Sports Medicine | FAI Treatment | Labral Repair | Traction Essential | Nerve Protection Critical
FEMOROACETABULAR IMPINGEMENT (FAI) CLASSIFICATION
Critical Must-Knows
- Cam = femoral-based (alpha angle greater than 55°); Pincer = acetabular-based (overcoverage)
- Mixed FAI is most common (80%) - address both cam and pincer components
- Traction essential for central compartment - 25-50lbs force, break seal with internal rotation
- Maximum 2 hours traction - risk of nerve injury (pudendal, sciatic) increases significantly
- Lateral femoral cutaneous nerve at risk with anterolateral portal
Clinical Pearls
- "Alpha angle greater than 55° on axial MRI indicates cam morphology
- "Positive anterior impingement test (FADIR) is most sensitive clinical sign
- "Always break the vacuum seal with longitudinal traction plus internal rotation before distraction
- "Lateral femoral cutaneous nerve crosses 1-2cm distal and medial to ASIS
Clinical Imaging
Imaging Gallery
Arthroscopic Labral Repair
Critical Hip Arthroscopy Exam Points
Traction Complications
Keep traction time and force to a minimum - traction time greater than 60 minutes significantly raises the complication rate (Larson 2016). Pudendal (perineal) numbness occurs in about 1.4% and the lateral femoral cutaneous nerve is the most commonly affected nerve overall (16.5%, persisting beyond 6 months in only 1.6%). Use a well-padded perineal post and release traction intermittently in prolonged cases.
Portal Safety
Lateral femoral cutaneous nerve crosses 1-2cm distal and medial to ASIS - at risk with anterolateral portal. Superior gluteal nerve can be injured with proximal portal placement. Establish portals under fluoroscopic guidance with air arthrogram.
Alpha Angle
Cam morphology defined as alpha angle greater than 55° on axial MRI or cross-table lateral radiograph. Measured as angle between femoral neck axis and point where head-neck junction exceeds head radius. Normal is less than 50°.
Central vs Peripheral
Central compartment (under traction): labrum, acetabular cartilage, ligamentum teres, femoral head. Peripheral compartment (without traction): head-neck junction, medial synovial fold, zona orbicularis. Both compartments need assessment.
At a Glance - FAI Types and Treatment
| FAI Type | Pathoanatomy | Imaging Finding | Surgical Treatment |
|---|---|---|---|
| Cam | Femoral head-neck asphericity (bump) | Alpha angle greater than 55° | Osteochondroplasty (bump resection) |
| Pincer | Acetabular overcoverage | CE angle greater than 40°, crossover sign | Rim trimming plus or minus labral repair |
| Mixed | Both cam and pincer (80% of cases) | Combined findings | Address both components |
CAM vs PINCERFAI Types - 'CAM vs PINCER'
| C | Curved bump Aspherical femoral head-neck junction |
| A | Alpha angle Greater than 55° on axial imaging |
| M | Male predominant Young athletic males most common |
| P | Pinch at rim Acetabular overcoverage pinches labrum |
| I | Increased CE angle Center-edge angle greater than 40° |
| N | Negative crossover Actually POSITIVE crossover sign on AP |
| C | Curved bump Aspherical femoral head-neck junction | M | Male predominant Young athletic males most common | I | Increased CE angle Center-edge angle greater than 40° |
| A | Alpha angle Greater than 55° on axial imaging | P | Pinch at rim Acetabular overcoverage pinches labrum | N | Negative crossover Actually POSITIVE crossover sign on AP |
Hook:CAM = bump on femoral head (young males). PINCER = rim pinches labrum (middle-aged females)!
AAPHip Arthroscopy Portals - 'AAP'
| A | Anterolateral Primary viewing portal, 1cm anterior/superior to GT tip |
| A | Anterior Primary working portal, at ASIS level at GT line |
| P | Posterolateral Posterior viewing/working, 1cm posterior/superior to GT |
| A | Anterolateral Primary viewing portal, 1cm anterior/superior to GT tip |
| A | Anterior Primary working portal, at ASIS level at GT line |
| P | Posterolateral Posterior viewing/working, 1cm posterior/superior to GT |
Hook:AAP = Anterolateral, Anterior, Posterolateral - the three standard hip arthroscopy portals!
SFLPNerves at Risk - 'SFLP'
| S | Sciatic Posterior, at risk with excessive traction or posterior portals |
| F | Femoral Anterior, protected by iliopsoas - rarely injured |
| L | Lateral femoral cutaneous Most commonly affected nerve (16.5%), causes meralgia paraesthetica |
| P | Pudendal Perineal post compression, about 1.4% transient neurapraxia |
| S | Sciatic Posterior, at risk with excessive traction or posterior portals | L | Lateral femoral cutaneous Most commonly affected nerve (16.5%), causes meralgia paraesthetica |
| F | Femoral Anterior, protected by iliopsoas - rarely injured | P | Pudendal Perineal post compression, about 1.4% transient neurapraxia |
Hook:SFLP = Sciatic, Femoral (rare), Lateral cutaneous (most common), Pudendal (traction)!
