Repetitive compressive loading of the open distal radial physis | Dorsal wrist pain in young gymnasts | X-ray shows physeal widening and irregularity | MRI stages the stress injury | Rest early or risk premature physeal arrest and positive ulnar variance
- What it is: a stress injury of the open distal radial physis caused by repetitive compressive loading in young gymnasts (and other wrist-loading athletes) - it is an overuse physeal injury, not an acute Salter-Harris fracture
- Presentation: dorsal wrist pain during weight-bearing activities (handstands, vault, beam), tenderness over the distal radial physis, and reduced grip or willingness to load the wrist - the hallmark is pain on axial compression of the hyperextended wrist
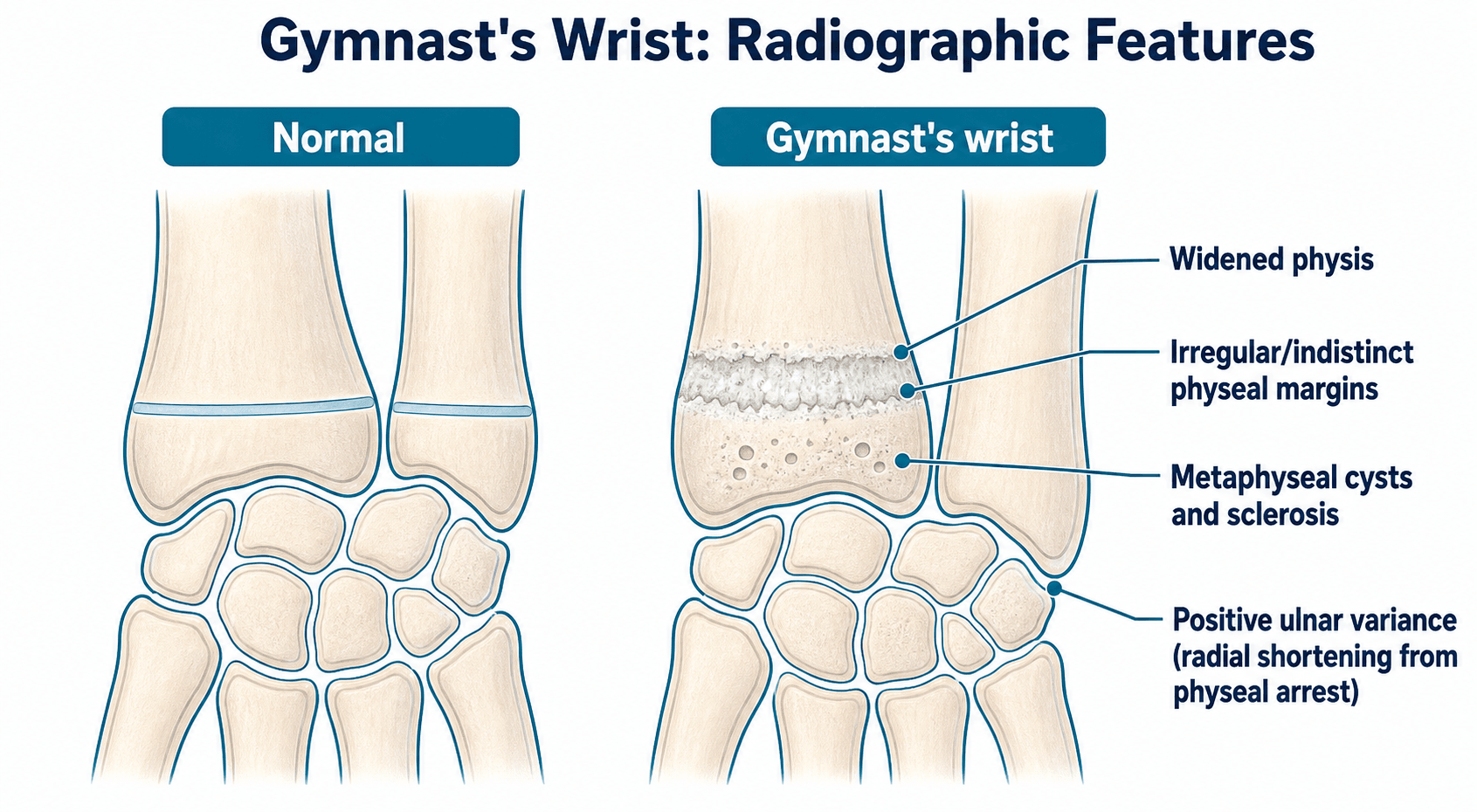
- Investigation: plain radiographs may show physeal widening, irregularity, cystic metaphyseal changes, or sclerosis; MRI is the gold standard and shows physeal widening with bone marrow oedema on fluid-sensitive sequences (the key finding)
- Management: graded - early identification and activity modification (reducing wrist loading) is the mainstay; splinting or casting for persistent cases; surgery (radial epiphysiodesis or ulnar shortening) is reserved for physeal arrest with progressive positive ulnar variance
- Complications: premature partial or complete physeal arrest of the distal radius leading to progressive positive ulnar variance, ulnar impaction syndrome, triangular fibrocartilage complex tears, and degenerative changes in the adult wrist
- “Gymnast's wrist is a REPETITIVE STRESS injury of the distal radial physis, not an acute Salter-Harris fracture - but the physis is the same structure and the mechanism is cumulative microtrauma
- “Ulnar variance progresses from neutral or negative to POSITIVE when the distal radial physis arrests prematurely - this is the long-term problem to watch for
- “MRI findings (physeal widening with bone marrow oedema) are present before plain radiograph changes - if you suspect it clinically and the X-ray looks normal, go to MRI
- “Activity modification is the treatment cornerstone: the gymnast who rests early recovers; the gymnast who pushes through risks permanent growth disturbance
Gymnast's wrist is chronic repetitive microtrauma to the open distal radial physis. It is not an acute Salter-Harris fracture, although the anatomy is the same. The examiner wants you to say "overuse physeal stress injury" and explain the mechanical basis (compression and dorsal shear from axial loading of the wrist in extension).
