Insertional Achilles Tendinopathy | Pump Bump | Retrocalcaneal Bursitis
- Haglund = posterosuperior calcaneal prominence, first described by Patrick Haglund in 1928
- Pump bump = colloquial term for Haglund driven by rigid heel-counter friction in dress shoes
- Three coexisting pathologies: BONY prominence + BURSITIS + TENDINOPATHY
- Eccentric loading (Alfredson) is less effective for insertional than midportion tendinopathy
- Surgical ostectomy typically 3-5 mm; reattach Achilles with suture anchors if tendon detached
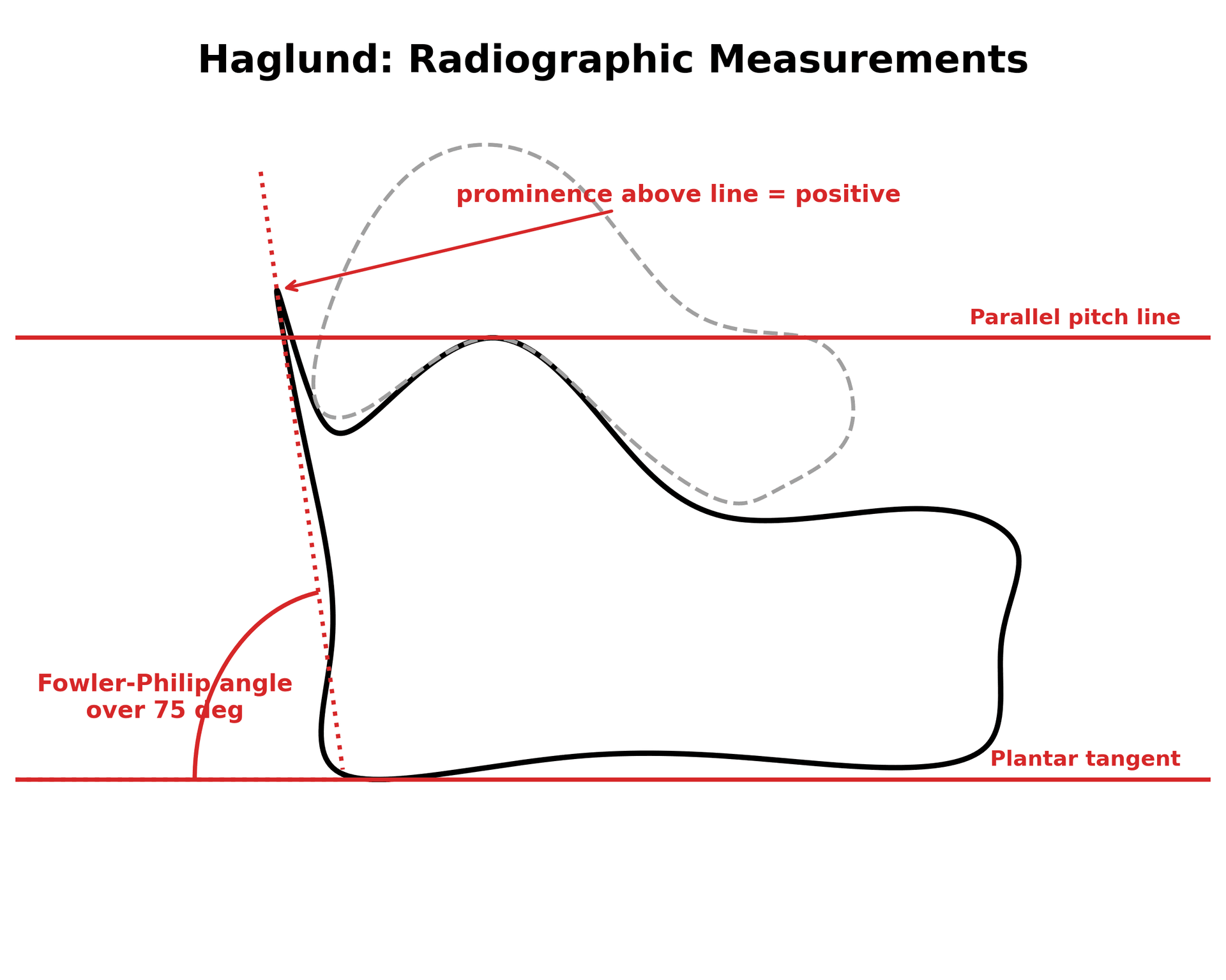
- “Lateral X-ray: parallel pitch lines define the Haglund prominence; Fowler-Philip angle over 75 degrees suggests Haglund
