Developmental Acetabular Deficiency | Progressive Arthritis | Joint-Preserving vs Arthroplasty
- Lateral CEA less than 25° = acetabular dysplasia (Wiberg angle)
- Periacetabular osteotomy (PAO) = gold standard joint preservation in young adults
- True acetabulum must be identified in Crowe III-IV for component placement
- Femoral shortening required in Crowe II-IV to avoid nerve stretch injury
- High hip center increases revision risk - restore anatomy when possible
- “DDH is the leading cause of hip arthritis in young women
- “Tönnis angle greater than 10° indicates lateral acetabular deficiency
- “Hartofilakidis classification focuses on acetabular development (preferred by some)
- “Shelf procedures augment lateral coverage but do not reorient acetabulum
Clinical Imaging
Imaging Atlas


Lateral center edge angle (CEA) under 25° is diagnostic. Normal is 25-40°. CEA measures lateral coverage of femoral head on AP radiograph. Tönnis angle greater than 10° indicates abnormal acetabular slope.
Based on femoral head migration. Type I = subluxation under 50%. Type II = 50-75%. Type III = 75-100%. Type IV = complete dislocation. Higher grades need femoral shortening to avoid sciatic nerve palsy.
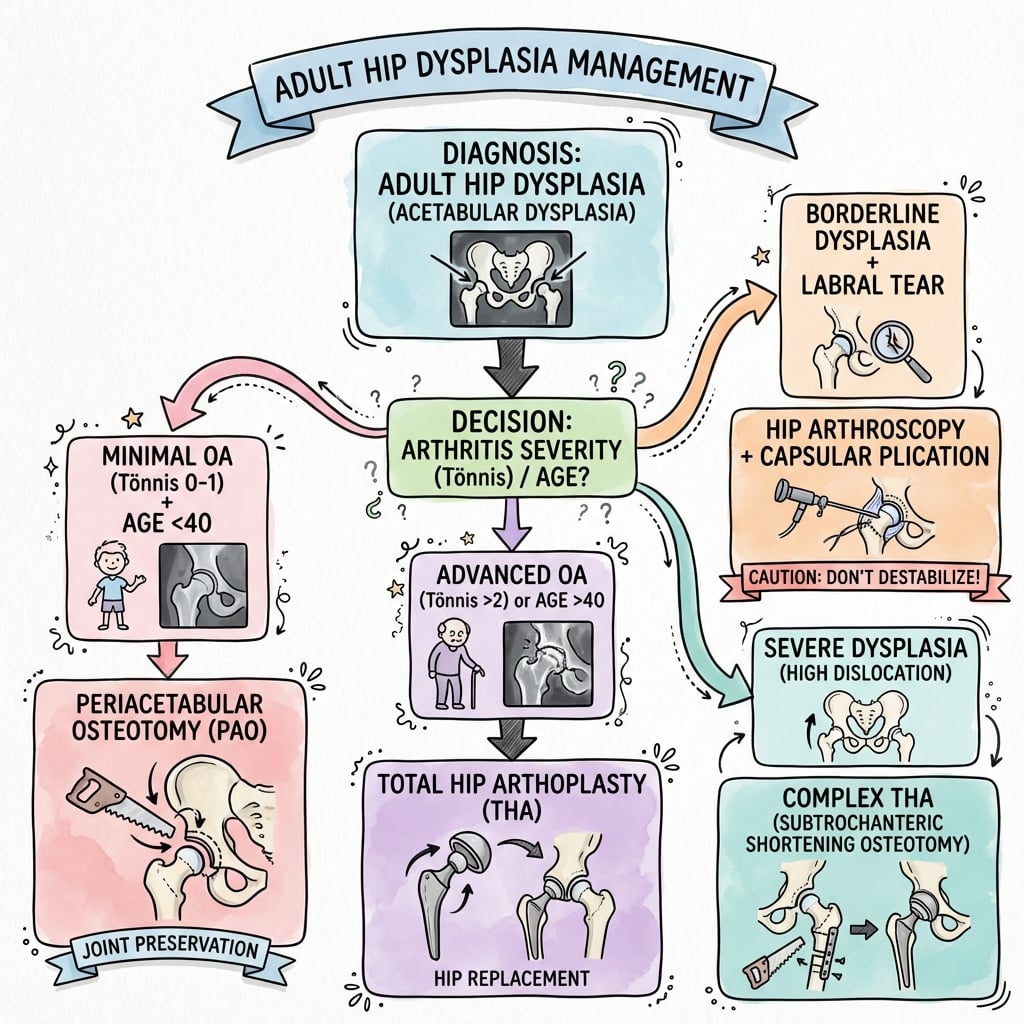
PAO for young patients under 40 with minimal arthritis (Tönnis grade 0-1). THA for older patients or established arthritis (Tönnis grade 2-3). Joint space must be preserved for PAO success.
