Glucocorticoid-Induced & Secondary Osteoporosis
Glucocorticoid-treated patients fracture at a higher BMD than in postmenopausal osteoporosis because bone quality (microarchitecture) is impaired, not just density - so a 'not that low' T-score is falsely reassuring. Assess clinical risk and treat early (loss is fastest in the first months).
Glucocorticoids cause two distinct bone problems: generalised osteoporosis (this topic) and focal osteonecrosis/AVN (e.g. femoral head). New hip/groin pain in a steroid patient needs an MRI for AVN, not just a DXA.
Overview & Epidemiology: When to Suspect a Secondary Cause
Most osteoporosis in older women is primary (postmenopausal), but you must actively look for a secondary cause when the picture is atypical: men, premenopausal women and children with osteoporosis; very low BMD or a fragility fracture out of proportion to age; osteoporosis in someone on a culprit drug (especially long-term glucocorticoids); a relevant systemic disease; or ongoing bone loss / fracture despite treatment. Identifying and treating the cause is often more effective than adding another bone drug.
GIOP is the commonest form of secondary osteoporosis and the commonest iatrogenic cause, with an estimated annual fracture rate of around 5% in treated patients (Saag, 2018) - which is why a steroid-treated patient is a standing fracture-risk problem, not an incidental one.