2-25-6Traction Safety - '2-25-6'
| 2 | Two hours maximum Maximum recommended traction time |
| 25 | Twenty-five pounds minimum Minimum force to break seal (25-50lbs) |
| 6 | Six millimeters Minimum joint distraction for safe access |
| 2 | Two hours maximum Maximum recommended traction time |
| 25 | Twenty-five pounds minimum Minimum force to break seal (25-50lbs) |
| 6 | Six millimeters Minimum joint distraction for safe access |
Hook:Remember 2-25-6: 2 hours max, 25lbs minimum, 6mm distraction needed!
Overview
Hip arthroscopy is a minimally invasive surgical technique for diagnosing and treating intra-articular and periarticular hip pathology. The primary indication is femoroacetabular impingement (FAI) with associated labral tears, though indications continue to expand.
Epidemiology of FAI:
- Imaging morphology is common and often asymptomatic: a systematic review of 2114 asymptomatic hips found cam morphology in 37% overall - 54.8% in athletes versus 23.1% in the general population (Frank 2015)
- Symptomatic FAI (FAI syndrome): Presents in athletes and active individuals, typically 20-45 years; diagnosis requires symptoms plus signs plus imaging (Warwick Agreement 2016)
- Sex distribution: Cam more common in males; Pincer more common in females; Mixed most common overall
- Athletic association: High-risk flexion-loading sports include ice hockey, football/soccer, martial arts, ballet and Australian Rules football
Pathophysiology:
- Cam mechanism: Aspherical femoral head-neck junction causes outside-in abrasion of acetabular cartilage during flexion and internal rotation. The abnormal convexity shears against the labrum and cartilage.
- Pincer mechanism: Acetabular overcoverage causes labral crush injury and countrecoup lesions on posterior acetabulum. Overcoverage may be global (coxa profunda) or focal (acetabular retroversion).
- Natural history: Untreated FAI leads to progressive cartilage damage and eventual osteoarthritis
Indications for Hip Arthroscopy:
- Femoroacetabular impingement (cam, pincer, or mixed)
- Labral tears
- Chondral lesions (debridement, microfracture)
- Ligamentum teres tears
- Loose bodies
- Synovial disorders (PVNS, synovial chondromatosis)
- Hip instability (capsular plication)
- Iliopsoas tendon release
Pathophysiology and Mechanisms
Hip Joint Anatomy: The hip is a ball-and-socket joint with inherent bony stability enhanced by the acetabular labrum, capsule, and ligaments. The femoral head is covered by hyaline cartilage except at the fovea (ligamentum teres attachment).
Labrum:
- Fibrocartilaginous ring attached to the acetabular rim
- Deepens the acetabulum by 21% and increases surface area by 28%
- Creates a suction seal that provides joint stability
- Blood supply from superior gluteal, inferior gluteal, and obturator vessels
- Vascularity is better peripherally than centrally (important for repair)
Capsule and Ligaments:
- Iliofemoral ligament (Y-ligament of Bigelow): strongest ligament, anterior
- Pubofemoral ligament: inferior, limits abduction
- Ischiofemoral ligament: posterior, limits internal rotation
- Zona orbicularis: circular fibers around femoral neck
Neurovascular Structures:
- Femoral neurovascular bundle: anterior, protected by iliopsoas
- Lateral femoral cutaneous nerve: crosses 1-2cm distal and medial to ASIS
- Superior gluteal nerve: exits above piriformis, at risk with proximal portals
- Sciatic nerve: posterior, at risk with traction and posterior portals
FAI Pathoanatomy:
Cam Morphology:
- Abnormal bump at femoral head-neck junction (anterosuperior most common)
- Results from developmental abnormality during skeletal maturation
- Alpha angle greater than 55° is diagnostic
- Causes outside-in cartilage abrasion during flexion/internal rotation
Pincer Morphology:
- Acetabular overcoverage (global or focal)
- Center-edge angle greater than 40° suggests overcoverage
- Crossover sign on AP pelvis indicates focal retroversion
- Causes labral crush injury and countrecoup posterior cartilage damage
Classification
Femoroacetabular Impingement Classification:
Cam-type FAI results from femoral-based pathology where an aspherical femoral head-neck junction (bump) impinges against the acetabular labrum and cartilage during hip flexion and internal rotation.
Key features: Alpha angle greater than 55° on axial imaging. Bump typically anterosuperior. More common in young athletic males. Causes outside-in cartilage abrasion pattern. Treatment involves osteochondroplasty (bump resection) to restore sphericity.
Labral Tear Classification (Seldes):
- Type 1: Detachment of labrum from acetabular cartilage (most common)
- Type 2: Cleavage plane within labral substance
Beck Cartilage Damage Classification:
- Grade 0: Normal cartilage
- Grade 1: Softening (malacia)
- Grade 2: Partial thickness defect
- Grade 3: Full thickness defect
- Grade 4: Exposed subchondral bone
Acetabular Rim Classification:
- Focal pincer: Retroversion of superior acetabulum
- Global pincer: Coxa profunda/protrusio acetabuli
Clinical Assessment
History:
Classic FAI presentation is a young athletic patient with activity-related groin pain, often with clicking, catching, or giving way. Pain typically insidious onset, worse with prolonged sitting, pivoting activities, and hip flexion.
Common symptoms: Deep anterior groin pain (C-sign where patient cups hand over greater trochanter). Pain with prolonged sitting (theater sign). Pain with hip flexion activities (squatting, stairs). Mechanical symptoms (clicking, catching, locking).