Restore anatomy to true acetabulum. High hip center increases dislocation and wear. Femoral anteversion often increased (monitor during reaming). Sciatic nerve at risk with limb lengthening over 4cm.
| Patient Scenario | Crowe Grade | Treatment | Key Pearl |
|---|---|---|---|
| Age under 40, painful hip, preserved joint space | I (under 50% subluxation) | Periacetabular osteotomy (PAO) | Reorients acetabulum - best long-term preservation |
| Age under 40, early arthritis, CEA under 20° | I-II (50-75% subluxation) | Consider PAO if Tönnis grade under 2 | Success depends on remaining cartilage quality |
| Age over 50, established arthritis | I-II (under 75% subluxation) | THA - standard technique with small modifications | Restore center of rotation, avoid high hip center |
| Any age, severe dysplasia with dislocation | III-IV (over 75% subluxation) | THA with subtrochanteric shortening osteotomy | Lengthen under 4cm to protect sciatic nerve |
CASTRadiographic Assessment of Hip Dysplasia
Hook:CAST your assessment on plain films - these 4 measurements determine treatment!
HALFCrowe Classification of DDH
Hook:HALF way measures the hip's journey out of the socket - 50%, 75%, 100%!
CARTILAGEPAO Contraindications
Hook:Protect the CARTILAGE - if it's gone, PAO fails and THA is inevitable!
Overview and Epidemiology
Adult hip dysplasia represents persistent acetabular underdevelopment from infancy or childhood, leading to progressive hip instability and premature osteoarthritis. The condition is often undiagnosed in infancy and presents in early adulthood when symptomatic.
DDH is the leading cause of hip arthritis in women under 40. Early recognition allows joint-preserving surgery (PAO) before irreversible cartilage damage. Missed diagnosis leads to THA in the third or fourth decade.
- Female predominance: 9:1 ratio due to hormonal laxity
- Age at presentation: 20-40 years (painful subluxation)
- Bilateral: 20-30% have contralateral involvement
- Ethnic variation: Higher in First Nations, Southern Europeans
- 10% of total hip arthritis from DDH in young adults
- Progression: 50-75% develop arthritis by age 50 if untreated
- Quality of life: Significant functional limitation in third decade
- Economic: Early THA with high revision burden
Anatomy and Pathophysiology
Shallow acetabulum → increased contact stress → rim overload → labral tears → progressive cartilage loss → early arthritis. The lateral CEA measures this coverage - under 25° doubles contact stress on remaining cartilage.
Normal vs Dysplastic Acetabulum
| Feature | Normal Hip | Dysplastic Hip | Consequence |
|---|---|---|---|
| Lateral CEA | 25-40° | Under 25° | Increased joint reactive force |
| Tönnis angle | 0-10° | Greater than 10° | Lateral instability and migration |
| Acetabular anteversion | 15-20° | Often greater than 25° | Anterior instability, labral damage |
| Contact area | 500-600 mm² | Under 300 mm² | Doubled or tripled contact stress |
Associated Soft Tissue Pathology
- Anterosuperior labral tears: 90% of symptomatic DDH
- Hypertrophy from chronic edge loading
- Ossification in long-standing cases
- Intrasubstance degeneration
- Capsular laxity: Contributes to instability
- Redundancy in chronic subluxation
- Adhesions in false acetabulum (Crowe IV)
- Hypertrophic ligamentum teres
Classification Systems
Crowe Classification (Most Common)
Based on degree of femoral head migration superiorly, measured on AP pelvis radiograph.