Premature partial or complete arrest of the distal radial physis shortens the radius relative to the ulna, producing progressive positive ulnar variance. This leads to ulnar impaction syndrome, TFCC tears, and degenerative change. Serial radiographs tracking ulnar variance are essential.
Plain radiographs can be normal early in the disease. MRI shows physeal widening and bone marrow oedema on fluid-sensitive sequences before radiographic irregularity develops. A symptomatic gymnast with a normal X-ray warrants MRI if the diagnosis is suspected.
Activity modification (reducing or eliminating weight-bearing through the wrist) is the primary treatment and is highly effective when started early. Casting or splinting for four to six weeks is used for persistent symptoms. The gymnast who continues to train through pain risks permanent physeal damage.
Overview
Gymnast's wrist is a repetitive stress injury of the open distal radial physis caused by chronic compressive loading of the wrist in young, skeletally immature athletes. It is the most common overuse injury of the wrist in competitive gymnasts, with studies reporting radiographic abnormalities in up to half of young gymnasts training at a high level. It also occurs in other sports that involve weight-bearing through the upper limb in wrist extension, such as cheerleading, martial arts, and certain field events in athletics.
The distal radial physis contributes roughly 70 to 80 percent of the longitudinal growth of the radius and about 40 percent of total forearm length. Repetitive axial compression and dorsal shear during gymnastics skills (vault, floor exercise, beam, rings, pommel horse, and handstands) overload this growth plate beyond its capacity to repair, producing a spectrum from physeal stress reaction through to physeal disruption and, in severe cases, premature physeal arrest.
The condition matters for three exam-relevant reasons: it is a classic example of an overuse physeal injury in the paediatric athlete, it illustrates the principle that MRI detects stress injury before plain radiograph changes appear, and the feared complication of premature physeal arrest with progressive positive ulnar variance links paediatric sports medicine to adult wrist pathology (ulnar impaction syndrome).