Physical Examination:
Observation: Observe gait for Trendelenburg or antalgic pattern. Note pelvic obliquity and limb length. Assess hip flexion contracture.
Range of motion: Compare to contralateral side. FAI typically shows decreased internal rotation in flexion. Measure flexion, extension, abduction, adduction, internal and external rotation.
FADIR Test
The FADIR (anterior impingement) test is the most sensitive clinical test for FAI. Position: supine with hip and knee at 90° flexion, then passively adduct and internally rotate. Positive test reproduces the patient's groin pain. While sensitive (95%), it has low specificity - must correlate with imaging.
Differential Diagnosis of Young-Adult Groin / Hip Pain:
Because cam and pincer morphology is common in asymptomatic people (37% asymptomatic cam in athletes/general population; Frank 2015), FAI syndrome is a clinical diagnosis of exclusion as much as inclusion. Actively exclude these mimics before attributing pain to impingement.
Differentiating FAI Syndrome from Mimics
| Condition | Typical patient / pain | Discriminating feature |
|---|---|---|
| FAI syndrome | Young active adult, deep anterior groin (C-sign), worse sitting/pivoting | Positive FADIR; cam/pincer plus symptoms; greater than 50% relief from intra-articular injection |
| Acetabular dysplasia | Often female, antero-lateral pain, instability/fatigue, micro-instability | Lateral centre-edge angle less than 20-25°; under-coverage (opposite of pincer) |
| Athletic pubalgia / inguinal-related groin pain | Athlete, lower abdominal/adductor-origin pain with sprinting and Valsalva | Tender pubic tubercle/adductor origin; pain NOT reproduced by FADIR; negative injection |
| Hip osteoarthritis | Older patient, stiffness, reduced overall ROM | Joint space narrowing, osteophytes (Tönnis 2 or more); poor arthroscopy candidate |
| Lumbar/L1-L2 referred pain | Back pain, dermatomal radiation, neurological signs | Pain not localised to groin; negative hip provocation; spinal signs positive |
| Greater trochanteric pain / gluteal tendinopathy | Lateral hip pain, tender over trochanter, pain lying on side | Lateral (not groin) tenderness; pain on single-leg stance/resisted abduction |
Investigations
Plain Radiographs:
AP Pelvis: Essential initial view. Assess center-edge angle, crossover sign, posterior wall sign. Must have proper positioning (coccyx 1-3cm above symphysis).
Lateral views: Cross-table lateral (Dunn view) or frog-leg lateral. Assess alpha angle, head-neck offset.
MRI and MR Arthrogram:
Standard MRI: Evaluates labrum, cartilage, and periarticular soft tissues. Axial oblique views best for alpha angle measurement.
MR Arthrogram: Gold standard for labral pathology. Intra-articular gadolinium improves labral tear detection. Sensitivity greater than 90% for labral tears.
Radial MRI: Series of views radiating from femoral neck axis. Best for comprehensive assessment of cam lesion location.
CT Scan:
3D CT: Provides excellent bony detail of cam and pincer morphology. Useful for surgical planning. Less radiation with low-dose protocols.
Diagnostic Injection:
Intra-articular injection of local anesthetic under fluoroscopic guidance can confirm intra-articular source of pain. Greater than 50% pain relief suggests intra-articular pathology.
Non-Operative Management
Indications for Non-Operative Treatment:
- Mild symptoms with minimal functional limitation
- Patient preference
- Significant osteoarthritis (relative contraindication to arthroscopy)
- Medical contraindications to surgery
- Initial management while diagnosis is being confirmed
Non-Operative Protocol:
Activity modification: Avoid aggravating positions (deep flexion, prolonged sitting). Physical therapy: Core and hip strengthening, focus on gluteal activation. NSAIDs: For symptomatic relief. Education: Explain pathophysiology and natural history.
Advance rehabilitation: Progressive hip strengthening program. Sport-specific modification: Identify and modify aggravating activities. Injection therapy: Consider intra-articular corticosteroid if indicated. Reassess: Evaluate response to conservative treatment.
Evaluate response: If improved, continue activity modification and maintenance program. If symptoms persist: Consider surgical intervention if appropriate candidate. Shared decision-making: Discuss risks and benefits of surgery vs continued non-operative care.
Injection Considerations
While intra-articular corticosteroid injections may provide temporary relief, they do not address the underlying mechanical problem. Some evidence suggests repeated injections may negatively affect cartilage and outcomes of subsequent surgery. Use judiciously and primarily as a diagnostic tool.
