Gustilo-Anderson Classification of Open Fractures
- Letting wound size set the grade. Size alone NEVER decides it — a small wound from a high-velocity gunshot, crush or heavy contamination is a Type III. Energy, contamination and neurovascular status upgrade the grade regardless of length.
- Finalising the grade in the ED. The grade is finalised at operative debridement and can be UPGRADED but never downgraded — an apparent Type II with periosteal stripping is a IIIB.
- Confusing IIIB with IIIC. IIIB = extensive soft-tissue loss/periosteal stripping needing a flap, with intact circulation; IIIC = an arterial injury requiring repair. The distinction is vascular, not the size of the wound.
- Equating IIIC with amputation. IIIC has the highest amputation rate but is NOT an automatic amputation — use the limb assessment (e.g. MESS) and orthoplastic input; the grade does not make that decision.
- Prioritising the 6-hour debridement myth over antibiotics. Antibiotics within 1 hour matter more than the exact debridement time — cefazolin for all, add gentamicin for III, add penicillin for farm/freshwater/sewage (Clostridium); 48–72 h duration.
The Gustilo-Anderson classification
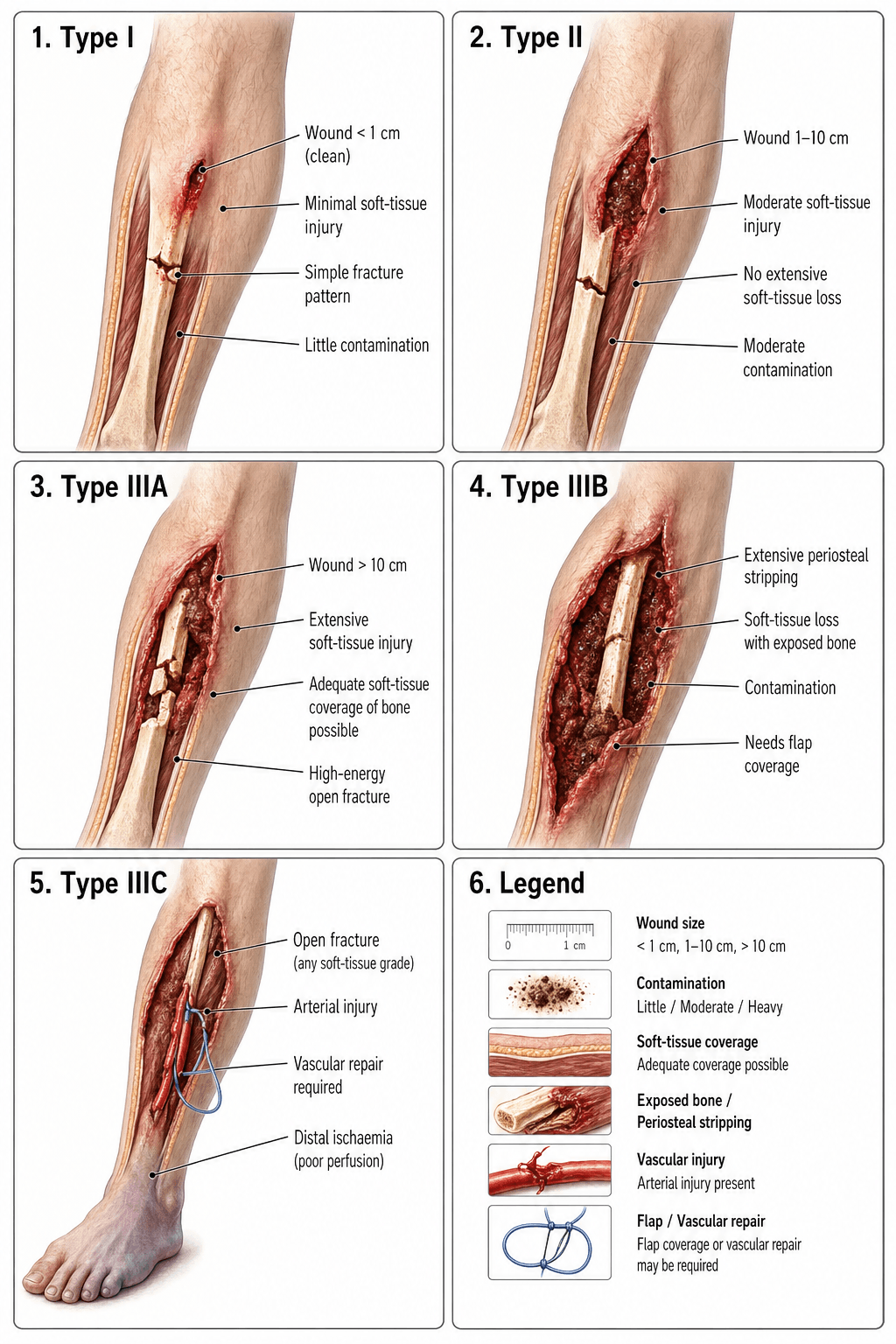
The system grades open fractures from Type I (least severe) to Type III (most severe), with Type III divided into A, B, and C. The final grade is determined in the operating room at debridement, not from the emergency department alone, because the true soft-tissue injury may not be apparent until surgical exploration.