- “Two-finger squeeze at the insertion: mediolateral pinch tenderness implicates retrocalcaneal bursa
- “Always assess cavus foot, gastrocnemius equinus, and FHL tendinopathy in the same consultation
- “Central tendon-splitting approach preferred for combined tendon and bony pathology
- “Baxter's nerve (first branch of lateral plantar) entrapment can mimic Haglund — examine the medial heel
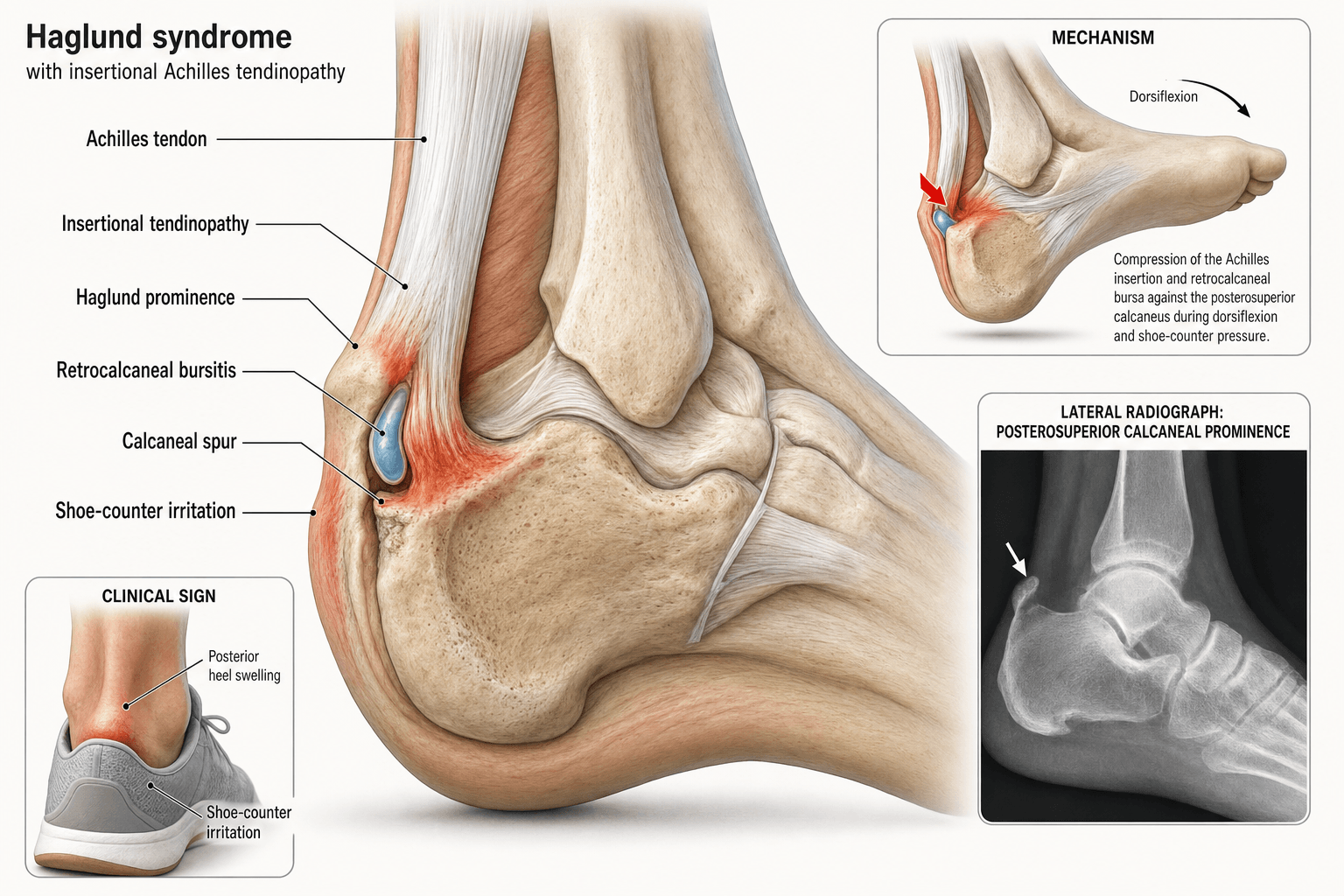
Haglund deformity = posterosuperior calcaneal prominence at the Achilles insertion. The retrocalcaneal bursa sits between the anterior distal Achilles and the calcaneus; the subcutaneous bursa lies between the tendon and the skin.
