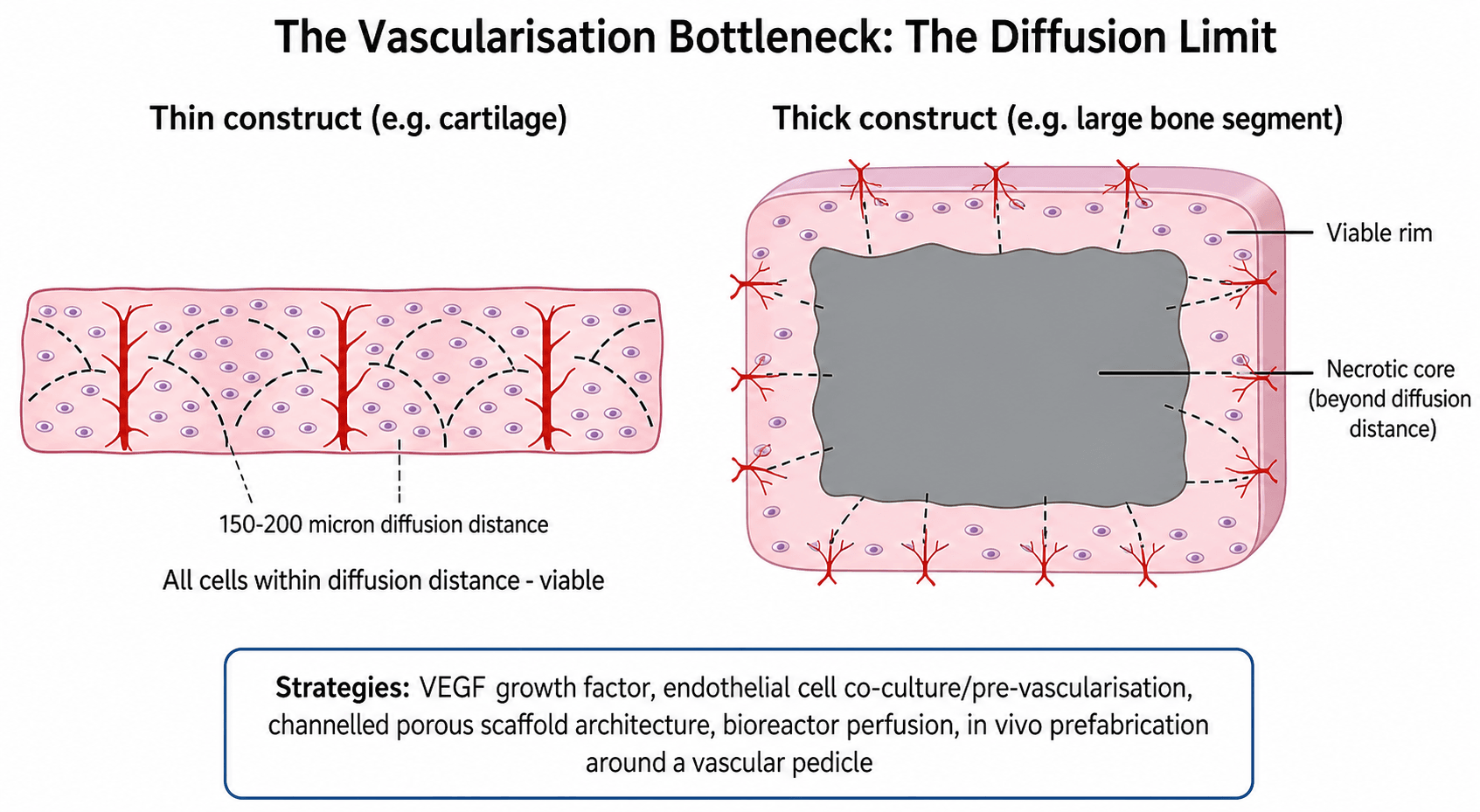
Cells survive only within about 150 to 200 microns of a capillary, so the core of a thick engineered construct goes necrotic without a blood supply - the reason big bone constructs fail while thin cartilage is easier. Overcome it with VEGF, endothelial co-culture/pre-vascularisation, channelled porous architecture, bioreactor perfusion, and in vivo prefabrication around a vascular pedicle.
Mnemonics & Memory Aids
CSS
Hook:Tissue engineering = CSS: Cells, Scaffold, Signals.
VECTOR
Hook:Gene therapy choices and challenges = VECTOR.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the tissue-engineering triad, and what is actually used clinically in orthopaedics?”
“What is gene therapy, how can genes be delivered, and why is it not yet routine in orthopaedics?”
Tissue-engineering triad
- Cells: MSCs (marrow/adipose), chondrocytes, osteoblasts
- Scaffold: 3D porous biodegradable (collagen/hydrogel; PLGA/PCL/ceramic/nanofibre)
- Signals: growth factors (BMP, TGF-beta, PDGF, VEGF) + mechanical stimuli
Clinical reality
- ACI/MACI - established cartilage technique
- Recombinant BMP-2/7 on collagen carrier (spine fusion, tibial nonunion)
- Orthobiologics adjunctive; whole-tissue constructs/gene therapy investigational
Gene therapy
- Deliver gene -> cells make protein (sustained local expression)
- Viral (efficient; immunogenicity/insertional mutagenesis) vs non-viral (safer, less efficient)
- In vivo (direct) vs ex vivo (modify cells -> re-implant; gene-activated matrix)
Challenges
- Vector safety; controlled, sustained expression
- Vascularising large constructs; cell-scaffold-signal optimisation
- Manufacturing, cost, regulation -> mostly experimental
Evidence & Key Studies
Paracrine signals and a gelatin hydrogel scaffold for enthesis (rotator cuff) tissue engineering
- Demonstrates the tissue-engineering triad: mesenchymal stem cells (cells) within a gelatin hydrogel (scaffold) responding to chondrogenic signals (TGF-beta3 and BMP-4) to form fibrocartilage/enthesis tissue.
- Growth-factor and paracrine signals drove enthesis-associated matrix and transcription-factor expression, showing how signals direct differentiation.
- Illustrates a spatially graded biomaterial approach for regenerating the tendon-to-bone enthesis.
Bioactive nanofibrous scaffold for annulus fibrosus repair in disc degeneration
- A biodegradable nanofibrous polyurethane scaffold loaded with a bioactive factor (fucoidan) supported annulus fibrosus repair in intervertebral disc degeneration.
- The bioactive scaffold reduced inflammation and oxidative stress and promoted extracellular-matrix deposition, maintaining disc height and mechanical properties in vivo.
- Highlights both the promise (scaffold + bioactive signal) and a key challenge - the foreign-body reaction and harsh degenerative microenvironment.
The use of cells within a scaffold responding to growth-factor signals (TGF-beta/BMP) to engineer enthesis tissue comes from the cited Timmer study, and the scaffold-plus-bioactive-factor approach - with the foreign-body-reaction challenge - for disc repair from the cited Yu study. The tissue-engineering triad, the ACI/MACI and recombinant-BMP clinical examples, and the viral/non-viral, in-vivo/ex-vivo gene- therapy framework with its safety limitations are standard, well-established teaching. (See also our Orthobiologics, Stem Cells (MSC) and Bone Grafts topics.)