90% Posterior | Reduce within 6 Hours | Sciatic Nerve at Risk
DIRECTION OF DISLOCATION
Critical Must-Knows
- Posterior dislocation is most common (90%) - mechanism is dashboard injury (knee hitting dashboard = flexed hip)
- Sciatic nerve at risk in posterior dislocation (10-20%) - peroneal division most vulnerable
- 6-hour golden window - AVN risk increases significantly if reduction delayed beyond 6 hours
- Associated fractures common - femoral head (Pipkin), acetabulum (posterior wall), femoral neck
- CT post-reduction mandatory to assess concentric reduction and associated fractures
Clinical Pearls
- "Posterior: leg shortened, adducted, internally rotated. Anterior: externally rotated, abducted
- "Sciatic nerve palsy: most recover by 2 years, explore if no recovery by 6 months
- "Pipkin I and II = different - Pipkin I below fovea (ORIF), Pipkin II above fovea (excise if small)
- "Thompson-Epstein classification for posterior; Epstein classification for anterior
Clinical Imaging
Imaging Gallery




Critical Hip Dislocation Exam Points
Time is Critical
6-hour golden window for reduction. AVN risk increases from 5% (under 6h) to 40%+ (over 12h). This is a true orthopaedic emergency. Reduce as soon as possible.
Sciatic Nerve
10-20% sciatic nerve injury in posterior dislocation. Peroneal division most vulnerable. Document nerve function BEFORE and AFTER reduction. Most recover by 2 years.
Associated Injuries
High-energy mechanism - look for associated injuries: femoral head fracture (Pipkin), acetabular fracture (posterior wall), femoral neck fracture (15%), knee injuries (PCL, patella).
Post-Reduction CT
CT mandatory after reduction. Assess for: concentric reduction, incarcerated fragments, femoral head impaction, acetabular fracture, femoral neck fracture.
Quick Decision Guide
| Injury Pattern | Key Finding | Treatment | Pearl |
|---|---|---|---|
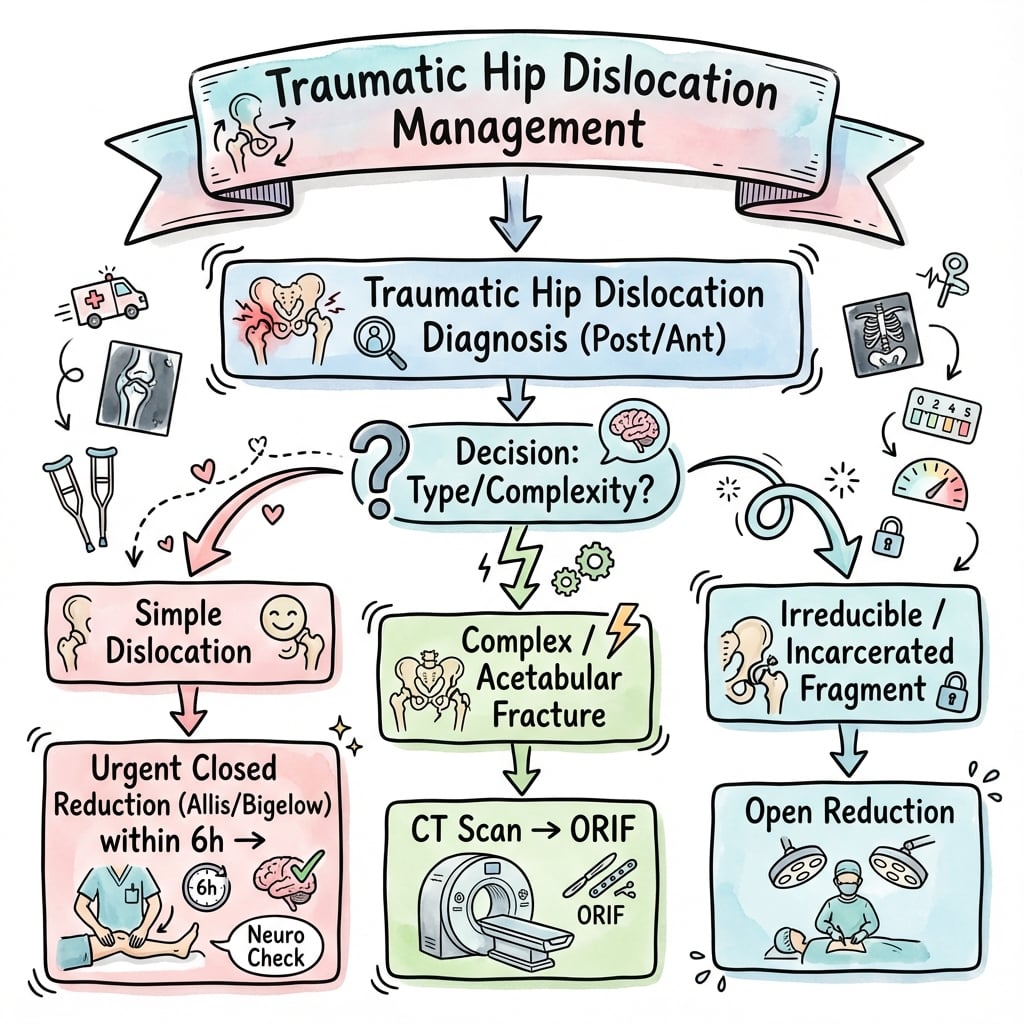
| Simple posterior dislocation | No fracture on X-ray | Urgent closed reduction, CT after | 6-hour window - treat as emergency |
| Posterior + posterior wall fracture | Posterior wall on CT | Reduce, CT assess wall size, ORIF wall | Wall over 40% = unstable, needs fixation |
| Posterior + Pipkin fracture | Femoral head fragment | Reduce, Pipkin classification guides Rx | Pipkin I (below fovea) = consider ORIF |
| Dislocation + femoral neck fracture | Femoral neck visible | Cannot reduce closed - open reduction | Devastating injury - high AVN risk |