Retrocalcaneal bursitis = mediolateral pinch pain just above the insertion. Insertional tendinopathy = pain on compressing the tendon with the ankle plantarflexed, with morning stiffness and painful heel raise.
Parallel pitch lines (Pavlov): draw the inferior calcaneal line and a parallel line through the posterosuperior tubercle. If the bony corner projects above the superior line, the calcaneus is too tall. Fowler-Philip angle over 75 degrees supports Haglund.
Remove the prominent bone (3-5 mm) and decompress the bursa. Address tendon pathology with debridement, reattachment through bone anchors, and central tendon splitting if calcified. Address equinus if present.
- Diagnosis
- Retrocalcaneal bursitis (USS or MRI)
- Treatment
- Heel lift, open-back shoes, NSAIDs, bursal injection
- Key Pearl
- Bursitis can occur without Haglund
- Diagnosis
- Haglund deformity (X-ray, parallel pitch lines)
- Treatment
- Footwear, heel lift, eccentric, then ostectomy
- Key Pearl
- Address bone and bursa; tendon often preserved
- Diagnosis
- Insertional Achilles tendinopathy (MRI or USS)
- Treatment
- Modified eccentric, ESWT, debridement with reattachment
- Key Pearl
- Tendon detachment and anchor reattachment if surgery
- Diagnosis
- MRI: intrasubstance signal, calcific deposits, partial tear
- Treatment
- Detachment, debridement, FHL transfer if extensive
- Key Pearl
- Endoscopic or open central tendon splitting both valid
ECCENTRICAlfredson Eccentric Protocol
Hook:ECCENTRIC = 9 steps to Alfredson's heavy-load protocol!
OSTEOTOMYSurgical Debridement Steps
Hook:OSTEOTOMY = the 9 surgical steps for combined Haglund and insertional tendinopathy!
Overview and Epidemiology
Haglund syndrome and insertional Achilles tendinopathy are grouped together because they coexist in 60-70 percent of posterior heel pain presentations. Conservative care fails in roughly 25-50 percent of insertional cases, and these are the patients who present for surgical opinion. Distinguishing pure Haglund (bone and bursa) from insertional tendinopathy (tendon-driven) changes both the conservative algorithm and the surgical plan.
- Age: peak 30-50 years; second smaller peak in active adolescents (Sever-type)
- Sex: women more often affected (pump bump from rigid heel counters)
- Activity: runners (insertional), walkers in tight dress shoes (Haglund)
- Foot shape: cavus, varus heel, Haglund-shaped calcaneus (Fowler-Philip over 75 degrees)
- Tightness: gastrocnemius-soleus equinus increases impingement
- Prevalence: insertional Achilles tendinopathy accounts for 20-25 percent of all Achilles tendon pain
- Recurrence: 25 percent chronic after first-line conservative care
- Surgical volume: 5-10 percent eventually undergo surgery
- Time to recovery: 6-9 months for full return to running post-operatively
- Quality of life: VISA-A scores commonly 50-60/100 at presentation
Pathophysiology
Haglund syndrome is best understood as a triad:
- Bony: posterosuperior calcaneal prominence (Haglund deformity) impinges on the anterior distal Achilles
- Bursal: retrocalcaneal and (or) superficial subcutaneous bursa inflamed by friction and pressure
- Tendon: insertional Achilles tendinopathy with collagen disorganisation, neovascularisation, and (in chronic cases) calcification
Treating only one component and ignoring the others leads to recurrent symptoms.