- Wound size
- Less than 1 cm
- Soft-tissue injury
- Minimal, clean wound
- Contamination
- Clean
- Neurovascular
- Intact
- Wound size
- 1 to 10 cm
- Soft-tissue injury
- Moderate muscle damage, no extensive crushing
- Contamination
- Moderate
- Neurovascular
- Intact
- Wound size
- Over 10 cm OR high energy
- Soft-tissue injury
- Adequate soft-tissue coverage of bone achievable
- Contamination
- Heavy (may include farm/sewage)
- Neurovascular
- Intact
- Wound size
- Over 10 cm OR high energy
- Soft-tissue injury
- Extensive periosteal stripping, massive loss; flap coverage required
- Contamination
- Heavy
- Neurovascular
- Intact
- Wound size
- Any size with arterial injury
- Soft-tissue injury
- Variable — often severe
- Contamination
- Variable
- Neurovascular
- Arterial injury requiring repair
Small · Moderate · Massive, then A-B-CThe three types and subtypes
Hook:A = Adequate coverage, B = Blown tissue (needs flap), C = Circulation compromised. The grade can be upgraded at surgery, never downgraded.
The grade can be upgraded but never downgraded. If initial inspection suggests Type II but operative debridement reveals periosteal stripping, it becomes Type IIIB. And wound size never sets the grade alone — a small wound from a high-velocity gunshot or crush can be a Type III. Always finalise the grade at operative debridement.
Clinical decision rules — antibiotics, debridement & fixation

- Type I
- Cefazolin (first-generation cephalosporin)
- Type II
- Cefazolin
- Type III
- Cefazolin + gentamicin (Gram-negative cover)
- Type I
- Penicillin (Clostridium cover)
- Type II
- Penicillin
- Type III
- Penicillin
- Type I
- 48–72 h post-debridement or 24 h after closure
- Type II
- 48–72 h post-debridement or 24 h after closure
- Type III
- 48–72 h post-debridement or 24 h after closure
- Type I
- Urgent (within ~6 h, ideally sooner)
- Type II
- Urgent (within ~6 h)
- Type III
- Urgent — immediate once stabilised
- Type I
- Usually definitive at index procedure
- Type II
- External fixation or definitive if soft tissues allow
- Type III
- Spanning external fixation, then staged definitive fixation
- Type I
- Primary or delayed primary closure
- Type II
- Delayed primary or skin graft
- Type III
- IIIA: delayed primary/local flap; IIIB: free flap; IIIC: revascularise then cover
Administer antibiotics within 1 hour of presentation — do not wait for theatre; every hour of delay increases infection risk. Debridement should follow urgently (traditionally within 6 hours), though modern evidence suggests the exact 6-hour threshold matters less than early antibiotics and a thorough surgical debridement.
Cephalosporin all · Gentamicin for III · Penicillin for Pond/farmAntibiotic selection by grade
Hook:Antibiotics within 1 hour, before theatre. Duration: 48–72 h post-debridement or 24 h after wound closure.
Debridement is the single most important infection-control step, and the examiner expects the technique, not just "washout":
- A systematic, layer-by-layer excision through an extensile approach — excise devitalised skin, fat, fascia and muscle, deliver and clean the fracture ends, and remove all foreign material. Loose avascular cortical fragments with no soft-tissue attachment are discarded (large articular fragments are retained), and a planned second-look debridement at 48–72 h is the norm for high-grade wounds.
- Judge muscle viability by the "4 Cs" — Colour, Consistency, Contractility and Capacity to bleed — and excise muscle that fails them.