| Anterior dislocation | Leg externally rotated, abducted | Closed reduction | Less common (10%), check femoral vessels |
SAIDPosterior Hip Dislocation Position
| S | Shortened Leg appears shorter |
| A | Adducted Leg pulled toward midline |
| I | Internally rotated Foot points inward |
| D | Dashboard injury Mechanism - knee hits dashboard |
| S | Shortened Leg appears shorter | I | Internally rotated Foot points inward |
| A | Adducted Leg pulled toward midline | D | Dashboard injury Mechanism - knee hits dashboard |
Hook:The patient SAID 'my knee hit the dashboard' - leg is Short, Adducted, Internally rotated, from Dashboard injury!
FABERAnterior Hip Dislocation Position
| F | Flexed Hip may be slightly flexed |
| A | Abducted Leg falls away from midline |
| B | Bulge anteriorly Head palpable in groin |
| E | Externally rotated Foot points outward |
| R | Rare (10%) Much less common than posterior |
| F | Flexed Hip may be slightly flexed | E | Externally rotated Foot points outward |
| A | Abducted Leg falls away from midline | R | Rare (10%) Much less common than posterior |
| B | Bulge anteriorly Head palpable in groin |
Hook:Anterior dislocation puts the hip in forced FABER position!
6 AVN6-Hour Rule Importance
| 6 | 6 hours Golden window for reduction |
| A | AVN risk Avascular necrosis increases |
| V | Very urgent True orthopaedic emergency |
| N | No delay Every hour counts |
| 6 | 6 hours Golden window for reduction | V | Very urgent True orthopaedic emergency |
| A | AVN risk Avascular necrosis increases | N | No delay Every hour counts |
Hook:After 6 hours, AVN risk climbs - '6 AVN' reminds you time is hip!
PERONEAL PRONESciatic Nerve in Posterior Dislocation
| P | Peroneal Division most at risk |
| E | Examine Before and after reduction |
| R | Recovery expected 90% recover by 2 years |
| O | Observe initially Most are neuropraxia |
| N | No recovery at 6 months Consider exploration |
| E | EMG/NCS If not recovering at 3 months |
| A | Always document Medicolegal requirement |
| L | Lateral nerve vulnerable Peroneal = lateral |
| P | Peroneal Division most at risk | O | Observe initially Most are neuropraxia | A | Always document Medicolegal requirement |
| E | Examine Before and after reduction | N | No recovery at 6 months Consider exploration | L | Lateral nerve vulnerable Peroneal = lateral |
| R | Recovery expected 90% recover by 2 years | E | EMG/NCS If not recovering at 3 months |
Hook:Peroneal is prone to injury when the hip goes posterior!