- Driver
- Posterosuperior calcaneal shape
- Histology
- Normal bone with prominent convexity
- When Present
- Lateral X-ray, parallel pitch lines
- Driver
- Mechanical impingement in dorsiflexion
- Histology
- Bursal hypertrophy, fibrin, inflammatory cells
- When Present
- MRI: fluid crescent anterior to tendon
- Driver
- Skin pressure from shoe counter
- Histology
- Lobular vascular proliferation
- When Present
- Posterior skin swelling, redness
- Driver
- Repetitive tensile load in hypovascular zone
- Histology
- Disorganised collagen, mucoid change, neovessels
- When Present
- MRI: intrasubstance signal, thickening
- Driver
- Chronic tendinopathy, dystrophic calcification
- Histology
- Hydroxyapatite in degenerated tendon
- When Present
- X-ray: bony spur at insertion
Hypovascular zone: 2-7 cm above insertion is a watershed area; insertional fibres have a separate poorer blood supply
Repetitive load: collagen microfailure outstrips repair
Neovascularisation: abnormal vessels grow with accompanying nerves (substance P positive) — target for sclerosing injections
Calcification: end-stage finding, often with intratendinous bone formation
Dorsiflexion: the prominent calcaneal corner drives into the anterior Achilles
Shoe counter: rigid backing compresses skin and superficial bursa
Equinus: limited dorsiflexion means more impingement per step
Cavus and varus: hindfoot varus loads the lateral insertion more
Classification and Types
Classification by Pathology Present
- Bone
- Prominent
- Bursa
- Inflamed
- Tendon
- Normal
- Treatment
- Ostectomy and bursectomy
- Bone
- Prominent
- Bursa
- Inflamed
- Tendon
- Degenerated
- Treatment
- Ostectomy, debridement, reattachment
- Bone
- Normal
- Bursa
- Variable
- Tendon
- Degenerated or calcified
- Treatment
- Eccentric, ESWT, debridement only
- Bone
- Variable
- Bursa
- Variable
- Tendon
- Partial tear plus calcification
- Treatment
- Debridement, reattachment, FHL transfer
Anatomical classification drives the choice between simple ostectomy and combined tendon reconstruction.
Clinical Assessment
- Pain location: posterior heel, at or just above the Achilles insertion
- Aggravating: dorsiflexion (stairs, hills), rigid shoe backs, prolonged standing
- Relieving: open-back shoes, heel lifts, rest, NSAIDs
- Morning stiffness: classic for insertional tendinopathy (not for pure bursitis)
- Shoe wear history: tight dress shoes, ice skates, ski boots
- Activity history: running mileage, hill work, sudden spike in load
- Inspect: posterosuperior bump, erythema, swelling, callus, pump-bump sign
- Palpate: bony prominence, retrocalcaneal bursa (medial-lateral pinch), Achilles insertion tenderness
- Two-finger squeeze: pincer-like tenderness of bursa and tendon
- Range of motion: dorsiflexion, Silfverskiold test for gastrocnemius equinus
- Strength: single-leg heel raise (often weak, painful in chronic tendinopathy)
- Neurovascular: sural nerve, Baxter's nerve (medial heel) palpation
The first branch of the lateral plantar nerve (Baxter's nerve) runs between the abductor hallucis and quadratus plantae and can be entrapped by a hypertrophied abductor hallucis, presenting as chronic medial heel pain. Distinguishing Baxter's neuropathy from Haglund and insertional tendinopathy matters: nerve-targeted therapy (release) differs from Achilles-targeted therapy. Always examine for Tinel sign over the medial heel, weakness of abductor digiti minimi, and burning paraesthesia.
- Pain site
- Posterosuperior corner
- Discriminating finding
- Visible and palpable bony bump
- Key test
- Lateral X-ray (parallel pitch lines)
- Pain site
- Achilles insertion, centred
- Discriminating finding
- Morning stiffness, tender tendon
- Key test
- MRI: intrasubstance signal at insertion
- Pain site
- Anterior to Achilles, deep
- Discriminating finding
- Pain on deep pinch, no skin redness
- Key test
- MRI: crescent of fluid anterior to tendon
- Pain site
- Posterior, superficial
- Discriminating finding
- Skin erythema, fluctuant swelling
- Key test
- Clinical, ultrasound confirms
- Pain site
- Medial heel, below calcaneus
- Discriminating finding
- Burning, Tinel sign medial heel
- Key test
- EMG, diagnostic injection
- Pain site
- Lateral hindfoot
- Discriminating finding
- Burning, Tinel behind lateral malleolus
- Key test
- Clinical, diagnostic block
- Pain site
- Within tendon substance
- Discriminating finding
- Bilateral, family history of hyperlipidaemia
- Key test
- Lipid panel, MRI
A useful bedside differentiator: single-finger tenderness at the posterosuperior bony corner suggests Haglund. Two-finger mediolateral pinch tenderness anterior to the tendon at the insertion suggests retrocalcaneal bursitis. Tender, thickened tendon itself with morning stiffness points to insertional tendinopathy. These are not exclusive, but they help stage the pathology and tailor imaging.