- Irrigation — the FLOW trial evidence — the large FLOW randomised trial compared irrigation pressures (high / low / very-low) and solutions (soap vs saline) and found no benefit of high pressure, while soap had a HIGHER reoperation rate than saline. The lesson: use low-pressure normal saline; high-pressure pulsatile lavage and additive soap are not advantageous and may drive contaminant deeper.
- The "6-hour rule" is a myth — a thorough debridement and antibiotics within 1 hour matter more than hitting an exact 6-hour mark; debride urgently but well rather than hastily.
Two wound-management adjuncts are easy marks the grade itself omits:
- Tetanus prophylaxis — an open fracture is usually a tetanus-prone wound (more than 6 hours old, deep, contaminated with soil/faeces, devitalised, or a puncture/missile injury). Management follows immunisation status: a fully immunised patient with a booster in the last 10 years usually needs nothing; an incomplete or uncertain history warrants a tetanus toxoid (Td/Tdap) booster, and human tetanus immunoglobulin is added for a tetanus-prone/high-risk wound in an incompletely immunised or unknown-status patient.
- Local antibiotic adjuncts — for dead-space management in Type III wounds, antibiotic-impregnated cement (PMMA) beads (vancomycin/tobramycin/gentamicin) deliver very high local concentrations while systemic antibiotics continue; antibiotic-loaded bioabsorbable carriers and local vancomycin/aminoglycoside at the wound have been studied as adjuncts to reduce deep infection. These supplement, not replace, the systemic prophylaxis.
Limitations, reliability & modern context
- Inter-observer reliability is only moderate. Brumback & Jones found ~60% average agreement among 245 surgeons, weakest for distinguishing IIIA from IIIB (the periosteal-stripping criterion is the most contentious).
- Wound size is a poor proxy for energy. A small wound from a high-velocity gunshot or crush can cause devastating soft-tissue injury — the system explicitly allows upgrading for high-energy mechanisms regardless of wound length.
- Type IIIC does not mandate amputation. Amputation rates for IIIC are high, but modern microsurgical reconstruction and the Mangled Extremity Severity Score (MESS) guide the salvage-versus-amputation decision — Gustilo-Anderson alone does not make that call.
- Patient factors are not captured — age, diabetes, vascular disease, smoking and polytrauma all influence outcome but are absent from the grade.
- Antibiotic duration is shortening — contemporary evidence supports 48–72 h post-debridement (or 24 h after closure); prolonged courses add no benefit and increase resistance.
- The OTA/OFC system (2010) scores skin, muscle, arterial, contamination and bone loss independently to address Gustilo's reliability limits, but has not replaced it in routine practice or exam syllabi.
Guidelines, registries & global practice
Open-fracture guidelines broadly agree on early antibiotics and urgent debridement but differ in specificity.
- Antibiotic timing
- Within 1 hour
- Duration
- 48–72 h post-debridement
- Debridement timing
- Urgent; expedited for highly contaminated / vascular injury
- Antibiotic timing
- As soon as possible
- Duration
- 48–72 h
- Debridement timing
- Urgent (historically within 6–8 h)
- Antibiotic timing
- Immediate on admission
- Duration
- 48–72 h or 24 h after closure
- Debridement timing
- Urgent (within ~6 h)
- Antibiotic timing
- Within 1 hour (timing matters more than duration)
- Duration
- Short course (≤72 h, even 24–48 h)
- Debridement timing
- Thorough debridement; exact 6-h cutoff less critical
- Registry data (Swedish Fracture Register, UK TARN) show infection in Type III open tibial fractures remains roughly 15–30% in contemporary practice despite protocolised care, with IIIB/IIIC driving most morbidity.
- Global practice variation is driven by resources — flap coverage for IIIB (free latissimus dorsi or ALT flap) requires microsurgical expertise unavailable in some settings, where external fixation, secondary healing or amputation rates are higher. WHO Essential Surgery stresses early antibiotics and debridement as the non-negotiable minimum.
- Resistance patterns vary — high-MRSA regions may add or substitute Gram-positive cover (e.g. vancomycin/clindamycin), beyond the original Gustilo-era recommendations.
Viva practice
- 1Resuscitate + antibiotics within 1 hourATLS; cefazolin for all, add gentamicin for Type III, add penicillin for farm/freshwater/sewage contamination; tetanus prophylaxis.