Overview and Epidemiology
Why This Topic Matters
Hip dislocation is a true orthopaedic emergency with time-sensitive management. The examiner will test your understanding of the 6-hour rule, sciatic nerve considerations, and associated injuries. Getting the basics wrong shows poor emergency management understanding.
Demographics
- Young adults (MVA, high-energy trauma)
- Native hips - dislocation rare in healthy hip
- Male predominance (2:1) - high-risk activities
- Prosthetic hips - much more common (different topic)
Mechanism
- MVA most common (dashboard injury)
- High-energy sports (AFL, rugby)
- Industrial accidents
- Fall from height
- Force vector determines direction
Anatomy and Mechanism
Key Anatomical Concept
The hip is inherently stable - a ball-and-socket joint requiring significant force to dislocate. Stability comes from: bony congruity, acetabular labrum, strong capsular ligaments (iliofemoral, pubofemoral, ischiofemoral), and surrounding muscles.
Femoral Head Blood Supply
| Artery | Source | Contribution | Clinical Relevance |
|---|---|---|---|
| MFCA - Retinacular vessels | Profunda femoris | 80-90% of head | Damaged in dislocation - AVN risk |
| LFCA | Profunda femoris | Minimal | Minor contribution |
| Ligamentum teres artery | Obturator artery | 10-20% (variable) | More important in children |
| Intraosseous from neck | Metaphyseal | Variable | May be compromised |
AVN Mechanism
Dislocation stretches/tears the retinacular vessels (from MFCA) that supply the femoral head. Prolonged dislocation = prolonged ischemia. AVN risk doubles after 6 hours and approaches 50% after 12-24 hours.
Classification Systems
Thompson-Epstein Classification (Posterior)
| Type | Description | Treatment |
|---|---|---|
| Type I | Simple dislocation, no/minimal fracture | Closed reduction, conservative |
| Type II | Posterior wall rim fracture (small) | Closed reduction, assess stability |
| Type III | Large posterior wall fracture (unstable) | ORIF posterior wall |
| Type IV | With acetabular floor fracture | ORIF acetabulum |
| Type V | With femoral head fracture (Pipkin) | Pipkin classification guides treatment |
Practical Simplification
In practice, think: Simple dislocation (reduce urgently) vs Complex (with fracture - reduce, then definitive fix). CT post-reduction determines if wall/head fixation needed.
Clinical Assessment
History
- Mechanism: MVA, dashboard, sport - force vector matters
- Time of injury: 6-hour rule critical
- Associated injuries: polytrauma? knee injury?
- Medical history: native vs prosthetic hip
- Anticoagulation: bleeding risk assessment
Examination
- ATLS first in polytrauma
- Obvious deformity - position diagnostic
- Leg length discrepancy
- Neurovascular status: sciatic (peroneal), femoral
- Knee examination: PCL, patella (dashboard)
- Log roll: pelvic stability
Posterior vs Anterior Clinical Signs
| Finding | Posterior | Anterior |
|---|---|---|
| Leg position | Shortened, adducted, IR (SAID) | Abducted, externally rotated |
| Knee position | Flexed | May be extended |
| Head palpable | Not anteriorly (empty) | Palpable in groin (bulge) |
| Nerve at risk | Sciatic (peroneal) | Femoral, lateral cutaneous |
| Frequency | 90% | 10% |
Polytrauma Assessment
ATLS takes priority. Hip dislocation often occurs in polytrauma setting. Complete primary and secondary survey. Missed ipsilateral femoral neck fracture is a disaster - do not attempt closed reduction if neck fracture suspected.
Differential Diagnosis of the Acutely Painful, Deformed Hip After Trauma
| Diagnosis | Discriminating Features | Key Imaging | Why It Matters |
|---|---|---|---|
| Posterior hip dislocation | Shortened, adducted, internally rotated (SAID); empty acetabulum | AP pelvis: head superolateral, smaller apparent head | Time-critical reduction to limit AVN |
| Anterior hip dislocation | Abducted, externally rotated; head palpable in groin | AP pelvis: head infero/anteromedial, larger apparent head | Different reduction vector; femoral vessel proximity |
| Femoral neck fracture | Shortened, externally rotated; unable to straight-leg raise | AP/lateral hip; CT if occult | Closed reduction of a coexisting dislocation can displace/comminute the neck - catastrophic |
| Intertrochanteric fracture | Shortened, externally rotated; elderly low-energy | AP hip/pelvis radiograph | No dislocation; different fixation pathway |
| Acetabular fracture without frank dislocation | Pain, reduced weight-bearing; head may be central/subluxed | Judet views + CT | May be central fracture-dislocation; staged reconstruction |
| Native vs prosthetic hip dislocation | Surgical scar, known arthroplasty, low-energy mechanism | Radiograph shows implant | Prosthetic instability has a separate work-up and reduction risk profile |
The Trap You Must Not Miss
The single most dangerous differential is a coexisting ipsilateral femoral neck fracture. If the neck is fractured, closed reduction of the dislocation can convert a salvageable injury into a displaced neck fracture with devastating AVN risk. Scrutinise the neck on the pre-reduction film, and if there is any doubt obtain CT or proceed to open reduction.