- Examples
- Glucocorticoids (commonest), aromatase inhibitors, androgen-deprivation therapy, anticonvulsants, prolonged PPIs, heparin, SSRIs, thiazolidinediones
- Examples
- Hyperparathyroidism, hyperthyroidism, hypogonadism, Cushing syndrome, diabetes
- Examples
- Malabsorption, coeliac disease, inflammatory bowel disease, post-bariatric, liver disease
- Examples
- Chronic kidney disease / renal osteodystrophy
- Examples
- Multiple myeloma, mastocytosis, thalassaemia
- Examples
- Rheumatoid and other inflammatory disease; immobilisation; alcohol excess; smoking
Pathophysiology: Bone Quality & How Glucocorticoids Damage Bone
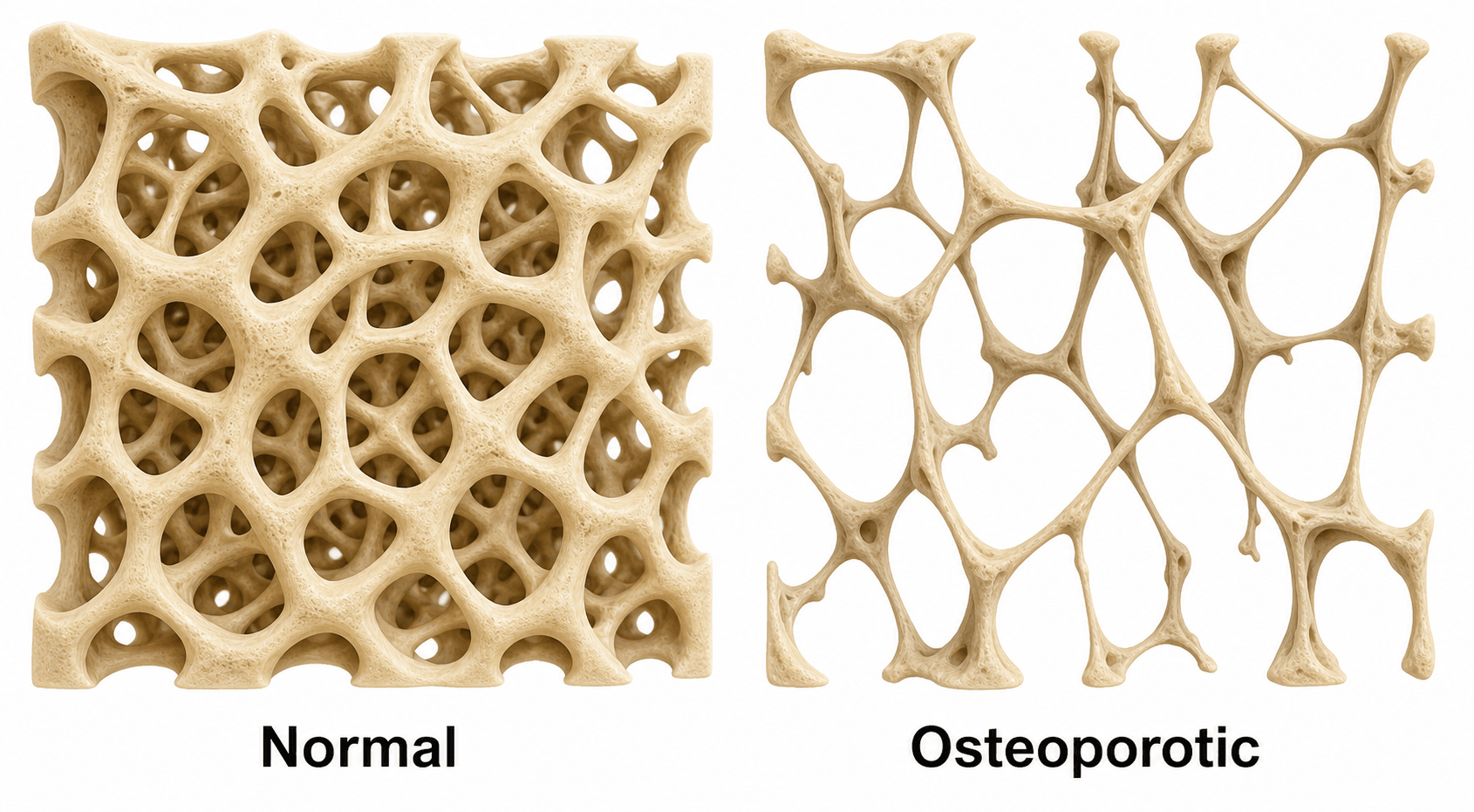
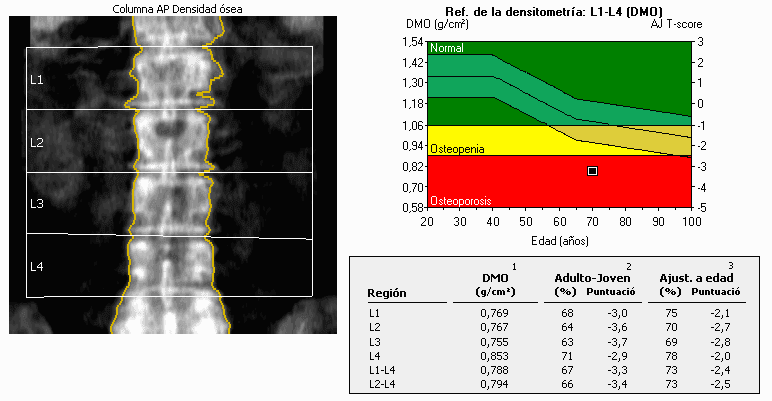
Osteoporosis is defined operationally on DXA as a T-score of −2.5 or lower (osteopenia −1 to −2.5), but the image makes the deeper point: strength depends on microarchitecture (trabecular number, connectivity and thickness), not density alone. That is precisely why GIOP — which degrades quality more than quantity — causes fractures at a higher BMD than postmenopausal osteoporosis, and why the T-score under-reads risk in steroid-treated patients.