Management Algorithm
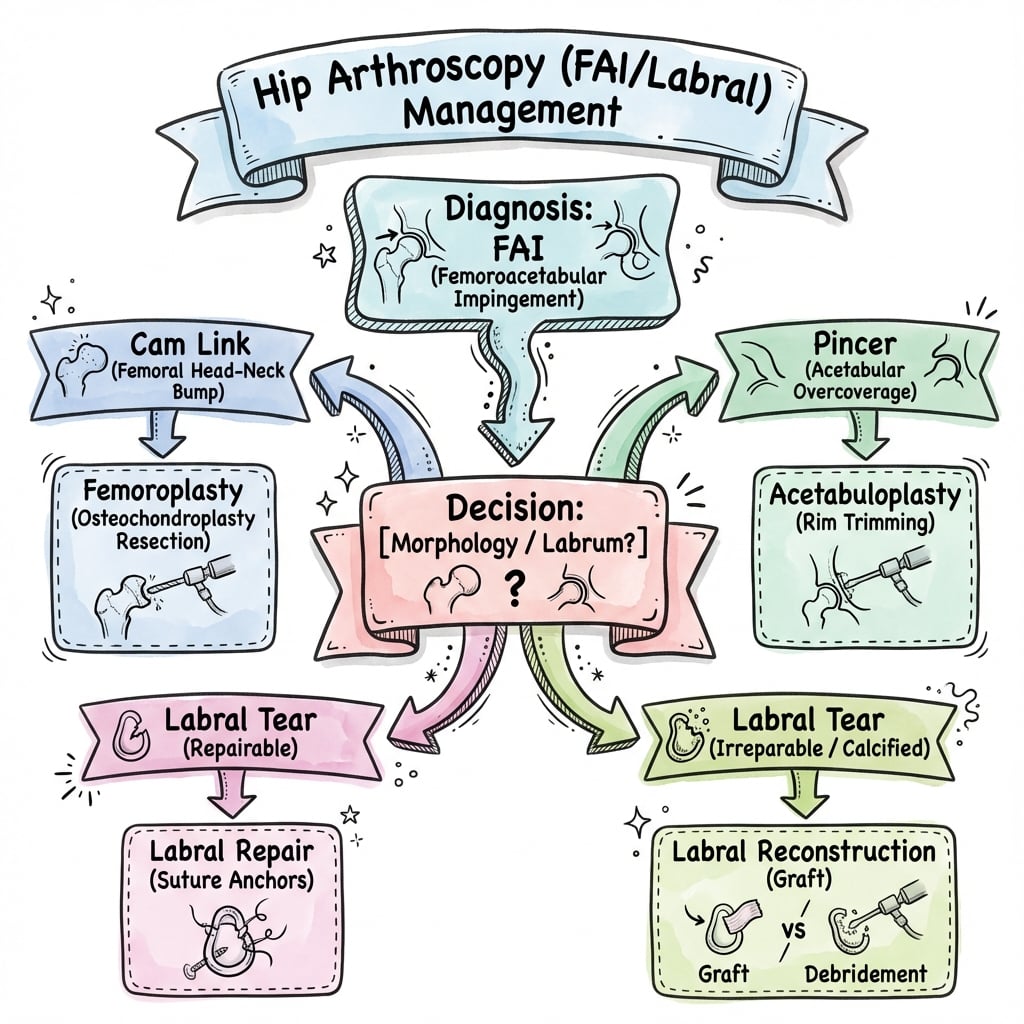
Decision-Making Framework for Hip Arthroscopy:
Clinical Assessment: Positive FADIR test with anterior groin pain in a young active patient. Correlate with imaging findings of cam (alpha greater than 55°) or pincer (CE greater than 40°) morphology. MR arthrogram to assess labrum.
Diagnostic Injection: Greater than 50% pain relief with intra-articular local anesthetic confirms intra-articular source and predicts good surgical outcome.
Key Decision Points:
- Joint space greater than 2mm → Good candidate for arthroscopy
- Joint space less than 2mm with arthritis → Consider arthroplasty
- Positive impingement test + positive injection → Best outcomes
- Mixed FAI → Must address both components
Surgical Management
Patient Positioning:
Supine positioning on fracture table is most common. Patient supine with perineal post well-padded. Operative limb in traction boot. Contralateral limb in padded post or abducted in leg holder.
Advantages: Familiar position, easier fluoroscopy, better anterior access. Disadvantages: Perineal post pressure risk.
Traction and Joint Access:
Traction Requirements:
- Force: 25-50 pounds typically needed
- Technique: Apply longitudinal traction, then internal rotation to break vacuum seal
- Confirmation: Fluoroscopic confirmation of 6mm distraction minimum
- Time limit: Maximum 2 hours - release if prolonged case
Portal Establishment:
Standard Portals:
- Anterolateral (AL): Primary viewing portal, 1cm anterior and superior to greater trochanter tip
- Anterior: Primary working portal, intersection of ASIS horizontal line and GT vertical line
- Posterolateral (PL): 1cm posterior and superior to GT, supplementary viewing/working
Technique: Establish portals under fluoroscopic guidance with air arthrogram. Use spinal needle to confirm trajectory. Make skin incision, then blunt trocar insertion to avoid nerve injury.
Central Compartment Procedures:
- Labral repair: Suture anchors for peripheral labral tears
- Labral debridement: For non-repairable tears
- Acetabular rim trimming: For pincer lesions
- Microfracture: For focal cartilage defects
- Ligamentum teres debridement: For symptomatic tears
- Loose body removal
Peripheral Compartment Procedures:
- Osteochondroplasty: Cam lesion resection to restore head-neck offset
- Capsulotomy management: Repair or plication as needed
- Iliopsoas release: If symptomatic internal snapping hip
Complications
Nerve Injuries:
Nerve Injuries in Hip Arthroscopy
| Nerve | Mechanism | Clinical Finding | Prevention |
|---|---|---|---|
| Lateral femoral cutaneous | Anterior/anterolateral portal injury | Meralgia paraesthetica (lateral thigh numbness) - most common (16.5%) | Portal placement 1-2cm from ASIS, blunt dissection |
| Pudendal nerve | Perineal post pressure / traction (about 1.4%) | Perineal numbness, sexual dysfunction | Well-padded post, intermittent release, minimal traction time |
| Sciatic nerve | Excessive traction, posterior portals | Posterior thigh numbness, foot drop | Limit traction force and time, careful posterior portals |
| Superior gluteal nerve | Proximal portal placement | Gluteus medius weakness, Trendelenburg | Stay distal to piriformis, avoid proximal portals |
Other Complications:
In the largest prospective multicentre series (1615 hips), the overall complication rate was 8.3% with mostly low-grade events; rates below are from that series unless stated otherwise (Larson 2016).