| Grade | Femoral Head Position | Acetabular Development | Treatment Implications |
|---|---|---|---|
| I | Under 50% superior migration, mostly in socket | Shallow but identifiable acetabulum | Standard THA or PAO possible |
| II | 50-75% migration, at level of acetabular rim | Moderate deficiency, true acetabulum visible | THA requires shortening or high hip center |
| III | 75-100% migration, above acetabulum | Severely deficient, false acetabulum forming | Subtrochanteric osteotomy for anatomic placement |
| IV | Complete dislocation, no contact with true socket | Rudimentary acetabulum, well-developed false socket | Complex reconstruction with bone grafting |
Measure the distance from the inter-teardrop line to the center of the femoral head. Divide by the height of the pelvis (teardrop to iliac crest). Result under 10% = I, 10-15% = II, 15-20% = III, over 20% = IV.
Clinical Assessment
- Groin pain: Anterolateral or anterior, worse with activity
- Clicking or catching: Labral pathology common
- Instability: Sensation of subluxation or giving way
- Childhood history: Hip screening, bracing, or surgery
- Family history: DDH in relatives (genetic component)
- Age at onset: Typically 20-40 years when symptomatic
- Gait: Trendelenburg gait (abductor insufficiency)
- Leg length: Apparent shortening in high dislocation
- ROM: Usually preserved early, decreases with arthritis
- Impingement: Anterior pain with flexion-adduction-IR
- Apprehension: Clunk with flexion-abduction-ER (instability)
- Abductor strength: Often weak (lever arm dysfunction)
Contralateral hip is dysplastic in 20-30% of cases. Always obtain full pelvis radiographs, not just symptomatic side. Bilateral PAO may be staged 6-12 months apart.
Differential Diagnosis of the Painful Young Adult Hip
| Diagnosis | Distinguishing features | Key radiographic / imaging finding | Pitfall |
|---|---|---|---|
| Acetabular dysplasia (this topic) | Activity-related groin pain, instability sense, female predominance | Lateral CEA under 25°, Tönnis angle over 10°, broken Shenton's line | Borderline CEA 20-25° easily missed |
| Femoroacetabular impingement (cam/pincer) | Pain with deep flexion and pivoting, positive FADIR, often male (cam) | Alpha angle over 55°, crossover/posterior wall signs; CEA normal or high (pincer) | Dysplasia and impingement can coexist; do not over-resect the rim |
| Borderline dysplasia with excessive femoral anteversion | Instability symptoms; apprehension; anteverted femur | CEA 18-25° with femoral version 20° or more on CT | Isolated arthroscopy gives inferior results — consider PAO/femoral osteotomy |
| Isolated labral tear | Mechanical clicking/catching, positive FADIR, no global instability | Labral tear on MR arthrogram with normal CEA and version | Treating the labrum alone fails if underlying dysplasia is unrecognised |
| Established osteoarthritis | Rest and night pain, stiffness, loss of internal rotation | Joint-space loss, osteophytes, subchondral cysts (Tönnis 2-3) | Mislabels an arthritic hip as a PAO candidate |
| Sequela of childhood hip disease (Perthes, treated DDH, SUFE) | Childhood hip history, deformity, leg-length difference | Coxa magna/plana, residual subluxation, proximal femoral deformity | May need femoral as well as acetabular correction |
Special Clinical Tests
Physical Examination Sequence
Watch for Trendelenburg gait - trunk shifts over stance leg due to abductor weakness. Positive Trendelenburg test (pelvis drops on opposite side) in 40-60% of symptomatic DDH.
Apparent vs true shortening. In high dislocation, apparent shortening from pelvic tilt. Measure from ASIS to medial malleolus (true) and umbilicus to malleolus (apparent).
Assess flexion (normally 120°+), abduction (45°), adduction (30°), and rotation. Loss of internal rotation often first sign of arthritis. Document for PAO vs THA decision.
FADIR test (flexion-adduction-internal rotation) for anterosuperior labral tear. FABER test (flexion-abduction-external rotation) for posterior impingement or SI joint.
Investigations
Imaging Protocol
AP pelvis - weight-bearing, coccyx centered over pubic symphysis. Measure lateral CEA, Tönnis angle, assess arthritis grade. False profile view measures anterior CEA.