Investigations
Imaging Protocol
Diagnosis usually obvious. Look for associated fractures: posterior wall, femoral head (shenton's arc), femoral neck. Do not delay reduction for extensive imaging.
Judet views if stable. Do not delay reduction - X-ray after if unstable patient.
Assess: concentric reduction, incarcerated fragments, femoral head impaction, posterior wall size, occult femoral neck fracture. This dictates further treatment.
Suspected labral pathology, soft tissue incarceration, early AVN assessment. Not urgent.
X-ray Signs of Hip Dislocation
Posterior Dislocation
- Head superolateral to acetabulum
- Smaller apparent head size (further from plate)
- Shenton's line disrupted
- Look for posterior wall fragment
- Internal rotation of lesser trochanter
Anterior Dislocation
- Head inferomedial (obturator) or anteromedial (pubic)
- Larger apparent head size (closer to plate)
- Shenton's line disrupted
- External rotation - lesser trochanter prominent
- Head may overlap obturator foramen

Management Algorithm
6-Hour Rule
Reduce within 6 hours! Every hour of dislocation increases AVN risk. Under 6h = 5% AVN. 6-12h = 15-20% AVN. Over 12h = 30-50% AVN. This is non-negotiable - prioritize reduction.
Closed Reduction Technique - Comprehensive Guide
Pre-Procedure Preparation
Documentation
- Time of injury - 6-hour rule critical
- Sciatic nerve exam - document BEFORE reduction
- Peroneal: dorsiflexion, toe extension, dorsal foot sensation
- Tibial: plantarflexion, plantar sensation
- Informed consent - AVN, nerve injury, need for open procedure
Setup
- General anaesthesia or deep sedation - muscle relaxation essential
- Theatre or ED resuscitation bay (if stable)
- Fluoroscopy available - confirm reduction
- Assistant to stabilize pelvis - this is crucial
- Padded table - patient supine
- Backup plan for open reduction if needed
Allis Maneuver (Preferred Technique)
Step-by-Step Allis Maneuver
Supine on firm table. Assistant positioned at patient's pelvis with hands pressing down on ASIS bilaterally. This counterforce is essential - without it, you'll pull the whole patient toward you.
Stand at the side of the table, facing the patient's head. Flex the hip to 90° and knee to 90°. This relaxes the iliofemoral ligament (strongest ligament in body) and positions the head at the acetabular opening.
Grasp the proximal tibia/knee region. Apply steady, in-line axial traction pulling the femur toward the ceiling (with hip at 90°). This is NOT a jerking motion - steady sustained force.
- Some surgeons place knee in crook of elbow for leverage
- Full body weight can be used - stand on table if needed
While maintaining traction, apply gentle internal and external rotation to the leg. This helps disengage the femoral head from behind the acetabulum and guides it over the rim.
- Listen/feel for a satisfying clunk of reduction
- Do NOT use excessive force or rotation
Once reduced, leg should return to normal length and alignment. Test ROM carefully - hip should move through flexion, extension, rotation smoothly. Obtain fluoroscopy or X-ray immediately.
Technique Pearl - Leverage
For strong patients or difficult reductions, stand on the table for better leverage. Place the patient's knee in the crook of your elbow, hold the tibia, and use your body weight to provide steady axial traction. This is the "Captain Morgan" technique variation.