- Fluid extravasation: Risk of abdominal compartment syndrome with prolonged cases (no extra-abdominal extravasation observed in the 1615-hip series)
- Femoral neck fracture / stress fracture: 0.1%; risk from excessive osteochondroplasty (avoid resecting more than ~30% of neck circumference)
- Instability: From excessive rim trimming or unrepaired capsulotomy (no iatrogenic instability in the 1615-hip series)
- Iatrogenic chondral injury: 1.2%; iatrogenic labral puncture: 0.9%
- Heterotopic ossification: 0.8%; NSAID prophylaxis reduces incidence
- Avascular necrosis: Rare (none in the 1615-hip series), associated with lateral epiphyseal vessel damage
- Superficial portal infection: 1.1%
- DVT 0.1% / PE 0.1%: Standard VTE risk-stratified prophylaxis
Traction and Nerve Protection
The lateral femoral cutaneous nerve is the most commonly affected nerve (16.5% transient disturbance, persisting beyond 6 months in only 1.6%); pudendal (perineal) numbness is less common at about 1.4%. The single most important modifiable factor is traction: time greater than 60 minutes significantly raises the complication rate, and pudendal neurapraxia is linked to longer traction. Prevention: well-padded wide perineal post; minimal traction force and time; intermittent release in prolonged cases; consider post-less or lateral positioning.
Rehabilitation
Post-Operative Protocol:
Weight-bearing: Typically 20lbs flat-foot weight-bearing for 2-4 weeks (longer if microfracture). ROM restrictions: Limit hip flexion to 90°, avoid FADIR position for 4-6 weeks. CPM: Consider continuous passive motion machine. Goals: Protect repair, control inflammation, maintain ROM.
Progress weight-bearing: Advance to full as tolerated. ROM: Progress to full ROM. Strengthening: Aquatic therapy, stationary bike, hip strengthening (avoid impingement positions). Goals: Restore ROM, begin strengthening, normalize gait.
Activities: Progress to elliptical, swimming, functional exercises. Strengthening: Progressive resistance training. Sport-specific: Begin sport-specific training at 12+ weeks. Return to sport: Typically 4-6 months depending on procedure and sport.
Procedure-Specific Considerations:
Labral repair:
- Protect repair for 4-6 weeks with ROM restrictions
- Avoid FADIR position during healing
- Full return to sport: 4-6 months
Microfracture:
- Protected weight-bearing 6-8 weeks
- CPM encouraged for cartilage healing
- Return to sport: 6-12 months
Osteochondroplasty alone:
- Earlier weight-bearing (2 weeks)
- Less ROM restriction needed
- Return to sport: 3-4 months
Outcomes and Prognosis
Short-Term Outcomes:
- Patient satisfaction: 85-90% satisfaction at 2 years
- Return to sport: 80-90% return to sport, 70-80% at same level
- Pain improvement: Significant improvement in pain scores (70-80% reduction)
- Functional improvement: Improved modified Harris Hip Score in 85%+
Long-Term Outcomes:
Outcomes by Cartilage Status
| Cartilage Status | Short-term Outcome | Long-term Outcome |
|---|---|---|
| Normal cartilage (Beck 0-1) | Excellent (over 90% good/excellent) | Over 90% hip preservation at 10 years |
| Moderate damage (Beck 2) | Good (75-85% good/excellent) | 70-80% hip preservation at 10 years |
| Severe damage (Beck 3-4) | Fair (50-60% good/excellent) | 50-60% hip preservation at 10 years |
Prognostic Factors:
Favorable:
- Young age (less than 40 years)
- Minimal osteoarthritis (Tonnis 0-1)
- Preserved joint space (greater than 2mm)
- Labral repair (vs debridement)
- Positive injection response pre-operatively
Unfavorable:
- Advanced osteoarthritis
- Joint space less than 2mm
- Full-thickness cartilage loss
- Age greater than 50 years
- Significant acetabular dysplasia
Special Considerations
Borderline Dysplasia:
- Center-edge angle 20-25° is borderline
- May benefit from arthroscopy if FAI component present
- Higher failure rate than non-dysplastic hips
- Consider periacetabular osteotomy (PAO) if significant dysplasia
Revision Hip Arthroscopy:
- Success rates lower than primary (60-70%)
- Most common reasons for failure: inadequate cam resection, missed pincer, untreated labral tear
- Better outcomes if clear identifiable pathology for revision
Hip Arthroscopy in Adolescents:
- FAI morphology develops during skeletal maturation
- Arthroscopy may be considered in skeletally mature adolescents
- Must ensure physes are closed before aggressive osteochondroplasty
Labral Reconstruction:
- Indicated when labrum is deficient and cannot be repaired
- Options: iliotibial band autograft, tensor fascia lata, allograft
- Emerging technique with promising early results
Associated Hip Instability:
- Can result from excessive capsulotomy or rim trimming
- Capsular plication may be needed
- Important to balance impingement correction with stability preservation
Evidence Base
Hip Arthroscopy vs Best Conservative Care - UK FASHIoN RCT
- Pragmatic multicentre RCT, 348 patients with FAI syndrome at 23 UK NHS hospitals
- Hip arthroscopy versus personalised hip therapy (physiotherapist-led conservative care)