Key measurements:
- Lateral CEA under 25° = dysplasia
- Tönnis angle greater than 10° = lateral deficiency
- Anterior CEA under 20° = anterior deficiency
3D CT pelvis for surgical planning (PAO or THA). Assesses acetabular version, bony defects, location of true acetabulum in Crowe III-IV. Allows templating and virtual correction.
Gold standard for labral pathology. Sensitivity over 90% for labral tears. Assesses cartilage quality (Outerbridge grading). Helps determine PAO candidacy or need for arthroscopy.
In equivocal PAO candidates, arthroscopy can directly visualize cartilage. Outerbridge grade 3-4 changes = poor PAO candidate. Can address labral tears at time of PAO (staged or simultaneous).
Radiographic Measurements
| Measurement | Normal Range | Dysplasia Threshold | Clinical Significance |
|---|---|---|---|
| Lateral CEA (Wiberg) | 25-40° | Under 25° | Primary diagnostic criterion for lateral dysplasia |
| Tönnis Angle | 0-10° | Greater than 10° | Measures acetabular slope - predicts progression |
| Anterior CEA (false profile) | Greater than 20° | Under 20° | Anterior deficiency requires specific PAO correction |
| Acetabular Index (Sharp angle) | Under 40° | Greater than 43° | Alternative measure of lateral deficiency |
Management Algorithm
Initial Conservative Approach
Indications: Asymptomatic or mild symptoms, CEA 20-25° (borderline), older patients declining surgery.
Conservative Treatment Steps
Avoid high-impact activities (running, jumping). Low-impact exercise (swimming, cycling) maintains fitness without excessive loading. Weight management critical.
Strengthen hip abductors (gluteus medius) to compensate for biomechanical disadvantage. Core stability and pelvis control. Stretching hip flexors and IT band.
NSAIDs for symptom control (avoid chronic use). Paracetamol for baseline pain. Intra-articular steroid injection can provide temporary relief and confirm intra-articular source.
Annual radiographs to monitor progression. If joint space narrows or symptoms worsen despite therapy, surgical consultation indicated.
Progression to surgery is indicated when: (1) pain limits function despite therapy, (2) radiographic progression (joint space loss), or (3) patient desire for definitive treatment before irreversible damage.


Surgical Technique
Bernese Periacetabular Osteotomy - Step by Step
Positioning: Supine on radiolucent table with affected hip at table edge. C-arm access for AP and lateral views.
PAO Surgical Steps
Incision from ASIS along iliac crest. Dissect interval between sartorius (femoral nerve) and tensor fascia lata (superior gluteal nerve). Subperiosteal elevation of iliacus off inner table.
Through same incision, curved osteotome directed posteriorly and inferiorly to cut ischium 10mm medial to acetabular rim. This cut exits just medial to acetabulum posteriorly.
Straight osteotome directed medially along superior pubic ramus. Exit 10mm medial to acetabular rim anteriorly. Protect obturator neurovascular bundle with retractor.
From AIIS superiorly toward SI joint (10-15cm). Incomplete posteriorly to maintain posterior column continuity. Use curved osteotome. Monitor with fluoroscopy.
Complete ischial cut with Gigli saw passed from intrapelvic to extrapelvic. Mobilize fragment with Schanz pins. Rotate laterally and anteriorly to increase coverage.
Fix with 3-4 cortical screws from ilium into mobilized fragment. Confirm hip congruity and improved CEA (target 30-35°) on fluoroscopy. Avoid overcorrection (pincer).
Final lateral CEA should be 30-35° - adequate correction without overcorrection. Tönnis angle should be 0 to negative 5°. Confirm hip remains congruent through full ROM.