Pathophysiology
Distal radial physis
The distal radial physis (growth plate) lies between the metaphysis and epiphysis of the distal radius. Key anatomical points:
- It is one of the most active physes in the body, contributing approximately 70 to 80 percent of radial longitudinal growth and roughly 40 percent of overall forearm length
- It typically closes at around 16 to 18 years in girls and 17 to 19 years in boys
- During gymnastics, the upper limb is a weight-bearing strut: forces of 2 to 4 times body weight are transmitted across the wrist during skills such as vaulting, back handsprings, and handstands
- In wrist hyperextension, the lunate compresses the volar aspect of the distal radial physis, while dorsal shear loads the dorsal physis
Pathomechanics
The injury develops through a cycle of repetitive microtrauma exceeding the rate of repair:
- Axial compression across the wrist loads the physis during weight-bearing skills
- Dorsal shear in hyperextension adds an angular stress component
- The physis responds with hypertrophy and widening of the physeal cartilage (a stress reaction)
- With continued loading, the physis develops microfractures of the zone of provisional calcification, metaphyseal bone resorption, and bone marrow oedema
- In severe or prolonged cases, the physis may partially or completely arrest prematurely, producing progressive positive ulnar variance
The dorsal and volar margins of the physis are most vulnerable because they experience the highest shear stresses. This explains why MRI often shows focal widening of the volar or dorsal physis rather than uniform widening.
The pathophysiology parallels a Salter-Harris type I stress injury - but instead of a single acute episode, the microtrauma is cumulative and repetitive. The examiner wants you to explain that the physis is the same structure, but the mechanism is chronic overload rather than a single acute force.
The skeletal-maturity spectrum: the weak link changes with age
A key conceptual point is that the site of overuse injury depends on skeletal maturity, because the load concentrates at whatever the weakest structure is:
- Open physis (the young gymnast) → the physis is the weak link → distal radial physeal stress injury (this topic).
- Closing / recently closed physis (older adolescent) → the load shifts to bone → distal radius stress fracture, and to the ulnar side → TFCC injury and ulnar impaction (compounded by any acquired positive ulnar variance).
- Mature wrist (adult gymnast) → repetitive loading produces carpal (capitate/scaphoid) stress injury, dorsal impaction/impingement, and degenerative change, often on a background of the positive ulnar variance acquired in childhood.
So "gymnast's wrist" in the strict sense is the physeal injury of the immature athlete; the same loading in a maturing or mature wrist manifests as a bony stress fracture or ulnar-sided/carpal pathology instead.
Classification
There is no single universally accepted classification system for gymnast's wrist. In practice, clinicians use a combination of radiographic grading and MRI staging to guide management.
- Radiographic findings
- No physeal abnormality
- Clinical significance
- No radiographic evidence of stress injury - but MRI may still show oedema
- Radiographic findings
- Physeal widening and/or irregularity, with or without mild metaphyseal cystic changes or sclerosis
- Clinical significance
- Early physeal stress reaction - responds well to activity modification
- Radiographic findings
- Physeal widening, irregularity, metaphyseal cysts, sclerosis, and early positive ulnar variance
- Clinical significance
- Established stress injury - requires enforced rest and close follow-up
- Radiographic findings
- Marked physeal disruption with progressive positive ulnar variance and signs of physeal arrest
- Clinical significance
- Risk of permanent growth disturbance - may need surgical intervention
Clinical Presentation
Who is affected
- Age: typically 10 to 14 years (skeletal immaturity with an open distal radial physis)
- Sex: both, but female gymnasts are more commonly affected in published series (reflecting higher participation rates and earlier peak training loads relative to skeletal maturity)
- Training level: competitive gymnasts training more than 15 to 20 hours per week are at highest risk; recreational gymnasts are less commonly affected
Symptoms
- Dorsal wrist pain that is worse during and after weight-bearing activities (handstands, vault, floor exercise, beam, rings)
- Pain often begins insidiously and worsens gradually over weeks to months
- Initially, pain is present only during high-impact skills; later it may occur with all wrist loading and even at rest
- Bilateral involvement is common (both wrists are loaded during gymnastics)
Signs
- Tenderness directly over the distal radial physis (palpable just proximal to the wrist joint on the radial side)
- Pain on axial compression of the wrist in hyperextension (reproducing the loading mechanism)
- Pain on passive wrist hyperextension
- Possible mild dorsal wrist swelling in more advanced cases
- Reduced grip strength or reluctance to bear weight through the wrist
- Normal range of motion unless there is established positive ulnar variance (then forearm rotation may be limited)
The clinical hallmark is pain on axial loading of the wrist in hyperextension, which reproduces the mechanism of injury. Press the patient's hand into extension against resistance while palpating the distal radial physis - this reproduces the pain in gymnast's wrist.