Alternative: Stimson Maneuver
Stimson Technique
- Patient prone on table with injured leg hanging off
- Hip flexed over edge of table (90°)
- Knee flexed to 90°
- Gravity provides traction on the hanging limb
- Assistant stabilizes pelvis
- Surgeon applies downward pressure on calf with gentle rotation
- Useful when Allis fails, but requires rolling patient prone
Advantages/Disadvantages
Advantages:
- Gravity provides continuous traction
- Less physical effort for surgeon
- Muscle relaxation with gravity
Disadvantages:
- Requires rolling polytrauma patient prone
- Cannot visualize patient face (airway)
- Not suitable for unstable patients
Critical Technical Points
Do's
- Document sciatic nerve function before AND after
- Ensure adequate sedation/relaxation - fighting muscles = failure
- Use steady sustained traction - not jerky movements
- Have assistant stabilize pelvis firmly
- Confirm reduction with imaging immediately
- Get CT post-reduction - mandatory
Don'ts
- Don't use excessive force - risk of iatrogenic fracture
- Don't attempt more than 2-3 times - go to open if failing
- Don't reduce if femoral neck fracture suspected - catastrophic
- Don't forget post-reduction CT - miss fragments or wall
- Don't delay for imaging - time is hip, reduce first
- Don't wait for specialist if unavailable - reduce within 6h
Troubleshooting Failed Reduction
| Problem | Likely Cause | Solution |
|---|---|---|
| Can't reduce despite good traction | Incarcerated fragment (labrum, osteochondral) | Proceed to open reduction - cannot force closed |
| Reduces but immediately redislocates | Posterior wall fracture (unstable) | Maintain reduction with traction, CT, plan ORIF wall |
| Patient fighting reduction attempts | Inadequate muscle relaxation | Increase sedation/paralysis, ensure full GA |
| Reduction attempted but limb still short/IR | Not actually reduced, head still out | Obtain fluoro immediately, reattempt or open |
| Clunk felt but CT shows non-concentric | Incarcerated soft tissue or fragment | Urgent operative removal of incarcerated tissue |
When to Abandon Closed Reduction
Stop closed reduction if: (1) X-ray shows femoral neck fracture - closed forces will displace it, (2) More than 2-3 gentle attempts fail - something is blocking reduction, (3) Patient becomes hemodynamically unstable. Proceed to open reduction urgently - still need to meet 6-hour window.

Surgical Technique
Closed Reduction Technique
Preparation:
- Adequate anesthesia and muscle relaxation (GA preferred)
- Fluoroscopy available
- Assistant required for counter-traction
Posterior Dislocation (Allis/Bigelow):
- Patient supine, assistant stabilizes pelvis
- Hip flexed to 90 degrees, knee flexed
- Inline traction along femoral axis
- Gentle internal rotation while maintaining traction
- Feel for "clunk" as head relocates
- Assess stability through range of motion
Anterior Dislocation:
- External rotation, extension, and traction
- Less common, often require open reduction
Post-Reduction Assessment:
- Fluoroscopy to confirm concentric reduction
- Full ROM under fluoro to assess stability
- CT scan to exclude loose fragments or fracture
Emergency reduction within 6 hours is critical to minimize AVN risk.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| AVN | 10-40% | Delayed reduction over 6h, repeated attempts | Surveillance, THA if symptomatic |
| Sciatic nerve injury | 10-20% | Posterior dislocation, bone fragments | Observe, most recover by 2 years |
| Post-traumatic OA | 20-40% | Cartilage damage, malreduction, AVN | Activity modification, THA long-term |
| Recurrent dislocation | Rare in native hip | Posterior wall deficiency, malreduction | Revision ORIF or THA |
| Heterotopic ossification | 3-5% | Delayed surgery, brain injury | Prophylaxis: indomethacin or RT |
| Femoral head collapse | Variable | AVN, untreated Pipkin | THA |
Avascular Necrosis
AVN Timeline
AVN may take 6-24 months to become apparent on X-ray. MRI can detect earlier (marrow changes). Follow with X-rays at 6 weeks, 3 months, 6 months, 1 year, 2 years. Treat symptomatic AVN with THA.
Postoperative Care and Rehabilitation
Rehabilitation Protocol
Toe-touch or protected weight bearing depending on stability. Bed rest initially. Thromboprophylaxis. ROM exercises.
If stable and no fracture: progress to full weight bearing. If ORIF: protected until fracture healing assessed on X-ray.
Full weight bearing. Progressive strengthening. Gait training. Hip abductor focus.
Return to sport/activity once strength restored. Long-term surveillance for AVN (X-rays).