Complications

| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Sciatic nerve palsy (THA) | 1-5% (up to 10% in Crowe IV) | Lengthening over 4cm, inadequate shortening | Usually neurapraxia - observation, PT, may recover 6-18 months |
| Lateral femoral cutaneous nerve injury (PAO) | 10-15% | Smith-Petersen approach, excessive retraction | Usually temporary dysesthesia, resolves 3-6 months |
| PAO nonunion | 2-5% | Smoking, inadequate fixation, bone quality | ORIF with bone graft and plate if symptomatic |
| Intra-articular fracture (PAO) | 1-5% | Osteotomy extends into joint | Convert to THA if severe; ORIF if minimal displacement |
| THA dislocation | 5-10% (higher in DDH) | High hip center, component malposition, laxity | Closed reduction, brace, revision if recurrent |
| Aseptic loosening (THA) | 15-25% at 15 years | High hip center, inadequate bone stock, young age | Revision THA with bone grafting |
| Heterotopic ossification | 10-20% | Extensive dissection, male gender | Prophylaxis with indomethacin or radiation |
Immediate postoperative foot drop or numbness after THA in high dislocation = sciatic palsy. Document exam pre-closure. If noted immediately, consider shortening revision urgently (within 24-48 hours) to decompress nerve.
Postoperative Care and Rehabilitation
PAO Recovery Timeline
Touch weight-bearing with crutches. DVT prophylaxis (enoxaparin or rivaroxaban). Pain control with multimodal analgesia. Early mobilization to prevent stiffness.
Touch to 25% weight-bearing. Gentle hip ROM exercises. No active hip flexion against gravity (protects iliopsoas). Continue crutches. Monitor for signs of nonunion.
Increase to full weight-bearing if radiographs show healing. Formal physical therapy for abductor strengthening. Progress to single crutch then cane. Return to activities of daily living.
Full weight-bearing without aids. Progress to impact activities. Return to work (desk job 6-8 weeks, manual 3-4 months). High-impact sports delayed to 12 months.
Annual radiographs for 5 years to monitor for arthritis progression. Low-impact exercise encouraged. Watch for loss of ROM or recurrent pain (suggests progression).
PAO recovery is long - expect 3-4 months to full function. Patients should be counseled preoperatively. Peak improvement is 12-18 months. Some never regain pre-DDH athletic ability.
Outcomes and Prognosis
PAO Outcomes
| Outcome Measure | Success Rate | Key Determinants |
|---|---|---|
| Conversion to THA avoided at 10 years | 85-90% | Preop Tönnis grade 0-1, adequate correction, age under 40 |
| Patient satisfaction | 80-85% | Realistic expectations, good cartilage quality, minimal complications |
| Return to sports | 60-70% | Low-impact sports better outcomes than high-impact |
Tönnis grade 2 or higher at time of surgery predicts failure. Joint space under 2mm, patient age over 40, and inadequate correction (final CEA under 25°) also predict poor outcomes.
THA Outcomes in DDH
- Crowe I-II classification
- Anatomic cup placement
- Adequate bone stock
- Modern implants (highly cross-linked polyethylene)
- Proper leg length restoration
- Crowe III-IV classification
- High hip center
- Young patient age (under 50)
- Poor bone quality
- Femoral shortening osteotomy (adds complexity)
Registry signal: Across the major national joint registries, THA performed for developmental dysplasia carries a higher long-term revision burden than THA for primary osteoarthritis, driven mainly by younger age at surgery, severe (Crowe III-IV) dysplasia, a high hip centre and acetabular bone deficiency. Restoring the anatomic centre of rotation, securing durable acetabular fixation and using modern bearings are the principal modifiable factors.