- Both groups improved; arthroscopy superior at 12 months
- Adjusted mean iHOT-33 difference 6.8 points (95% CI 1.7-12.0) favouring arthroscopy
- Difference exceeded the minimum clinically important difference (6.1 points)
Warwick Agreement on FAI Syndrome (International Consensus)
- International multidisciplinary consensus, 22 panellists from 9 countries, endorsed by 25 societies
- Introduced the term 'FAI syndrome' - requires symptoms PLUS signs PLUS imaging findings
- Imaging morphology alone (cam/pincer) is NOT a diagnosis without symptoms
- Accepted treatments: conservative care, rehabilitation, and arthroscopic or open surgery
Labral Refixation vs Debridement
- Comparative cohort, 94 hips with pincer/combined FAI, mean 3.5-year follow-up
- Good-to-excellent results in 92% of refixation versus 68% of debridement hips (p=0.004)
- Modified Harris Hip Score, SF-12 and VAS pain all significantly better after refixation
- Supports labral preservation to retain the suction-seal function
Alpha Angle and Cam Morphology
- Defined the alpha angle on oblique axial MRI to quantify head-neck concavity
- Mean alpha angle 74° in symptomatic impingement hips versus 42° in asymptomatic controls (p less than 0.001)
- Good inter-observer reproducibility across four observers
- Established the radiographic basis for diagnosing cam morphology
Outcomes Based on Pre-operative Joint Space
- Prospective series, 112 hips, minimum 2-year follow-up
- Modified Harris Hip Score improved from 58 to 84 (mean gain 24 points)
- Joint space narrowing of 2mm or more independently predicted a better outcome (p=0.005)
- Labral repair (versus debridement) also predicted a better outcome (p=0.032)
Complications After Hip Arthroscopy - Prospective Multicentre Series
- 1615 consecutive hips, 4 centres, validated complication grading scheme
- Overall complication rate 8.3% (excluding transient periportal numbness)
- Lateral femoral cutaneous nerve disturbance 16.5% (persisting beyond 6 months in only 1.6%)
- Pudendal (perineal) numbness 1.4%; traction time greater than 60 minutes raised complication risk
- Pudendal neurapraxia hips had longer traction (61.5 vs 43.8 minutes, p less than 0.001)
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Young Athlete with Groin Pain
"A 25-year-old male professional soccer player presents with 6 months of right groin pain that is worse with kicking and sprinting. He describes a deep anterior hip pain that is aggravated by prolonged sitting."
History: The presentation is classic for FAI in a young athlete. I would establish the exact location of pain (C-sign suggests intra-articular), onset and duration (insidious over 6 months suggests impingement rather than acute labral tear), aggravating factors (kicking involves hip flexion/internal rotation - classic impingement position), and mechanical symptoms (clicking suggests labral pathology). I would ask about prior injuries and treatments attempted.
Examination: I would assess gait, hip ROM (expect decreased internal rotation in flexion), and perform provocative tests. FADIR test (anterior impingement) is most sensitive - positive if reproduces groin pain with hip flexion, adduction, and internal rotation. FABER test assesses labrum and SI joint. Log roll test assesses intra-articular pathology. I would also examine the spine, SI joints, and perform a hernia check.
Investigations: AP pelvis and cross-table lateral radiographs to assess for cam (alpha angle greater than 55°) and pincer (CE angle greater than 40°) morphology. MR arthrogram is gold standard for labral evaluation. Diagnostic intra-articular injection can confirm intra-articular source of pain (greater than 50% relief predicts good surgical outcome).
Management: Initial non-operative trial (3-6 months) with activity modification, physiotherapy, and NSAIDs. If imaging confirms FAI and symptoms persist despite conservative management with positive injection response, hip arthroscopy is indicated. Surgical goals: osteochondroplasty for cam lesion, labral repair if torn, address any pincer component.
Portal Anatomy and Nerve Risk
"You are planning hip arthroscopy on a patient with confirmed FAI and labral tear. The examiner asks you to describe your portal placement and the nerves at risk."
Standard Portals: I use three standard portals for hip arthroscopy. The anterolateral portal is my primary viewing portal, placed 1cm anterior and superior to the greater trochanter tip. The anterior portal is my primary working portal, placed at the intersection of a horizontal line from the ASIS and a vertical line from the greater trochanter. The posterolateral portal is placed 1cm posterior and superior to the greater trochanter tip for supplementary viewing and working.
Nerves at Risk: The lateral femoral cutaneous nerve is at greatest risk with the anterior portal - it crosses approximately 1-2cm distal and medial to the ASIS. Injury causes meralgia paresthetica (lateral thigh numbness). Prevention involves staying more than 2cm from ASIS and using blunt dissection after skin incision.