The Silfverskiöld test separates an isolated gastrocnemius contracture from a combined gastrocnemius-soleus (true ankle) equinus, which changes the operation. Measure passive ankle dorsiflexion with the subtalar joint held neutral (to lock the midfoot), first with the knee extended and then with the knee flexed to 90 degrees. The gastrocnemius crosses the knee; the soleus does not. Dorsiflexion that is restricted with the knee straight but improves markedly with the knee bent = isolated gastrocnemius tightness — the lesion that drives dorsiflexion impingement in Haglund and the indication for a gastrocnemius recession (e.g. Strayer) rather than a tendo-Achilles lengthening. If dorsiflexion remains limited in both knee positions, the soleus is also tight (combined equinus).
HAGLUNDHaglund Clinical Triad
Hook:HAGLUND = the seven clinical features of posterosuperior heel pain!
Investigations
Imaging Protocol
Views: weight-bearing lateral ankle or calcaneus
Look for: posterosuperior bony prominence, parallel pitch lines, Fowler-Philip angle, intratendinous calcification, posterior calcaneal cyst
Clinical correlation: defines the bone component, guides ostectomy planning
Indication: dynamic assessment of retrocalcaneal bursa, tendon thickening, neovessels
Findings: bursal fluid crescent, tendon thickening greater than 6 mm, hypoechoic areas, neovascularisation on Doppler
Operator dependent, but cheap and readily repeatable
Indication: chronic cases, suspected partial tear, surgical planning
Findings: intrasubstance signal, calcification, partial tear, retrocalcaneal fluid, Kager fat pad oedema
Best test to assess tendon quality and partial tears
Lateral X-ray first. Most Haglund decisions can be made on a good weight-bearing lateral view with the parallel pitch lines drawn. MRI is reserved for cases where tendon quality is unclear (chronic, failed conservative, suspected partial tear) or when the diagnosis is in doubt. Do not MRI every patient with posterior heel pain.
Management Algorithm
Conservative Management (First Line, 6 Months)
Goal: settle bursitis, offload the prominence, restore tendon load tolerance
Conservative Protocol
Footwear: open-back shoes, no rigid counter
Heel lift: 8-12 mm to reduce dorsiflexion impingement
Activity modification: relative rest, avoid hills, stairs, sprinting
Ice: 15 minutes twice daily
Eccentric protocol (Alfredson): modified for insertional — flat ground, no step dorsiflexion stretch
Heavy slow resistance (HSR): 3 sessions per week alternative
Gastrocnemius stretching: 30-second hold, 3 reps, twice daily
NSAIDs: short course for bursitis (avoid long-term)
ESWT (shockwave): 3 sessions, 2000 pulses, moderate energy
Sclerosing injections (polidocanol): for neovessels at the anterior tendon
PRP (autologous blood): 2-3 injections if available, evidence variable
High-volume stripping: for resistant paratendinopathy
Outcome measure: VISA-A score trend (50-60 to greater than 70 considered good response)
Persistent pain, low VISA-A: surgical opinion
Return to running: gradual mileage, no hills initially
For insertional tendinopathy, do not perform the standard Alfredson heel drop off a step (which loads the insertion in dorsiflexion). Instead, use flat-ground heel drops or isometric contractions for the first 4-6 weeks. The standard Alfredson protocol works well for midportion tendinopathy but can aggravate insertional symptoms.