- 2Provisional grade + wound carePhotograph, remove gross debris, saline dressing (do NOT close), splint, neurovascular check. Wound size is provisional — energy/contamination/NV status can upgrade it.
- 3Urgent operative debridementThorough irrigation and excision of non-viable tissue; FINALISE the grade here (upgrade only). Spanning external fixation for Type III; definitive fixation for I/II if soft tissues allow.
- 4Staged coverage & fixationIIIA local flap/closure; IIIB free flap (typically by ~5–7 days) then definitive fixation; IIIC revascularise first (MESS to weigh salvage vs amputation). Antibiotics 48–72 h per debridement.
- I under 1 cm clean; II 1–10 cm moderate; III over 10 cm OR high-energy OR heavy contamination OR arterial injury (size never downgrades).
- IIIA coverage achievable; IIIB needs a flap (periosteal stripping); IIIC arterial injury requiring repair (highest amputation rate).
- Grade upgraded but never downgraded — finalise at debridement.
- Cefazolin within 1 hour for all; add gentamicin for III; add penicillin for farm/water; 48–72 h duration.
- Reliability is only moderate (~60%), weakest IIIA-vs-IIIB.
- IIIC ≠ automatic amputation — use MESS; patient factors aren't in the grade.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old man is brought to the emergency department after a motorbike collision. He has an open tibial shaft fracture with a 4 cm wound on the anteromedial shin. The wound is moderately contaminated with road dirt. Distal pulses are palpable, and toe dorsiflexion is intact. How do you classify this fracture, and what is your initial management?”
“A 42-year-old farmer sustains a Gustilo-Anderson Type IIIB open tibial fracture in a tractor rollover. The wound is heavily contaminated with soil, with extensive periosteal stripping over 8 cm. The posterior tibial pulse is present. Walk me through your staged management.”
Exam cheat sheet
Classification
- Type I: wound under 1 cm, clean, low energy, intact NV
- Type II: wound 1–10 cm, moderate soft-tissue injury, intact NV
- Type III: over 10 cm OR high-energy OR heavy contamination (regardless of wound size)
- IIIA coverage achievable; IIIB periosteal stripping → flap; IIIC arterial injury → repair
Antibiotics & timing
- All open fractures: cefazolin within 1 hour of presentation
- Type III: add gentamicin (Gram-negative cover)
- Farm/river/sewage: add penicillin (Clostridium)
- Duration: 48–72 h post-debridement or 24 h after wound closure
Key pitfalls
- Grade upgraded at debridement but never downgraded
- Wound size alone does not determine type — energy/contamination can upgrade it
- Type IIIC ≠ automatic amputation — use the MESS score
- Classify definitively in theatre, not in the emergency department
Evidence
Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses
- The original Gustilo-Anderson paper (1025 open long-bone fractures) introduced the three-type system (I, II, III) and a prophylactic-antibiotic + debridement protocol.
- Prospective protocolised care cut the overall infection rate to 2.5% (and the Type III rate from 44% retrospectively to 9% prospectively).
- Infection risk correlated with the severity of soft-tissue injury; a cephalosporin was recommended as the prophylactic of choice.
Problems in the management of type III (severe) open fractures: a new classification of type III open fractures
- Subdivided Type III into A (coverage achievable), B (periosteal stripping/bone exposure needing a flap) and C (arterial injury requiring repair).
- Wound-sepsis rates were IIIA ~4%, IIIB ~52%, IIIC ~42%; amputation rates were 0%, 16% and 42% respectively (only 2 patients developed osteomyelitis overall).
- Gram-negative organisms then dominated infections, prompting the move from a cephalosporin alone to a cephalosporin plus an aminoglycoside for Type III.
According to PubMed, the classification comes from Gustilo & Anderson 1976 (PMID 773941; the original I/II/III system) and the A/B/C subdivision plus the sepsis (IIIA 4%, IIIB 52%, IIIC 42%) and amputation (0%/16%/42%) rates from Gustilo et al. 1984 (DOI 10.1097/00005373-198408000-00009). The moderate reliability (~60% agreement) comes from Brumback & Jones 1994 (DOI 10.2106/00004623-199408000-00006), the short-antibiotic-course evidence from Messner et al. 2017 (DOI 10.1089/sur.2017.108), and the alternative OTA/OFC system from the OTA Open Fracture Study Group 2010 (DOI 10.1097/BOT.0b013e3181c7cb6b).