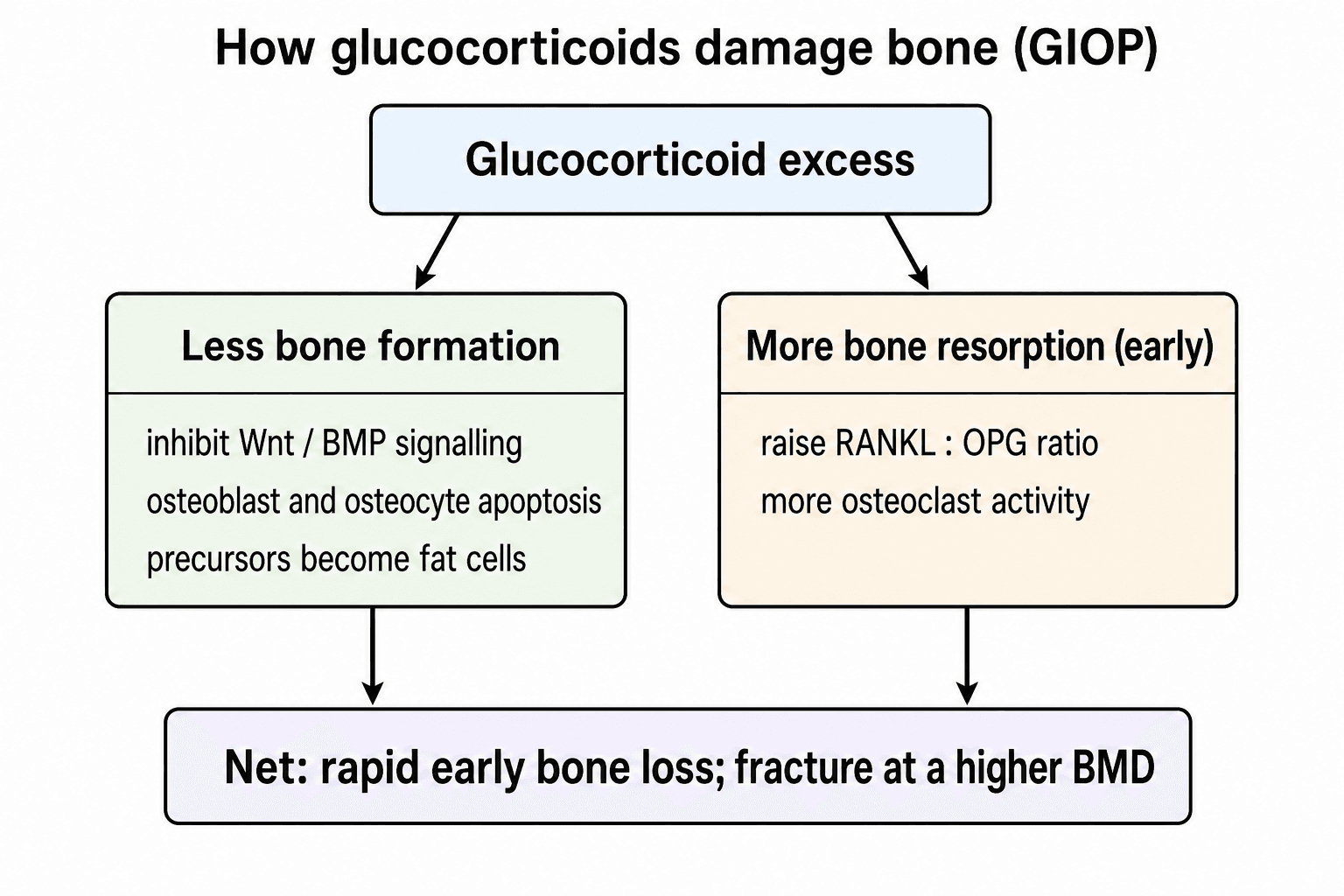
Glucocorticoids damage bone through several routes at once:
- Suppress bone formation — they inhibit Wnt/β-catenin and BMP signalling, diverting mesenchymal precursors to adipocytes rather than osteoblasts, and cause osteoblast and osteocyte apoptosis.
- Increase resorption early — they raise the RANKL:OPG ratio, enhancing osteoclast maturation and activity (a relatively early, transient phase).
- Indirect effects — reduced intestinal calcium absorption, increased renal calcium loss, and hypogonadism (sex-steroid suppression).
The net result is a rapid early phase of bone loss followed by ongoing formation suppression.
Glucocorticoids suppress bone formation (osteoblast/osteocyte apoptosis, reduced Wnt/BMP) as well as increasing early resorption; bone loss is fastest in the first months and partly dose-dependent.
Patients on glucocorticoids fracture at a higher BMD than in postmenopausal osteoporosis (bone quality, not just density, is impaired), so risk is underestimated by T-score alone — assess clinical risk and treat earlier.
Investigations: Secondary-Cause Screen & Fracture-Risk Assessment
Before attributing osteoporosis to age, screen for the common, treatable secondary causes (tailored to the patient): serum calcium and phosphate, renal and liver function, 25-hydroxy vitamin D, PTH, TSH, testosterone (in men), coeliac serology, and a myeloma screen (FBC/ESR, protein electrophoresis) where indicated; consider 24-hour urinary calcium, cortisol testing, and others as the history directs. Finding a secondary cause changes management — you treat the cause.