Additional Nerve Considerations: The pudendal nerve is at risk from perineal post pressure during traction (perineal numbness in about 1.4% in large series). I keep traction force and time to a minimum and use a well-padded, wide post. The sciatic nerve is at risk with excessive traction force or posteriorly directed portals. The superior gluteal nerve exits above piriformis and is at risk with proximal portal placement - I stay below the level of the piriformis insertion.
Portal Technique: I establish portals under fluoroscopic guidance. First, I inject the joint with saline and air to create an air arthrogram. I use a spinal needle to confirm trajectory before making skin incisions. After skin incision, I use blunt trocar insertion to protect nerves.
Cam vs Pincer Morphology
"You are shown radiographs of a hip. The examiner asks you to differentiate between cam and pincer morphology and describe how you would measure the relevant angles."
Cam Morphology Assessment: Cam FAI is femoral-based pathology caused by an aspherical bump at the femoral head-neck junction, typically anterosuperior. The diagnostic measurement is the alpha angle, measured on an axial view (cross-table lateral or axial MRI). I draw a line along the femoral neck axis, then identify the point where the head-neck junction exceeds the radius of the femoral head. The alpha angle is measured between the neck axis and a line from the femoral head center to this point. Normal is less than 50°, cam morphology is greater than 55°.
Pincer Morphology Assessment: Pincer FAI is acetabular-based from overcoverage. For global overcoverage, I measure the center-edge (CE) angle on the AP pelvis - the angle between a vertical line through the femoral head center and a line to the lateral acetabular edge. Normal is 25-40°, pincer is greater than 40°. For focal retroversion, I look for the crossover sign where the anterior acetabular wall crosses the posterior wall before the lateral edge, creating a figure-8 pattern.
Mixed Morphology: Mixed FAI (both cam and pincer) is present in approximately 80% of cases. Both components must be identified and addressed surgically. This requires osteochondroplasty for the cam lesion and rim trimming with labral management for the pincer component.
Clinical Correlation: Cam morphology is more common in young athletic males and causes outside-in cartilage abrasion. Pincer morphology is more common in middle-aged females and causes labral crush injury with countrecoup posterior cartilage damage.
Traction Complications
"During hip arthroscopy, the anesthetist informs you that you have been operating for 2.5 hours with traction continuously applied. They ask about traction-related complications."
Immediate Concern: Prolonged continuous traction is the key concern. In large prospective series, traction time greater than 60 minutes significantly increases the overall complication rate, and hips with pudendal neurapraxia had longer mean traction times (about 61 vs 44 minutes). Pudendal (perineal) numbness occurs in roughly 1.4% and the lateral femoral cutaneous nerve is the most commonly affected nerve overall (16.5%). My priority is to minimise further traction.
Other Nerves at Risk: The sciatic nerve is also at risk with prolonged traction, particularly with higher traction forces. Additionally, the femoral nerve and lateral femoral cutaneous nerve can be affected by sustained traction.
Immediate Actions: If I have completed the central compartment work, I would release traction immediately and proceed with peripheral compartment work (cam resection) which does not require traction. If central compartment work is incomplete, I would release traction for at least 10 minutes before reapplying, and work as efficiently as possible to complete the case.
Prevention Strategies: For future cases, I monitor traction time closely and plan for intermittent release every 1.5-2 hours. I use a well-padded, wide perineal post and minimum necessary traction force. In very prolonged or complex cases, consider lateral positioning to eliminate the perineal post entirely. Pre-operative planning and surgical efficiency help minimize traction time.
Post-operative Management: I will examine the patient post-operatively for perineal numbness and document findings. If neurapraxia is present, I will counsel the patient that this typically resolves within 6 weeks but can take up to 6 months.
Poor Surgical Candidate
"A 55-year-old woman presents with hip pain and imaging shows FAI with a joint space of 1.5mm and Tonnis grade 2 osteoarthritis. She is keen for hip arthroscopy to avoid hip replacement."
Assessment of Candidacy: This patient has several factors that predict poor outcomes from hip arthroscopy. Her joint space of 1.5mm (less than 2mm threshold), Tonnis grade 2 osteoarthritis, and age of 55 are all unfavorable prognostic factors. Studies show that patients with joint space less than 2mm have a 50% conversion to THA within 2 years.
Counseling Discussion: I would explain that while I understand her desire to preserve her native hip, hip arthroscopy is unlikely to provide lasting benefit in her situation. The outcomes data show that patients with advanced arthritis and joint space narrowing have significantly higher failure rates and often require total hip replacement within a few years anyway.
Options Presented: I would present her options: (1) Continued non-operative management with activity modification, physiotherapy, NSAIDs, and potentially intra-articular injections - this may provide symptomatic relief but will not halt disease progression. (2) Total hip arthroplasty - this is the most predictable option for lasting pain relief and functional improvement in her situation. (3) Hip arthroscopy - I would explain this carries significant risk of failure and may not delay arthroplasty, but if she strongly prefers, we could discuss with understanding of realistic expectations.
Realistic Expectations: If she still wishes to pursue arthroscopy, I would ensure she understands that the procedure may provide temporary improvement but has approximately 50% chance of requiring THA within 2 years. She must accept this possibility before proceeding.
MCQ Practice Points
Clinical Pearl
Q: What are the radiographic definitions of Cam and Pincer FAI? A: Cam FAI is defined by an alpha angle greater than 55 degrees (femoral side). Pincer FAI is defined by a Center-Edge (CE) angle greater than 40 degrees or a crossover sign (acetabular side).