Complications
- Incidence
- 5-15 percent open, less than 2 percent endoscopic
- Risk Factors
- Posterior wound tension, smoking, steroids
- Management
- Meticulous closure, offload, vascularised flap if needed
- Incidence
- 2-5 percent
- Risk Factors
- Lateral dissection too far
- Management
- Identify and protect; neuroma if cut
- Incidence
- 1-3 percent
- Risk Factors
- Early loading, FHL transfer if extensive debridement
- Management
- Cast, surgical repair if complete
- Incidence
- 5-10 percent
- Risk Factors
- Under-resection of posterosuperior corner
- Management
- Revision ostectomy, MRI to assess
- Incidence
- 10-20 percent
- Risk Factors
- Prolonged immobilisation, over-tight reattachment
- Management
- Physiotherapy, heel raise long term
- Incidence
- 1-2 percent
- Risk Factors
- Prolonged immobility, obesity, OCP
- Management
- Mechanical prophylaxis, consider chemical
- Incidence
- 10-15 percent over 5 years
- Risk Factors
- Cavus, equinus, inadequate rehab
- Management
- Footwear, gastrocnemius lengthening, revision
The posterior approach crosses a watershed area with poor skin vascularity and is the most common cause of re-operation. Meticulous technique (no skin tension, full-thickness flaps, careful soft tissue handling, offloading) reduces dehiscence. Smokers and diabetics are at the highest risk. Endoscopic surgery trades wound risk for technical difficulty and limited tendon visualisation.
Outcomes and Prognosis
- Time to effect
- 12 weeks
- Success
- 60-70 percent in midportion, 30-50 percent in insertional
- Long-term
- Best in compliant, non-calcified cases
- Time to effect
- 8-12 weeks
- Success
- 50-60 percent improvement in pain scores
- Long-term
- Useful adjunct, not stand-alone in severe cases
- Time to effect
- 6-8 weeks
- Success
- 40-50 percent for neovessel-positive cases
- Long-term
- Evidence still limited
- Time to effect
- 6-9 months
- Success
- 85-90 percent good-to-excellent at 2 years
- Long-term
- Gold standard for failed conservative
- Time to effect
- 3-6 months
- Success
- 80-85 percent for pure Haglund
- Long-term
- Less wound risk, limited for tendon work
Favours good outcome: short symptom duration, single pathology (bone only or tendon only), compliant eccentric loading, normal BMI, non-smoker, no diabetes.
Favours poor outcome: long-standing symptoms, intratendinous calcification, partial tear over 50 percent, smoking, diabetes, obesity, equinus not addressed.
Key threshold: 6 months of structured conservative care — earlier surgery does not improve outcomes and may worsen them.
Guidelines, Registries & Global Practice
- Insertional Achilles tendinopathy accounts for 20-25 percent of all Achilles tendon pain in running populations across regions
- Pure Haglund is more common in women wearing rigid dress shoes and in ice-hockey, skiing, and football populations
- Incidence of insertional tendinopathy in runners is roughly 10 percent per year in published cohorts (UK, US, Australian, Dutch registries)
- Bilateral involvement occurs in up to 40 percent of insertional cases — always examine both sides
- High-resource: ESWT, MRI, ultrasound-guided injection, and endoscopic surgery are widely available
- Limited-resource: structured eccentric loading, footwear advice, and open ostectomy remain the backbone
- Universal principle: outcome depends far more on patient compliance with loading and footwear than on the technology used
- Surgery: open central tendon splitting is universally available; endoscopic ostectomy is concentrated in specialist foot and ankle centres
- Diagnosis emphasis
- Clinical diagnosis, lateral X-ray to define Haglund, MRI for surgery planning
- First-line treatment
- Footwear, heel lift, modified Alfredson, ESWT
- Surgery threshold
- Failed 6 months conservative + low VISA-A
- Diagnosis emphasis
- Clinical plus lateral X-ray, MRI for chronic or surgical cases
- First-line treatment
- Activity modification, modified eccentric, ESWT, PRP optional
- Surgery threshold
- Failed conservative with persistent functional limitation
- Diagnosis emphasis
- Combined clinical and imaging diagnosis; ultrasound and MRI equivalent
- First-line treatment
- Eccentric loading, HSR, ESWT, orthotics
- Surgery threshold
- Central tendon splitting with anchor reattachment for combined cases
- Diagnosis emphasis
- Weight-bearing lateral X-ray mandatory; MRI for surgical planning
- First-line treatment
- Eccentric loading, footwear, ESWT
- Surgery threshold
- Open or endoscopic ostectomy based on tendon involvement
There is no dedicated arthroplasty or implant registry for Haglund syndrome (no implants used). The evidence base is dominated by small case series and operative-technique reviews, with only a few high-quality RCTs (Beyer 2015 for HSR vs eccentric; Rompe for ESWT). Registry data from the National Joint Registry (UK), AJRR (US), and AOANJRR (Australia) do not capture this condition. Guidance is therefore principle-based: diagnose with a lateral X-ray, treat the triad, fail conservative for 6 months before surgery, and address equinus when present.