Always examine both wrists even if only one is symptomatic. Bilateral physeal stress changes are common, and the asymptomatic side may show early signs that warrant activity modification before symptoms develop.
Investigations
Plain radiographs (first-line)
Standard PA and lateral wrist radiographs are the initial investigation. A dedicated PA view in neutral forearm rotation (shoulder abducted 90 degrees, elbow flexed 90 degrees, forearm neutral) is essential for measuring ulnar variance accurately.
Radiographic findings in gymnast's wrist:
- What it looks like
- Increased transverse lucency at the distal radial growth plate on the PA view
- Significance
- The earliest and most specific radiographic sign - reflects physeal hypertrophy and stress reaction
- What it looks like
- Loss of the normal smooth, parallel margins of the physis
- Significance
- Indicates physeal disruption rather than just reactive widening
- What it looks like
- Small lucent areas and adjacent sclerosis in the distal radial metaphysis, adjacent to the physis
- Significance
- Chronic stress changes - the metaphysis is reacting to abnormal physeal load transfer
- What it looks like
- The distal ulnar articular surface is more distal than the distal radial articular surface on a neutral PA view
- Significance
- Indicates relative radial shortening from premature physeal arrest - the key finding that changes management
- What it looks like
- No visible physeal abnormality
- Significance
- Does not exclude the diagnosis - MRI is needed if clinical suspicion is high
MRI (gold standard)
MRI is the investigation of choice when the diagnosis is suspected clinically but radiographs are normal, or when staging the severity of physeal injury to guide return-to-sport decisions.
Key MRI findings:
- Physeal widening (especially volar and/or dorsal margins)
- Bone marrow oedema adjacent to the physis (high signal on T2 fat-suppressed or STIR sequences, low signal on T1)
- Physeal signal change (fluid-like signal extending through the physis)
- Metaphyseal cystic change and sclerosis (seen earlier than on plain radiographs)
Ulnar variance measurement
Ulnar variance is measured on a neutral rotation PA wrist radiograph by drawing a line perpendicular to the long axis of the radius through the ulnar border of the lunate fossa (radial articular surface) and measuring the distance to the distal ulnar articular surface:
- Negative variance: ulna is shorter than the radius (normal in most children)
- Neutral variance: equal lengths
- Positive variance: ulna extends beyond the radius (the pathological direction in gymnast's wrist)
Serial ulnar variance measurements on standardised neutral-rotation PA radiographs are the key to monitoring for premature physeal arrest. A progressive shift toward positive variance over serial visits is the radiographic hallmark of growth arrest and warrants referral for consideration of surgical intervention.


Differential Diagnosis
Dorsal/wrist pain in a young athlete has several causes; the distal radial physeal stress injury is the commonest in a high-volume gymnast, but the differential must be worked through clinically and on imaging.
- Discriminating feature
- Tender distal radial physis, pain on axial loading in hyperextension, open physis
- Key investigation
- X-ray (physeal widening) → MRI (physeal oedema)
- Discriminating feature
- Anatomical snuffbox tenderness, pain on axial thumb load
- Key investigation
- Scaphoid-series X-ray; MRI/CT if occult
- Discriminating feature
- Older adolescent with a closing/closed physis, dorsal metaphyseal pain
- Key investigation
- X-ray ± MRI (marrow oedema, fracture line)
- Discriminating feature
- Ulnar-sided pain, pain/click on forearm rotation, positive ulnar variance
- Key investigation
- MRI/MR arthrography; neutral-rotation PA for variance
- Discriminating feature
- Dorsal swelling or focal dorsal pain, transilluminates if cystic
- Key investigation
- Ultrasound or MRI
- Discriminating feature
- Pain on resisted/repetitive extension, dorsal swelling/crepitus
- Key investigation
- Clinical; ultrasound/MRI
- Discriminating feature
- Central/dorsal wrist pain, focal carpal tenderness
- Key investigation
- MRI (marrow signal change)
Management
Management is guided by the severity of physeal stress injury and the presence or absence of premature physeal arrest. The overarching principle is that the earlier the diagnosis and the sooner wrist loading is reduced, the better the outcome.