Clinical Pearl
Q: Which nerve is most commonly injured during hip arthroscopy? A: The Lateral Femoral Cutaneous Nerve (LFCN) is the most commonly affected nerve overall (16.5% transient disturbance in large series, persisting beyond 6 months in only 1.6%), typically from the anterior/anterolateral portal. The Pudendal nerve (perineal numbness, about 1.4%) is the classic traction-related injury and is the high-yield answer for "traction complication".
Clinical Pearl
Q: What are the traction safety limits? A: Traction should be limited to less than 2 hours duration and minimum necessary force (typically 25-50lbs) to reduce neurapraxia risk.
Clinical Pearl
Q: What joint space width predicts poor outcomes? A: Joint space less than 2mm is a strong predictor of failure and conversion to Total Hip Arthroplasty (50% within 2 years).
Clinical Pearl
Q: What is the most sensitive physical exam test for FAI? A: The FADIR test (Flexion, Adduction, Internal Rotation). It is highly sensitive (95%) but has low specificity.
Guidelines, Registries & Global Practice
Global epidemiology. FAI morphology is common and frequently asymptomatic, so imaging must always be correlated with symptoms and signs. A PRISMA systematic review of 2114 asymptomatic hips (mean age 25 years) found asymptomatic cam morphology in 37% overall - 54.8% in athletes versus 23.1% in the general population - and the mean alpha angle in asymptomatic hips was 54° (Frank 2015). This is the single most important framing fact: morphology alone is not disease.
The diagnosis is a triad, not a radiograph. The 2016 Warwick Agreement (international consensus, 25 endorsing societies) introduced the term FAI syndrome, requiring symptoms + clinical signs + imaging findings together. Imaging morphology without symptoms is not FAI syndrome and should not be treated (Warwick 2016).
Guidance side by side
Major Guidance / Consensus on FAI Syndrome
| Body (region) | Core position | Basis / evidence level |
|---|---|---|
| Warwick Agreement (international consensus) | FAI syndrome = symptoms + signs + imaging; first-line either conservative care or surgery after shared decision-making | Consensus statement (Level V) |
| NICE (UK) | Open and arthroscopic FAI surgery may be used with standard arrangements for governance, consent and audit; recognises evidence is still maturing | Interventional procedures guidance |
| BJSM / FASHIoN trial evidence (UK) | Arthroscopy gives a clinically meaningful but modest benefit over structured physiotherapy at 12 months (iHOT-33 +6.8) | Level I RCT |
| ISHA / hip-preservation societies | Endorse arthroscopic management for appropriately selected FAI syndrome with preserved joint space and minimal arthritis | Society endorsement / expert consensus |
Patient selection drives outcome (global, evidence-led). Across health systems the same predictors apply: preserved joint space (2mm or more) and labral repair predict better results, while advanced arthritis (Tönnis 2 or more) and joint space less than 2mm predict failure and conversion to total hip replacement (Philippon 2009). The decisive modifiable intra-operative safety factor is traction - time greater than 60 minutes raises the complication rate (Larson 2016).
Registries and practice variation. Hip arthroscopy is a hip-preservation rather than an arthroplasty procedure, so it is not captured by the major joint replacement registries (NJR England & Wales, AOANJRR Australia, AJRR USA, SHAR Sweden). These registries are nonetheless relevant downstream: a meaningful minority of arthroscopy patients with pre-existing chondral wear later convert to total hip arthroplasty, and registry analyses are used to compare outcomes of THA after prior hip arthroscopy. Volume and access vary widely - arthroscopy is concentrated in high-resource centres with fluoroscopy and traction tables and a learning curve effect on complications, whereas in many regions open surgical hip dislocation or non-operative care predominate. FAI syndrome is recognised worldwide in flexion-loading sports (football/soccer, ice hockey, Australian Rules football, dance, martial arts), reflecting the higher cam prevalence seen in athletes.
HIP ARTHROSCOPY
Clinical summary
FAI Classification
- •Cam = femoral bump, alpha greater than 55°, young males
- •Pincer = acetabular overcoverage, CE greater than 40°, middle-aged females
- •Mixed = most common (80%), address both components
- •Crossover sign = focal acetabular retroversion
Traction Safety
- •Maximum 2 hours traction time
- •25-50lbs force typically needed
- •Minimum 6mm joint distraction
- •Break seal with IR before distraction
Nerves at Risk
- •LFCN: most common nerve injury (16.5% transient); pudendal ~1.4%
- •Lateral femoral cutaneous: anterolateral portal (meralgia)
- •Sciatic: excessive traction, posterior portals
- •Superior gluteal: proximal portal placement
Portal Placement
- •Anterolateral: 1cm anterior/superior to GT tip (viewing)
- •Anterior: ASIS horizontal meets GT vertical (working)
- •Posterolateral: 1cm posterior/superior to GT
- •Always establish under fluoroscopic guidance
Key Numbers
- •Alpha angle: greater than 55° = cam
- •CE angle: greater than 40° = pincer
- •Joint space: less than 2mm = poor outcome
- •2 hours max traction, 25lbs min force, 6mm distraction
Exam Pearls
- •FADIR test most sensitive for FAI
- •Joint space greater than 2mm critical for good outcomes
- •Labral repair preferred over debridement
- •Pudendal nerve most commonly injured