The interpretive key: in uncomplicated osteoporosis, primary or glucocorticoid-induced, the routine bone biochemistry - serum calcium, phosphate, alkaline phosphatase and PTH - is characteristically NORMAL. The secondary-cause screen is therefore aimed at unmasking the mimics whose biochemistry is abnormal:
- Osteomalacia - low or normal calcium, low phosphate, high alkaline phosphatase, high PTH, low vitamin D
- Primary hyperparathyroidism - high calcium with a high PTH
- Paget's disease - an isolated high alkaline phosphatase (normal calcium/phosphate)
- Multiple myeloma - high calcium, high ESR, a paraprotein on electrophoresis
- Renal osteodystrophy (CKD) - high phosphate, high PTH, abnormal calcium
An abnormal result moves you off the osteoporosis pathway and onto treating that disease - which is exactly why the panel is worth sending even when osteoporosis seems obvious.
≥2.5 mg/dprednisolone, ≥3 months is the ACR threshold that triggers fracture-risk assessment — and for high-dose glucocorticoids (over ~7.5 mg/day), FRAX can be adjusted upward, because standard FRAX underestimates risk at higher steroid doses.
For adults starting or continuing GCs ≥2.5 mg/day prednisolone-equivalent for ≥3 months, assess fracture risk as soon as possible after starting: clinical fracture-risk assessment, BMD with vertebral fracture assessment (or spinal X-ray), and FRAX if 40 years or older (adjusted for GC dose). Stratify into low, medium, high or very-high fracture risk — prior fragility fracture, very low BMD and high FRAX scores push patients into the higher categories.
Clinical Presentation
GIOP is usually asymptomatic until a fragility fracture - characteristically a vertebral compression fracture (back pain, height loss, kyphosis), but also hip and other low-trauma fractures. Because loss is fastest in the first months of treatment and patients fracture at a higher BMD, the first presentation can be a fracture in someone whose DXA looked only mildly reduced. The practical lesson is to identify the at-risk steroid patient before the fracture, not after it.

Glucocorticoids cause two distinct bone problems: generalised osteoporosis (this topic) and focal osteonecrosis (avascular necrosis) — classically of the femoral head — through a different mechanism (marrow fat, vascular and apoptotic effects). A steroid-treated patient with new hip/groin pain needs to be worked up for osteonecrosis (MRI), not just assumed to have osteoporosis.
Management (2022 ACR Algorithm)
Optimise calcium and vitamin D, lifestyle measures (weight-bearing exercise, stop smoking, limit alcohol, falls reduction), and use the lowest effective GC dose for the shortest time. These apply regardless of risk category.
Reassess fracture risk and repeat DXA periodically (commonly every 1-2 years while on glucocorticoids, or sooner if the steroid dose is high), and re-evaluate when glucocorticoids stop - bone partly recovers, so treatment can sometimes be stepped down once the steroid (and its risk) is withdrawn, provided the patient is no longer high-risk. Throughout, the single most effective bone-protective move remains using the lowest effective glucocorticoid dose for the shortest time and treating the underlying disease.
Because GIOP bone loss is fastest at the start, do not delay assessment and treatment until a follow-up DXA shows loss. If denosumab is used and then stopped, there is a rebound increase in bone resorption with a risk of multiple vertebral fractures — so plan sequential therapy (e.g. transition to a bisphosphonate) rather than simply discontinuing.
Complications & Prognosis
- Detail
- Vertebral (commonest), hip and other low-trauma fractures - the endpoint GIOP treatment exists to prevent
- Detail
- Impaired bone quality means fractures occur at a higher BMD than postmenopausal OP - risk is under-read by T-score
- Detail
- Stopping denosumab causes a surge in resorption and multiple vertebral fractures - plan sequential therapy
- Detail
- Focal AVN (e.g. femoral head) - a distinct steroid complication needing MRI, not a feature of GIOP
- Detail
- Largely preventable: bone loss is partly reversible and fracture risk falls with early calcium/vit D plus an effective agent and the lowest GC dose
The antiresorptives the algorithm recommends carry rare but important long-term complications you should counsel about. An atypical femoral fracture (AFF) is a transverse or short-oblique fracture of the subtrochanteric/diaphyseal femur with minimal trauma, often with prodromal thigh or groin pain, localised lateral cortical thickening ('beaking') and a medial spike, and is frequently bilateral - associated with prolonged bisphosphonate (and also denosumab) use; it warrants stopping the drug, imaging the contralateral femur, and prophylactic fixation of a painful incomplete lesion. Osteonecrosis of the jaw (ONJ) - exposed necrotic jaw bone - is rare at osteoporosis doses (commoner at oncology dosing) and is reduced by dental assessment before and during therapy. These risks are why therapy is reviewed periodically and a drug holiday considered for bisphosphonates - but not a simple stop for denosumab (rebound, as above).