- Management
- Activity modification: reduce or stop weight-bearing wrist skills for 4 to 8 weeks. Maintain conditioning with lower-body and core training. Consider wrist guards or taping on return
- Return to sport
- Gradual reintroduction of wrist-loading skills once pain-free, typically 6 to 12 weeks. Follow-up X-ray to confirm resolution of physeal changes
- Management
- Short-arm cast or rigid splint for 4 to 6 weeks to enforce rest. MRI to assess physeal stress injury severity. Strict activity modification after cast removal
- Return to sport
- Minimum 3 months before gradual return to gymnastics. Repeat X-ray and possibly MRI before return. May need a full season off to allow physeal recovery
- Management
- Referral to a paediatric orthopaedic or upper-limb surgeon. Surgical options include distal radial epiphysiodesis to arrest remaining growth symmetrically, or ulnar shortening osteotomy if significant positive ulnar variance has developed
- Return to sport
- Extended rehabilitation. Return to gymnastics may not be possible or advisable. Long-term monitoring of ulnar variance and wrist function is essential
The vast majority of gymnast's wrist is managed non-operatively:
- Activity modification: the single most important intervention. Reduce or eliminate all weight-bearing through the wrist. The gymnast can continue non-weight-bearing conditioning (running, lower-body strength, core work).
- Immobilisation: a short-arm cast or rigid wrist splint for 4 to 6 weeks is used when activity modification alone has failed to settle symptoms.
- Physiotherapy: after the rest period, gradual rehabilitation of wrist range of motion, strength, and sport-specific loading under guidance.
- Wrist guards and taping: on return to sport, wrist guards (such as the Tiger Paw) or supportive taping can reduce dorsal wrist hyperextension and may help distribute load, though evidence for prevention is limited.
- Monitoring: serial radiographs every 3 to 6 months to track ulnar variance and physeal appearance during the recovery period and until skeletal maturity.
Complications
- Mechanism
- Chronic physeal disruption leads to partial or complete closure before skeletal maturity
- Key point
- Shortens the radius relative to the ulna, producing positive ulnar variance
- Mechanism
- Radial shortening from physeal arrest makes the ulnar head project more distally
- Key point
- Measured on serial neutral-rotation PA wrist radiographs; progressive change is the red flag
- Mechanism
- The elongated ulna abuts the lunate, compressing the TFCC and lunotriquetral articulation
- Key point
- Chronic ulnar-sided wrist pain, reduced grip strength, degenerative change
- Mechanism
- Positive ulnar variance overloads the triangular fibrocartilage complex
- Key point
- Ulnar-sided wrist pain, clicking, and pain on forearm rotation
- Mechanism
- Extended rest periods and rehabilitation
- Key point
- Psychological and competitive impact on the young athlete - involve coaches and parents early
- Mechanism
- Return to the same loading pattern that caused the injury
- Key point
- Risk is highest in gymnasts who return to full training too quickly or without technique modification
Premature physeal arrest
This is the most important complication to understand for the exam. The mechanism is:
- Repetitive loading damages the physis beyond its capacity for normal repair
- The zone of provisional calcification is disrupted, and bony bridges form across the physis (physeal bar formation)
- These bridges tether further growth: partial arrest causes angular deformity, complete arrest stops radial growth entirely
- The ulna continues to grow at its normal rate (the distal ulnar physis is unaffected)
- The result is progressive positive ulnar variance as the child grows - the discrepancy worsens with each year of remaining growth
- Positive ulnar variance leads to ulnar impaction (abutment of the ulnar head against the lunate), TFCC tears, and eventual degenerative arthritis
When asked about complications, lead with premature physeal arrest and positive ulnar variance - that is what the examiner is probing. The cascade is: chronic physeal stress leads to physeal arrest, which shortens the radius, which produces positive ulnar variance, which causes ulnar impaction and TFCC pathology.