Joint-preservation survivorship at a glance
| Follow-up | Hips preserved (free of THA) | Source | Key lesson |
|---|---|---|---|
| 15 years | Approximately 92% | Wells/Clohisy (Washington University) | Avoid overcoverage; treat concomitant cam |
| 20 years | Approximately 60% | Steppacher/Siebenrock (Bern) | Selection: minimal arthritis, no impingement signs |
| 30 years | Approximately 29% | Lerch/Siebenrock (Bern) | Tönnis grade 2 or more contraindicates PAO |
Evidence Base and Key Trials
A New Periacetabular Osteotomy for Hip Dysplasia (Bernese PAO — landmark)
- Original description of the Bernese periacetabular osteotomy through a single Smith-Petersen approach
- Allows extensive multiplanar acetabular reorientation without changing true pelvic diameter
- Posterior column left mechanically intact, permitting stable two-screw fixation and early partial weight-bearing
- Mean correction of 31° in the vertical (lateral) centre-edge angle of Wiberg
- Early complications: two intra-articular osteotomies, one transient femoral nerve palsy, one nonunion, heterotopic bone before indomethacin prophylaxis
Intermediate-Term Hip Survivorship and PROMs After PAO (Washington University)
- 154 hips (129 patients) with classic acetabular dysplasia followed a mean of 10.3 years
- Kaplan-Meier hip survival (endpoint THA) was 92% at 15 years; only 8 hips (5%) underwent THA
- Fair or poor preoperative joint congruency raised failure risk (OR 8.65)
- Postoperative lateral CEA over 38° (overcoverage) raised failure risk (OR 8.04)
- Concurrent head-neck osteochondroplasty was associated with reduced failure (OR 0.27)
Mean 20-Year Follow-up of the Bernese PAO
- First 75 hips treated at the originating institution, mean age 29 years, followed a mean of 20.4 years
- 60% of hips (41 of 68) preserved without conversion to THA at minimum 19 years
- Predictors of poor outcome: older age, lower preoperative Merle d'Aubigné-Postel score, positive anterior impingement test, limp, higher osteoarthritis grade, higher postoperative extrusion index
- Radiographic parameters stable over 20 years except osteoarthritis grade
Thirty-Year Survivorship After PAO for Hip Dysplasia
- Same originator cohort (75 hips) followed to a mean of 29 years (range 27-32)
- Cumulative survivorship free of THA, radiographic OA progression and pain was 29% at 30 years
- More than 70% eventually developed progressive osteoarthritis, pain or underwent THA
- Strong predictors of failure: preoperative Tönnis grade over 1 (HR 5.7), age over 40 (HR 4.3), postoperative acetabular retroversion (HR 4.8) and anterior overcoverage over 27% (HR 3.2)
PAO in Patients 40 Years and Older — Outcomes and Predictors of Failure
- 166 patients aged 40 years or older (mean 44), median follow-up 9.6 years
- Median survival was 17.0 years for Tönnis grade 0, 14.6 years for grade 1 and only 12.9 years for grade 2
- Higher preoperative Tönnis grade and worse WOMAC function predicted failure
- PAO remained effective in patients over 40 provided arthritis was absent or mild (Tönnis 0-1)
Proximal Placement of the Acetabular Component (High Hip Centre) — Long-Term Follow-up
- 37 complex cemented THAs in which the hip centre was placed proximally relative to the interteardrop line, mean follow-up 11 years
- 84% rated good or excellent; mean Harris hip score improved from 43 to 93
- 33 of 37 components were not displaced laterally — proximal placement without lateralisation was the key to acceptable results
- Six components (16%) loosened; only one required revision over the follow-up
Cementless THA with Subtrochanteric Shortening Osteotomy for Crowe IV DDH
- 21 Crowe IV hips reconstructed with a cementless stem and transverse subtrochanteric shortening osteotomy, cup placed at the anatomic hip centre, mean follow-up 5 years
- Mean Harris hip score improved from 36.2 to 90.8
- No osteotomy nonunions; one permanent sciatic nerve palsy and two early dislocations
- Allows reduction to the true acetabulum while limiting nerve stretch
Subtrochanteric Shortening with a Cemented Exeter Stem for Crowe IV DDH
- 18 Crowe IV hips treated with derotational subtrochanteric shortening osteotomy and a cemented Exeter stem, mean follow-up 114 months
- Significant improvement in Merle d'Aubigné-Postel pain, function and movement scores
- No postoperative sciatic nerve palsy; one osteotomy nonunion revised successfully
- Three acetabular revisions for aseptic loosening over the follow-up period
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old woman presents with 2 years of progressive left groin pain. Pain is worse with activity and relieved by rest. She has no history of childhood hip problems. Examination shows full ROM but positive FADIR test. AP pelvis radiograph demonstrates lateral CEA of 18°, Tönnis angle of 15°, and Tönnis grade 1 arthritis. What is your assessment and management?”
“A 58-year-old woman requires THA for severe arthritis secondary to DDH. Preoperative radiographs show Crowe type III dysplasia with the femoral head 5cm superior to the true acetabulum. She has a well-developed false acetabulum. Walk me through your surgical planning and technique.”