Mnemonics & Memory Aids
STEROIDGIOP mechanism in one word
Hook:STEROID captures GIOP: suppressed formation, early loss, fracture at higher BMD, assess and treat.
SECONDSecondary causes
Hook:Think SECOND causes in the atypical patient: steroids, endocrine, coeliac, other drugs, myeloma, kidney.
ABCDThe 2022 ACR management
Hook:ABCD of GIOP care: Assess early, Bone agent if high-risk, Calcium/vit D for all, Don't stop denosumab abruptly.
Viva practice
Practise clinical reasoning and management decisions out loud
“A 58-year-old man on long-term prednisolone for an inflammatory condition is referred after a low-trauma vertebral fracture. How do glucocorticoids damage bone, and how would you assess and treat his osteoporosis?”
“When would you suspect a secondary cause of osteoporosis, and what would your screening workup include?”
Suspect secondary when
- Men, premenopausal women, children; disproportionate BMD/fracture
- On glucocorticoids or other culprit drug; relevant systemic disease
- Ongoing loss/fracture despite treatment
GIOP mechanism
- Down Wnt/BMP + osteoblast/osteocyte apoptosis (down formation)
- Up RANKL:OPG (early up resorption); down Ca absorption, hypogonadism
- Fast early loss; fractures at higher BMD than postmenopausal
Workup
- Ca/PO4, renal/liver, 25-OH vit D, PTH, TSH, testosterone (men)
- Coeliac serology, myeloma screen (FBC/ESR, electrophoresis)
- DXA with vertebral fracture assessment + FRAX
GIOP management (2022 ACR)
- Assess if GC at least 2.5 mg/day for at least 3 months (clinical + DXA/VFA + FRAX if 40+)
- All: Ca/vit D, lifestyle, lowest effective GC dose
- Medium/high/very-high risk: bisphosphonate, denosumab or PTH analogue; anabolic conditionally first-line if high-risk; plan sequential therapy
Evidence
2022 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis
- For adults on more than 3 months of GCs at 2.5 mg/day or more, strongly recommends early fracture-risk assessment: clinical assessment, BMD with vertebral fracture assessment/spinal X-ray, and FRAX if 40 years or older.
- For medium/high/very-high fracture risk, pharmacologic treatment is strongly recommended; choice of oral/IV bisphosphonate, denosumab or PTH analogue by shared decision-making.
- Anabolic agents are conditionally recommended as initial therapy for high and very-high risk; new recommendations cover discontinuation and sequential therapy.
Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover
- Excess glucocorticoids interfere with the canonical BMP pathway and inhibit Wnt protein production, causing mesenchymal progenitors to differentiate to adipocytes rather than osteoblasts.
- Glucocorticoids increase the RANKL:OPG ratio (promoting osteoclast maturation/resorption) and cause osteoblast and osteocyte apoptosis, reducing formation.
- Avoiding excess glucocorticoid use is mandatory in GIOP — explaining why GIOP both suppresses formation and (early) increases resorption.
The assessment/treatment algorithm comes from the 2022 ACR practice guideline (Humphrey et al., DOI), the molecular mechanism from the Cheng et al. review (DOI), the anabolic-versus-bisphosphonate fracture data from the teriparatide-versus-alendronate RCT (Saag et al. 2009, DOI), and the denosumab-versus-risedronate data from Saag et al. 2018 (DOI). The list of secondary causes, the screening panel, the FRAX glucocorticoid-dose adjustment and the osteonecrosis distinction are standard, well-established clinical knowledge. (See also our Osteoporosis, Osteonecrosis and Bone Signalling Pathways topics.)