Weight Bearing Decisions
Simple dislocation (no fracture, concentric reduction): May weight bear as tolerated early. With posterior wall ORIF: Protected until wall healed (6-12 weeks). Pipkin ORIF: Depends on fragment size and fixation.
Outcomes and Prognosis
Prognostic Factors
Outcomes by Pattern
| Pattern | Good Outcome Rate | Key Factors | Complications |
|---|---|---|---|
| Simple posterior dislocation | 70-80% | Early reduction, no fracture | AVN 5-10%, OA 15-20% |
| Posterior + wall fracture | 50-70% | Quality of reduction, wall stability | AVN 10-20%, OA 20-40% |
| Pipkin I | 60-70% | Fragment size, excision vs ORIF | AVN 10-20% |
| Pipkin II | 40-60% | Articular involvement, reduction quality | AVN 20-30%, OA 30-50% |
| Pipkin III | 20-40% | Age, dual blood supply injury | AVN 40-60%, often THA |
Factors Affecting Outcome
Favorable Factors
Reduction within 6 hours, Simple dislocation without fracture, Concentric stable reduction achieved, Young patient without comorbidities, No sciatic nerve injury
Unfavorable Factors
Delayed reduction over 6-12 hours, Associated acetabular or femoral head fracture, Non-concentric or unstable reduction, Sciatic nerve injury (peroneal component), Repeated closed reduction attempts
Long-term Outcomes
Most patients with simple posterior dislocations reduced within 6 hours have good functional outcomes. The main determinants of long-term outcome are development of AVN and post-traumatic osteoarthritis. Younger patients may tolerate mild degenerative change better than older patients. THA remains the salvage procedure for severe AVN or debilitating arthritis.
Evidence Base and Key Trials
Timing and AVN - Hougaard & Thomsen (origin of the time-to-reduction principle)
- 98 adults with 100 traumatic posterior dislocations, minimum 5-year follow-up
- Avascular necrosis in only 4.8% of hips reduced within 6 hours
- Avascular necrosis in 52.9% of hips reduced more than 6 hours after injury
- Higher AVN incidence with Stewart-Milford grade III and IV dislocations; no benefit demonstrated from skeletal traction or non-weight-bearing
AVN & Post-Traumatic OA Meta-Analysis - Kellam & Ostrum
- Systematic review and meta-analysis of AVN and post-traumatic arthritis after traumatic hip dislocation
- Posterior dislocation AVN event rate 10.6-43.0%; PTA event rate 19.4-58.6%
- Odds ratio of AVN 5.6 for reduction after 12 hours versus before 12 hours
- Injury severity (higher Thompson-Epstein grade) correlates with more AVN and PTA
Posterior Wall Stability on CT - Moed
- Walls involving less than 20% are generally stable; greater than 40-50% are generally unstable, leaving an indeterminate middle zone
- Static 2D CT measurement was an unreliable predictor of instability for fragments around 20-40%
- Dynamic fluoroscopic stress examination under general anaesthesia is the recommended gold-standard test of stability
- Small CT wall size does not reliably exclude instability
Non-Operative Posterior Wall after Stable EUA - Grimshaw & Moed
- 21 posterior wall fractures shown to be stable on dynamic stress fluoroscopy under anaesthesia, treated non-operatively
- At minimum 2-year follow-up, modified Merle d'Aubigne scores were good to very good in all
- All radiographically assessed hips had a congruent joint with no post-traumatic arthritis
- Stable EUA reliably predicts a congruent joint and good early outcome without surgery
Femoral Head (Pipkin) Fracture Outcomes & Approach - Stannard
- 26 femoral head fractures associated with hip dislocation - often poor functional outcome
- Kocher-Langenbeck posterior approach carried a 3.2x higher odds of AVN versus the Smith-Petersen anterior approach
- Brumback classification differentiated fracture types better than Pipkin in this series
- 3-mm cannulated screws with washers gave poor results and are contraindicated for head fixation
Vascular-Safe Surgical Dislocation - Ganz Technique
- Trochanteric flip osteotomy with anterior dislocation through a posterior approach, based on detailed MFCA anatomy
- External rotators are not divided and the obturator externus protects the medial femoral circumflex artery
- 213 hips over 7 years with intra-operative confirmation of head perfusion - no subsequent AVN reported in the series
- Gives full access to the femoral head and acetabulum for fixation of head fractures and loose bodies
HO Prophylaxis Caution - Indomethacin & Long-Bone Nonunion (Burd RCT)
- Patients with acetabular fractures randomised to indomethacin or radiation for HO prophylaxis
- Among 112 with a concomitant long-bone fracture, nonunion occurred in 26% of the indomethacin group versus 7% without indomethacin (p=0.004)
- Radiation therapy did not carry the same nonunion penalty
- Companion RCT (Moore 1998, JBJS Br, PMID 9546456) showed indomethacin and single-dose ~800 cGy radiation were equally effective at preventing HO
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Simple Posterior Hip Dislocation
"A 25-year-old male is brought to ED after an MVA. He was an unrestrained front passenger. His left leg is shortened, adducted, and internally rotated. He has no other obvious injuries and is haemodynamically stable. X-ray shows a posterior hip dislocation with no obvious fracture. It is 2 hours since the accident. How would you manage this patient?"