“You have just completed a THA for Crowe type II dysplasia in a 52-year-old woman. Intraoperative lengthening was approximately 3.5cm. In recovery, she has a complete foot drop and numbness over the dorsum of the foot. How do you manage this?”
MCQ Practice Points
Q: What is the normal range for the lateral center edge angle (Wiberg angle) and what value indicates dysplasia? A: Normal lateral CEA is 25-40°. A value under 25° indicates acetabular dysplasia. The CEA is measured on AP pelvis radiograph as the angle between a vertical line through the femoral head center and a line from the center to the lateral acetabular edge. It quantifies lateral coverage of the femoral head.
Q: Describe the Crowe classification of developmental hip dysplasia. A: Crowe classification grades DDH based on degree of femoral head superior migration: Type I = subluxation under 50% (head mostly in socket), Type II = 50-75% subluxation (head at rim level), Type III = 75-100% subluxation (head above socket), Type IV = complete dislocation with false acetabulum. Higher grades require femoral shortening to avoid nerve injury during THA.
Q: What are the key indications and contraindications for periacetabular osteotomy (PAO)? A: Indications: Symptomatic acetabular dysplasia (CEA under 25°), age under 40-45 years, minimal arthritis (Tönnis grade 0-1), preserved joint space (over 2mm). Contraindications: Advanced arthritis (Tönnis grade 2-3), inadequate cartilage (Outerbridge 3-4), reduced joint space (under 2mm), age over 45, large osteophytes. PAO success depends on remaining cartilage quality.
Q: What is the safe limit for limb lengthening during THA in dysplastic hips, and what is the risk of exceeding it? A: The safe limit for acute limb lengthening is generally under 4cm. Lengthening beyond this threshold significantly increases the risk of sciatic nerve palsy due to nerve stretch. In Crowe III-IV hips with greater than 4-5cm superior migration, femoral shortening osteotomy should be performed to allow anatomic cup placement without excessive lengthening. Sciatic nerve palsy incidence rises from 1-2% to 5-10% when lengthening exceeds 4cm.
Q: How do THA outcomes in developmental dysplasia compare to primary osteoarthritis? A: THA in DDH has higher revision rates than primary OA. Registry data shows 15-year revision rates of 15-25% for DDH vs 5-10% for OA. Poor prognostic factors include Crowe III-IV classification, young patient age (under 50), high hip center placement, and inadequate bone stock. Modern techniques emphasizing anatomic cup placement and femoral shortening when needed have improved outcomes.
Q: How does long-term joint-preservation survivorship after PAO change with follow-up, and what is the single most important predictor of failure? A: Survivorship free of conversion to THA falls progressively with time: around 92% at 15 years (Wells/Clohisy), about 60% at 20 years and roughly 29% at 30 years in the original Bern cohort (Steppacher, then Lerch). The dominant, consistent predictor of failure across these series is preoperative arthritis - a Tönnis grade of 2 or more is a contraindication. Older age, positive impingement signs, postoperative acetabular retroversion and anterior overcoverage also predict failure.
Guidelines, Registries & Global Practice
Global epidemiology
Developmental dysplasia of the hip is the single most important cause of secondary hip osteoarthritis in young adults, particularly women. There is striking geographic and ethnic variation: prevalence is high in populations with traditional swaddling (Eastern Europe, parts of the Mediterranean and the Middle East, some First Nations and Native American groups) and comparatively low in populations who carry infants in abduction. Late-presenting (adolescent and adult) dysplasia is over-represented in regions without universal neonatal hip screening, so a surgeon anywhere in the world should expect a spectrum from subtle borderline dysplasia to neglected Crowe IV high dislocation.