Record in every posterior heel pain consultation:
- Components present (bone, bursa, tendon) with explicit clinical findings
- Silfverskiold test result and equinus assessment
- X-ray findings (parallel pitch lines, Fowler-Philip angle, calcification)
- Conservative plan and duration (footwear, heel lift, modified Alfredson)
- Outcome measure (VISA-A) at baseline and follow-up
- Surgical threshold discussed if conservative fails
Posterior heel pain is a recurring source of complaints worldwide. A clear, well-documented conservative trial protects both patient and clinician.
Controversies & Areas of Uncertainty
The standard Alfredson protocol was designed for midportion disease and may aggravate insertional symptoms because of dorsiflexion loading. Modified flat-ground variants, HSR, and isometrics all have advocates, but no head-to-head trial exists for the insertional subtype.
Endoscopic ostectomy reduces wound complications but limits tendon visualisation. Open central tendon splitting is more versatile for combined cases. Choice is driven by surgeon experience and tendon involvement, not by strong comparative evidence.
FHL transfer is reserved for very large insertional defects (over 50 percent) or revision cases. Outcomes are good but the donor morbidity (loss of hallux plantarflexion strength) is real. Indication is not standardised.
Platelet-rich plasma and autologous blood injections are widely marketed, but the randomised evidence does not show consistent benefit over placebo for insertional tendinopathy. Consider only within trials or for refractory cases after shared decision-making.
MCQ Practice Points
Q: What is the Haglund deformity and where does it sit? A: Posterosuperior bony prominence of the calcaneus at the Achilles tendon insertion. It is the bony component of the Haglund syndrome triad, first described by the Swedish orthopaedist Patrick Haglund in 1928.
Q: How do you define the Haglund deformity on a lateral X-ray? A: Parallel pitch lines (Pavlov). Draw the inferior calcaneal line and a parallel line through the posterosuperior tubercle. If the bony corner projects above the superior line, the calcaneus is too tall. A Fowler-Philip angle over 75 degrees supports Haglund but is less specific.
Q: Why does insertional Achilles tendinopathy respond less well to standard Alfredson eccentric loading? A: Because the step in the classic Alfredson protocol loads the insertion in maximal dorsiflexion, which compresses the tendon against the posterosuperior calcaneal corner. The modified protocol uses flat-ground heel drops or isometric contractions that avoid this impingement.
Q: What are the components of surgical management for combined Haglund and insertional tendinopathy? A: (1) Posterior midline or paratendinous approach; (2) central tendon splitting; (3) debridement of calcific and necrotic tendon; (4) 3-5 mm calcaneal ostectomy; (5) bursectomy; (6) Achilles reattachment with two suture anchors in equinus; (7) consider gastrocnemius recession for equinus.
Q: What is the minimum duration of structured conservative care before offering surgery? A: At least 6 months of structured, compliant loading (modified eccentric or HSR), footwear modification, ESWT, and activity change. Earlier surgery does not improve outcomes and may worsen them.
Q: How do you distinguish Haglund/insertional tendinopathy from Baxter's nerve entrapment? A: Baxter's nerve (first branch of the lateral plantar) entrapment presents with medial heel burning, Tinel sign over the medial heel, and weakness of the abductor digiti minimi. Haglund/insertional tendinopathy presents with posterior heel pain, bony bump, and tendon tenderness. Nerve-targeted therapy (release) differs from Achilles-targeted therapy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old recreational marathon runner presents with 8 months of posterior right heel pain. He can no longer run uphill without pain. He has tried rest, NSAIDs, and a heel lift. On examination, there is a tender posterosuperior bump, painful mediolateral squeeze at the insertion, and a single-leg heel raise reproduces pain. Silfverskiold is positive for gastrocnemius tightness. Lateral X-ray shows a prominent posterosuperior corner and parallel pitch lines positive. What is your diagnosis and management?”
