High-energy traction injury of the young adult | Decide preganglionic versus postganglionic | Timing is everything | Build the arm with nerve transfers
- The injury: a high-energy traction injury, usually in a young man after a motorcycle crash - the force pulls the roots and trunks and can tear the root clean out of the spinal cord
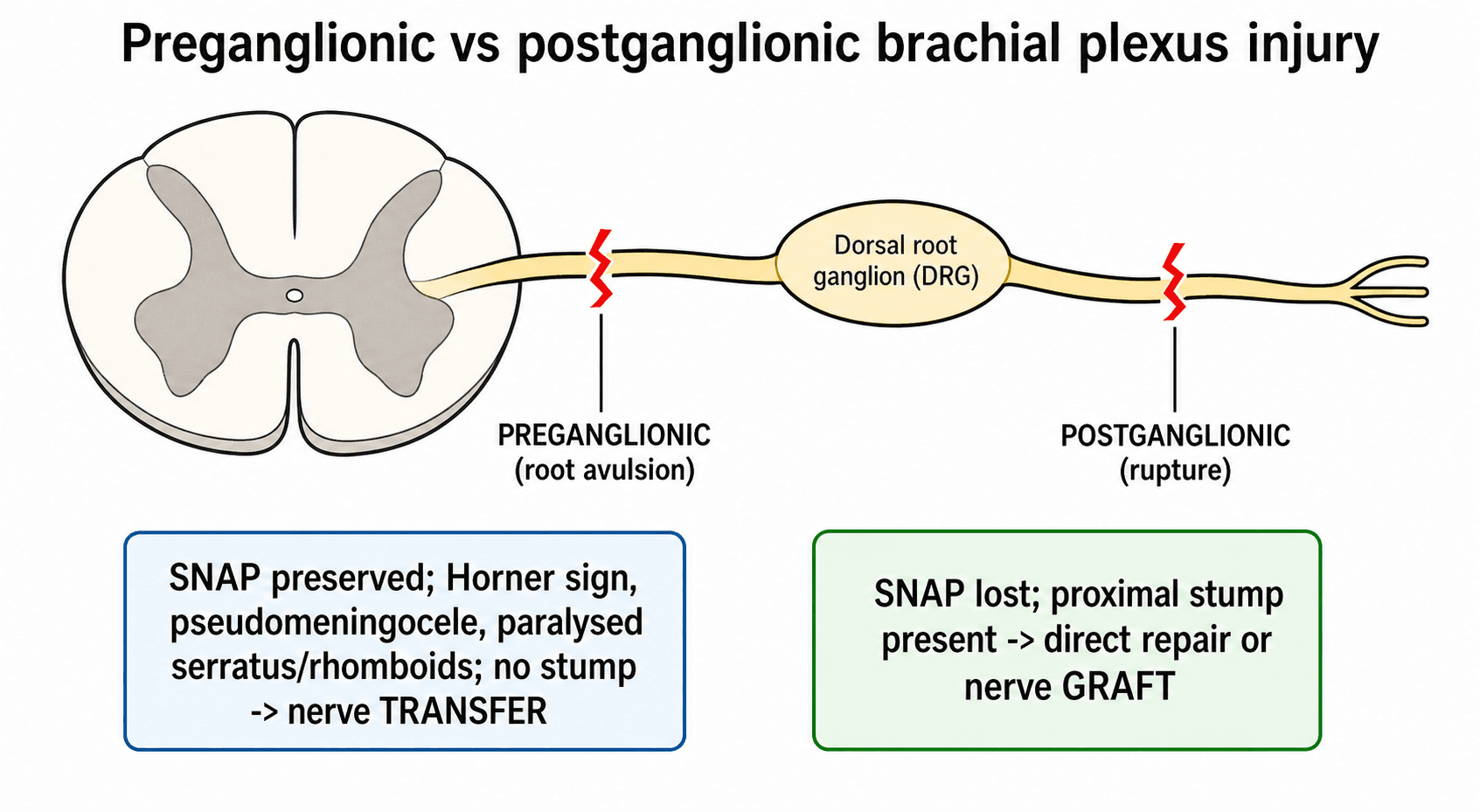
- The key split: a preganglionic (root avulsion) lesion is proximal to the dorsal root ganglion and cannot be repaired directly - it needs a nerve transfer; a postganglionic lesion is distal and may be grafted or may recover
- The clues to avulsion: a Horner's sign, winged scapula, paralysed rhomboids/serratus, preserved sensory nerve action potentials in an anaesthetic limb, and a pseudomeningocele on imaging - all point preganglionic
- Timing: reinnervate the muscle before it dies. Sharp/open injuries are explored early; closed traction injuries are usually reconstructed by 3 to 6 months, and results fall off sharply after about a year
- The priorities: restore elbow flexion first, then shoulder stability/abduction, then hand function - hand recovery is the hardest and least reliable goal
- “A Horner's sign (ptosis, miosis, anhidrosis) means a T1 root avulsion until proven otherwise - it is a marker of a severe, preganglionic, proximal injury
- “In a preganglionic injury the limb is anaesthetic but sensory nerve conduction is PRESERVED, because the cell body in the dorsal root ganglion is still connected to its peripheral axon - a classic exam discriminator
- “Elbow flexion is the first reconstructive priority, classically via an Oberlin (ulnar fascicle to biceps motor branch) transfer in upper plexus injury
- “Refer early to a specialist plexus centre - delayed referral is common and directly worsens the achievable outcome
This is the single most important decision. A preganglionic lesion (root avulsion) is proximal to the dorsal root ganglion - it cannot be repaired or grafted directly and needs a nerve transfer. A postganglionic lesion is distal and may be repaired, grafted, or recover. Get this wrong and you plan the wrong operation.
Ptosis, miosis (small pupil) and facial anhidrosis on the injured side mean the T1 sympathetic outflow has been disrupted - a marker of a lower root avulsion and a severe, proximal injury. Always look for it; it changes the prognosis and the plan.
In a preganglionic injury the limb is numb, but the sensory nerve action potential (SNAP) is preserved on nerve conduction studies. The dorsal root ganglion cell body and its peripheral axon are still connected, so the peripheral nerve conducts even though the brain receives nothing. Numb limb + present SNAP = avulsion.