Major guidance, side by side
| Body / region | Core position on adult DDH | Evidence base |
|---|---|---|
| Bernese / EFORT-aligned hip-preservation consensus (Europe) | PAO is the reorientation osteotomy of choice in the skeletally mature dysplastic hip with congruent joint and Tönnis grade 0-1; correct to a lateral CEA in the low-to-mid 30s without overcoverage | Long-term originator cohorts (Ganz; Steppacher; Lerch) |
| AAOS / North American hip-preservation practice (US) | Joint preservation (PAO, with arthroscopy or osteochondroplasty for concomitant impingement) for symptomatic dysplasia with preserved cartilage; THA when arthritis is established | Multicentre PAO cohorts (Clohisy / ANCHOR group) |
| NICE / BOA (UK) | No DDH-specific surgical guideline; arthroplasty is governed by general hip-replacement standards emphasising shared decision-making, implant choice supported by registry data and routine registry submission | NICE NG157 (joint replacement); National Joint Registry |
| AO Foundation (technique reference) | Standardised description of Bernese PAO and of subtrochanteric shortening for high dislocation; emphasises preserving the posterior column and protecting the sciatic nerve | AO surgical reference / instructional material |
Registry evidence (arthroplasty)
The major national joint registries — the NJR (England, Wales, NI), AJRR (USA), AOANJRR (Australia), the Swedish (SHAR), Norwegian and New Zealand registries — consistently show that THA for developmental dysplasia revises more often than THA for primary osteoarthritis, with the excess risk concentrated in younger patients, severe (Crowe III-IV) deformity, high hip centres and bone-deficient acetabula. Registries also support uncemented acetabular fixation in good bone and a survival advantage for larger heads and modern cross-linked or ceramic bearings, all of which matter disproportionately in this young, high-demand population. Exact percentages differ between registries and reporting years, so quote the trend (higher revision burden) rather than a single number in a viva.
A common viva pivot is: "This patient could have been screened as a neonate — why are you seeing dysplasia now?" Be ready to discuss variability in neonatal screening, swaddling practices and late presentation, then move to a principle-based plan (preserve if cartilage allows, replace anatomically if it does not) that holds true regardless of health system.
Global practice variation
- 3D CT and software templating available for complex Crowe III-IV planning
- PAO concentrated in high-volume hip-preservation units (learning-curve dependent)
- Modern bearings and modular/uncemented implants routinely available
- Mandatory or near-universal registry submission
- Later presentation; more neglected high dislocations
- Reliance on plain radiographs and intra-operative judgement
- Cemented or basic uncemented constructs; restricted implant inventory
- Subtrochanteric shortening especially valuable where small, low-cost stems must reach the true acetabulum
Regardless of health system, document:
- Preoperative counselling: higher long-term revision burden than THA for primary OA, nerve-injury risk (rising with lengthening, up to 5-10% in high dislocation), and the long PAO recovery (3-4 months to full function)
- Surgical planning: imaging and templating for complex cases, with identification of the true acetabulum
- Informed consent: nerve palsy, dislocation, nonunion/intra-articular fracture (PAO) and the possibility of eventual conversion to THA
- Postoperative monitoring: a documented neurovascular examination immediately after THA in high dislocation
Key Measurements
- Lateral CEA under 25° = dysplasia (normal 25-40°)
- Tönnis angle greater than 10° = abnormal slope
- Anterior CEA under 20° = anterior deficiency
- Joint space under 2mm = poor PAO candidate
Crowe Classification
- Type I = under 50% subluxation (in socket) - standard THA or PAO
- Type II = 50-75% subluxation (at rim) - THA with shortening or high center
- Type III = 75-100% subluxation (above socket) - subtrochanteric osteotomy
- Type IV = complete dislocation - complex THA with femoral shortening
Treatment Algorithm
- Age under 40 + Tönnis 0-1 + CEA under 25° = PAO
- Age over 45 or Tönnis 2-3 = THA
- Crowe I-II = standard THA to true acetabulum
- Crowe III-IV = THA with femoral shortening (under 4cm lengthening)
- PAO success = 85-90% at 10 years if well selected
Surgical Pearls
- PAO: reorient acetabulum to CEA 30-35° (avoid overcorrection)
- THA: restore anatomy to true acetabulum, avoid high hip center
- Femoral shortening when lengthening would exceed 4cm
- Neuromonitoring for Crowe III-IV THA
- Long stem to bridge subtrochanteric osteotomy
Complications
- Sciatic nerve palsy: 1-5% (up to 10% in Crowe IV)
- LFCN injury in PAO: 10-15% (usually temporary)
- PAO nonunion: 2-5%
- THA dislocation: 5-10% (higher than primary OA)
- Revision rate: 15-25% at 15 years (vs 7-8% in OA)