“A 32-year-old woman presents with 4 months of bilateral posterior heel pain, worse when she wears work heels. She has a visible posterosuperior bump on each heel, erythema over the bump, and tenderness on mediolateral pinch. Single-leg heel raise is mildly painful but strong. Silfverskiold is normal. Lateral X-ray shows a positive parallel pitch lines sign. She has tried gel heel cups. How do you manage this?”
Key Anatomy and Pathology
- Haglund = posterosuperior calcaneal prominence at the Achilles insertion
- Three coexisting pathologies: BONY prominence + BURSITIS + TENDINOPATHY
- Retrocalcaneal bursa lies between anterior Achilles and calcaneus
- Insertional tendon is a watershed area with poor blood supply
Diagnosis
- Lateral X-ray with parallel pitch lines (Pavlov) defines Haglund
- Fowler-Philip angle over 75 degrees supports Haglund
- Two-finger mediolateral squeeze: retrocalcaneal bursitis
- MRI for chronic or surgical cases (tendon quality, partial tear)
Treatment Algorithm
- First line: footwear (open-back), heel lift 8-12 mm, NSAIDs
- Loading: modified Alfredson on flat ground or HSR for 12 weeks
- Adjuncts: ESWT, sclerosing injection for neovessels
- Surgery: ostectomy plus tendon reattachment if conservative fails over 6 months
Eccentric Pearls
- Step Alfredson works for midportion, not for insertional
- Insertional: flat-ground heel drops or isometrics first
- 180 reps per day is the original protocol; HSR is 3 times per week alternative
- Compliance is the strongest predictor of outcome
Surgical Pearls
- 3-5 mm calcaneal ostectomy removes the impinging corner
- Central tendon splitting accesses the insertional pathology
- Reattach with 2 suture anchors in equinus, then bring to neutral in boot
- Address gastrocnemius equinus (Silfverskiold) with recession when positive
Complications
- Posterior wound dehiscence is the most common re-operation cause (5-15 percent open)
- Sural nerve injury 2-5 percent, identify and protect
- Achilles re-rupture 1-3 percent, longer in FHL transfer cases
- Recurrence 10-15 percent over 5 years if equinus and footwear not addressed
Evidence Base and Key Trials
Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis
- Prospective cohort of 30 recreational athletes with midportion Achilles tendinosis
- Heavy-load eccentric protocol: 180 reps per day (3 sets of 15, twice daily) on a step
- All 30 patients returned to pre-injury activity at 12 weeks with no further pain
- Satisfaction was high despite continued neovascularisation on follow-up imaging
Heavy Slow Resistance Versus Eccentric Training as Treatment for Achilles Tendinopathy: A Randomized Controlled Trial
- RCT of 58 patients with midportion Achilles tendinopathy randomised to Alfredson eccentric or heavy slow resistance (HSR) training
- Both groups improved significantly in VISA-A and pain scores at 12 and 52 weeks
- HSR group had higher patient satisfaction at 52 weeks with only 3 sessions per week
- No difference in pathology thickness on ultrasound between groups at 52 weeks
Surgical strategies: insertional Achilles tendinopathy
- Technique review and clinical series of central tendon splitting with calcaneal ostectomy
- Approach: midline or medial paratendinous, full-thickness flap, longitudinal split of the tendon
- Ostectomy 3-5 mm, debridement of calcific and necrotic tissue, reattachment with two suture anchors
- High satisfaction (greater than 80 percent) in chronic insertional cases failing conservative care
Posterior heel pain associated with a calcaneal step and Achilles tendon calcification
- Early clinicopathological series linking posterosuperior calcaneal shape to insertional Achilles pathology
- Described the calcaneal step: abrupt change in cortical contour at the Achilles insertion
- Histology: insertional calcification and mucoid degeneration of tendon at the bone-tendon junction
- Suggested surgical resection of the step and reattachment of the tendon for chronic cases