Scenario 2: Hip Dislocation with Posterior Wall Fracture
"A 30-year-old female presents after a motorcycle accident with a posterior hip dislocation. You perform closed reduction successfully at 4 hours post-injury. Post-reduction CT shows concentric reduction but a displaced posterior wall fragment involving approximately 50% of the articular surface. She has normal sciatic nerve function. What is your further management?"
Scenario 3: Pipkin Fracture
"A 35-year-old presents after an MVA with a posterior hip dislocation. You reduce the hip successfully at 5 hours. CT post-reduction shows a femoral head fragment (Pipkin type II - above the fovea involving 30% of the weight-bearing surface). The acetabulum appears intact. There is no sciatic nerve injury. How would you manage this?"
MCQ Practice Points
Timing Question
Q: What is the approximate AVN rate if a posterior hip dislocation is reduced after 12 hours? A: 40-50%. The 6-hour rule: under 6h = 5% AVN, 6-12h = 20%, over 12h = 40%+. Time to reduction is the most important modifiable factor.
Nerve Question
Q: Which division of the sciatic nerve is most commonly injured in posterior hip dislocation? A: Peroneal (common peroneal) division. It is more lateral and tethered, making it more vulnerable. Clinically presents as foot drop and dorsal foot numbness.
Clinical Question
Q: What is the classic leg position in posterior hip dislocation? A: Shortened, Adducted, Internally Rotated (SAID). The leg appears shorter, is pulled toward midline, with the foot pointing inward. This is the dashboard injury position.
Wall Question
Q: At what percentage of posterior wall involvement does the hip become unstable post-reduction? A: Over 40% posterior wall involvement. This threshold indicates the need for ORIF to prevent redislocation. Assess on CT post-reduction.
Classification Question
Q: What distinguishes Pipkin I from Pipkin II femoral head fractures? A: Pipkin I = below the fovea (infrafoveal), spares weight-bearing surface. Pipkin II = above the fovea (suprafoveal), involves weight-bearing surface and has worse prognosis.
Imaging Question
Q: What mandatory imaging is required after closed reduction of a hip dislocation? A: CT scan. Essential to assess: concentric reduction (no incarcerated fragments), posterior wall integrity, femoral head fracture, occult femoral neck fracture, and loose bodies.