Clinical Relevance
Gymnast's wrist is a viva favourite because it links paediatric sports medicine, physeal anatomy, imaging strategy (MRI before X-ray changes), and growth disturbance in a single clinical scenario that examiners across all training systems will recognise.
In the basic science viva, it is a perfect topic for discussing the structure and function of the physis, the blood supply of the growth plate, and how the zone of provisional calcification is the weakest link under shear stress. In the paediatric or upper-limb clinical viva, a young gymnast with dorsal wrist pain and physeal widening on X-ray is a straightforward spot diagnosis that leads into investigation strategy, management, and the complications of premature physeal arrest. In the trauma viva, understanding that the same physis that is injured acutely in a Salter-Harris fracture is injured chronically in gymnast's wrist demonstrates a sophisticated understanding of growth-plate pathology.
The key messages for the exam are: recognise the clinical pattern (young gymnast, dorsal wrist pain on loading, tender distal radial physis), use MRI when the X-ray is normal, rest early and enforce it, and monitor ulnar variance serially to catch premature physeal arrest before it produces irreversible positive ulnar variance.
Guidelines, Registries and Global Practice
- No single international guideline specifically addresses gymnast's wrist. Management is based on expert consensus, retrospective case series, and the general principles of overuse physeal injury management shared across paediatric sports medicine societies worldwide (AAP, AOSSM, EFOST, and equivalent national bodies).
- Activity modification as first-line treatment is universally agreed: reducing or eliminating compressive wrist loading until symptoms resolve and physeal changes normalise. The duration and degree of restriction vary by practice, but all published reviews agree that continued training through pain worsens the prognosis.
- MRI for early detection is increasingly standard in centres with access, reflecting the evidence that MRI shows physeal stress changes before plain radiographs. In settings without MRI access, a clinical diagnosis with enforced rest is acceptable, but the risk of underdiagnosis is acknowledged.
- Premature physeal arrest and positive ulnar variance are managed surgically in specialist centres globally. The threshold for ulnar shortening osteotomy varies (some surgeons operate at 2 to 3 mm positive variance with symptoms, others observe until variance is progressive and symptomatic), but the principle of addressing ulnar impaction before degenerative change is consistent.
- Prevention strategies under investigation include wrist guards (such as the Tiger Paw), technique modification to reduce hyperextension, training load monitoring, and periodic screening radiographs in high-level gymnasts. No consensus guideline mandates routine screening, but many elite gymnastics programmes in North America, Europe, and Australasia obtain baseline wrist radiographs and track ulnar variance in skeletally immature athletes.
Memory aids
GRIPClinical Presentation
Hook:A young Gymnast presents with Radial physis pain, Imaging confirms the stress injury, and the feared complication is Positive ulnar variance from premature physeal arrest.
LOADRisk Factors
Hook:High LOAD on an open physis is the recipe for gymnast's wrist - the greater the training volume and the longer the delay, the worse the outcome.
RESTManagement Steps
Hook:REST is literally the treatment - Reduce loading, Evaluate with MRI, Splint if needed, Track ulnar variance. The mnemonic IS the management plan.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old female competitive gymnast presents with a 3-month history of bilateral dorsal wrist pain, worse during vault and floor exercises. Her coach says she has been training 22 hours per week. On examination, there is tenderness directly over the distal radial physis bilaterally and pain on axial compression of the wrist in hyperextension. Discuss your diagnosis, investigation, and management.”
“A 13-year-old gymnast was diagnosed with gymnast's wrist 18 months ago and was treated with activity modification. She returns with persistent ulnar-sided wrist pain. Serial radiographs now show positive ulnar variance of 4 mm, increased from 1 mm at diagnosis. The distal radial physis appears closed on the affected side. Discuss your assessment and management.”