Guidelines, Registries & Global Practice
Global Epidemiology
- Traumatic native-hip dislocation is uncommon and high-energy worldwide; the great majority (~85-90%) are posterior
- Dominant mechanism globally is road traffic collision (dashboard/front-seat passenger); motorcycle and pedestrian trauma predominate in low- and middle-income settings
- Sport (rugby codes, American football, skiing, soccer) is a recognised cause in young athletes
- In children, posterior dislocation predominates and AVN remains the key long-term adverse event (posterior ~86%, AVN ~15% of associated pathologies in a paediatric systematic review, Baumann 2023, PMID 37947036)
- Most fragility-type hip "dislocations" in the elderly are in fact prosthetic instability - a separate clinical entity
Practice Variation
- Where reduction happens varies: many systems reduce in the emergency department under procedural sedation; others mandate theatre/GA - both are defensible if muscle relaxation is adequate
- Time-to-reduction targets differ but the universal principle is "as soon as safely possible"; the historical 6-hour figure is a teaching anchor, not a regulatory threshold
- Stability assessment of intermediate posterior wall fractures varies between CT-only and examination under anaesthesia (EUA), with trauma units increasingly favouring EUA (Moed, PMID 19104298)
- Approach for femoral head fractures varies between anterior (Smith-Petersen), surgical hip dislocation (Ganz) and posterior (Kocher-Langenbeck), with a trend toward vascular-protective approaches
What Major Bodies Say (Principles - no single dedicated guideline exists)
| Source / Body | Position on Hip Dislocation | Evidence Basis |
|---|---|---|
| AAOS / OTA (North America) | Emergent reduction of the dislocated hip; mandatory post-reduction CT; EUA or CT to decide posterior wall stability; ORIF for unstable walls | Expert consensus + retrospective series (Moed, Grimshaw) |
| BOA / BOAST (UK) | Polytrauma hips managed in the ATLS framework within trauma networks; urgent reduction and senior-led decision-making; combined ortho-plastic and pelvic/acetabular referral pathways for associated fractures | BOAST standards for pelvic/acetabular and open fractures (principle-level) |
| AO Foundation / AO Trauma | Reduction priority, careful classification (Thompson-Epstein, Pipkin/Brumback), MFCA-protective approaches, anatomic articular reconstruction of wall/head fractures | AO surgical principles and technique teaching |
| EFORT (Europe) | Reinforces prompt reduction, mandatory cross-sectional imaging, and referral of complex fracture-dislocations to specialist acetabular units | European educational consensus |
No Dedicated RCT-Based Guideline
There is no high-level (NICE-style) clinical guideline specific to traumatic native hip dislocation because the injury is rare and randomised data are lacking. Practice rests on retrospective cohorts and meta-analysis (Hougaard 1986, Kellam & Ostrum 2016) plus expert consensus. In a viva, state this honestly: management is principle-driven (rapid reduction, mandatory post-reduction CT, stability-guided fixation), not protocol-driven.
Registry Evidence
- There is no dedicated traumatic-dislocation registry; long-term salvage data come from arthroplasty registries
- The AOANJRR (Australia), NJR (England & Wales), and Nordic registries capture THA performed for post-traumatic osteoarthritis and post-dislocation AVN, which is the common end-point of failed hips
- Post-traumatic / AVN indications are a recognised subgroup with their own revision profile, informing counselling about the possibility of eventual hip replacement
Australian Context
- MVA remains the main cause despite seatbelt and speed legislation, with a relative excess from high-speed rural crashes and remoteness affecting time-to-reduction
- AFL and NRL contribute occasional sporting dislocations in young athletes
- Trauma network designation and retrieval logistics (large distances) directly affect how quickly a rural patient reaches a unit able to reduce and image the hip
- The AOANJRR is the relevant registry for the arthroplasty end-point in post-traumatic AVN/OA
Medicolegal Considerations
Key documentation: (1) Time of injury AND time of reduction - the 6-hour rule, (2) Sciatic nerve exam before AND after reduction, (3) Consent including AVN and nerve risks, (4) Post-reduction CT performed and reviewed, (5) Follow-up plan for AVN surveillance. Delayed reduction and missed sciatic nerve injury are litigation risks.
HIP DISLOCATIONS
Clinical summary
Key Facts
- •Posterior 90%, Anterior 10%
- •6-hour rule: reduce early to minimize AVN
- •SAID position: Shortened, Adducted, IR (posterior)
- •Dashboard injury = posterior dislocation
Sciatic Nerve
- •10-20% injury rate in posterior dislocation
- •Peroneal division most vulnerable
- •Document BEFORE and AFTER reduction
- •90% recover by 2 years, explore at 6 months if not
Thompson-Epstein
- •Type I-II: Simple or small wall fragment
- •Type III: Large posterior wall (over 40%) - ORIF
- •Type IV: Acetabular floor fracture
- •Type V: Femoral head fracture (Pipkin)
Pipkin Classification
- •Pipkin I: Below fovea - better prognosis
- •Pipkin II: Above fovea - weight-bearing involved
- •Pipkin III: With femoral neck - disaster
- •Pipkin IV: With acetabular fracture
Post-Reduction CT
- •MANDATORY after every reduction
- •Check: concentric reduction, wall, fragments
- •Non-concentric = incarcerated tissue/bone
- •Over 40% wall = needs ORIF
AVN Rates
- •Under 6 hours: 5% AVN
- •6-12 hours: 20% AVN
- •Over 12 hours: 40%+ AVN
- •Surveillance X-rays for 2 years