“The examiner shows you a diagram of the distal radial physis and asks you to describe the anatomy of the growth plate, explain why the physis is vulnerable to stress injury in gymnasts, and contrast this with an acute Salter-Harris fracture.”
What It Is
- Repetitive stress injury of the open distal radial physis in young gymnasts
- Not an acute Salter-Harris fracture - chronic cumulative microtrauma
- Most common overuse wrist injury in competitive gymnasts
- Up to 50% of young high-level gymnasts show radiographic physeal changes
Clinical Presentation
- Age 10-14, bilateral dorsal wrist pain on loading
- Tender distal radial physis, pain on axial compression in hyperextension
- Always examine both wrists (bilateral involvement common)
- Training more than 15-20 hours per week is the key risk factor
Investigation
- PA + lateral wrist X-ray: physeal widening, irregularity, cysts, ulnar variance
- MRI if X-ray normal: physeal widening + bone marrow oedema = diagnosis
- Measure ulnar variance on neutral-rotation PA view and track serially
- MRI detects stress injury BEFORE radiographic changes appear
Management
- Activity modification (reduce/stop wrist loading) is the mainstay
- Cast or splint 4-6 weeks if rest alone fails
- Monitor ulnar variance serially for premature physeal arrest
- Surgery (ulnar shortening or epiphysiodesis) for progressive positive ulnar variance
Complications
- Premature physeal arrest leading to progressive positive ulnar variance
- Ulnar impaction syndrome and TFCC tears
- Recurrence on return to sport if loading is not modified
- Extended absence from sport (psychological and competitive impact)
Evidence
Gymnast's Wrist: Comprehensive Review of Pathophysiology, Diagnosis and Management
- Comprehensive review of distal radial physeal stress syndrome in gymnasts, covering epidemiology, pathomechanics, imaging, and management
- Up to 50% of competitive young gymnasts demonstrate radiographic abnormalities of the distal radial physis on screening studies
- The mechanism is repetitive compressive loading across the wrist during weight-bearing gymnastics skills, transmitting 2 to 4 times body weight through the distal radial physis
- Management is primarily non-operative with activity modification; surgical intervention is reserved for established physeal arrest with progressive positive ulnar variance
Semi-Quantitative Dixon MRI Assessment of Stress-Related Bone Marrow Oedema in Gymnasts' Wrists
- Developed and validated a semi-quantitative Dixon MRI method for assessing stress-related bone marrow oedema in the wrists of young gymnasts
- Symptomatic gymnasts showed significantly higher water signal fractions in regions of interest adjacent to the distal radial physis compared with asymptomatic gymnasts and non-gymnasts
- Even asymptomatic gymnasts demonstrated measurable MRI changes compared with non-gymnasts, suggesting subclinical physeal stress
- Dixon MRI provides a reproducible, quantitative tool for detecting and monitoring physeal stress changes before they become symptomatic
3D Assessment of Physeal Volume on MRI as a Biomarker for Distal Radial Physeal Damage in Gymnasts
- Used 3D MRI segmentation to measure distal radial physeal volume in symptomatic gymnasts, asymptomatic gymnasts, and non-gymnast controls
- Symptomatic gymnasts had significantly larger distal radial physeal volumes than both asymptomatic gymnasts and controls, reflecting physeal widening from stress injury
- 3D physeal volume correlated with skeletal age and training load, providing an objective biomarker for physeal stress injury severity
- The study demonstrated a dose-response relationship: greater cumulative wrist loading was associated with larger physeal volumes
Wrist Pain, Distal Radial Physeal Injury, and Ulnar Variance in Young Gymnasts
- Prospective study of 44 young female gymnasts examining the relationship between wrist pain, distal radial physeal injury on radiographs, and ulnar variance
- Gymnasts with radiographic physeal abnormalities had significantly more wrist pain than those without physeal changes
- Positive ulnar variance was associated with both physeal injury and wrist pain, supporting the link between repetitive loading, physeal damage, and altered forearm mechanics
- Training intensity and duration of participation were significant risk factors for both physeal injury and positive ulnar variance