Denervated muscle has a time limit. Sharp/open and vascular injuries are explored urgently; closed traction injuries are reconstructed by about 3 to 6 months and outcomes fall sharply after roughly a year. Delayed referral to a plexus centre is a common, avoidable cause of a poor result.
Overview
The brachial plexus is the network of nerves that carries motor and sensory signals from the lower cervical and first thoracic spinal nerves out to the whole upper limb. An adult traumatic brachial plexus injury is usually a high-energy traction injury - the classic patient is a young man thrown from a motorcycle, whose head and shoulder are forced apart so violently that the nerves are stretched, ruptured, or pulled out of the spinal cord altogether.
The result can be devastating: a partly or completely paralysed, numb, and often painful arm in a young, working person. For the exam, this topic rewards a clear, structured approach rather than memorised lists. Three threads run through everything: work out exactly where and how badly the plexus is injured (especially preganglionic versus postganglionic), act within the time window before denervated muscle is lost, and rebuild the limb in order of usefulness - elbow flexion first, then shoulder, then (rarely) hand.
It is worth separating this from brachial plexus birth palsy, a different obstetric traction problem in neonates with its own classification (Narakas) and a high rate of spontaneous recovery. The adult injury is higher-energy, recovers far less spontaneously, and the surgical decisions are driven hard by timing and by the preganglionic/postganglionic distinction.
Pathophysiology and Applied Anatomy
You cannot reason about a plexus injury without the anatomy, but you only need it at the level the examiner tests: which section is injured, and what that predicts.
The five sections run proximal to distal and are easy to remember as "Read Those Damn Cadaver Books" - Roots, Trunks, Divisions, Cords, Branches.
- Roots (C5, C6, C7, C8, T1): the spinal nerves emerging from the neck. The dorsal root ganglion (DRG) sits on the sensory root - its position is the anatomical basis of the whole preganglionic/postganglionic split.
- Trunks: C5+C6 form the upper trunk, C7 alone the middle trunk, C8+T1 the lower trunk - these lie in the supraclavicular region.
- Divisions: each trunk splits into an anterior and posterior division behind the clavicle.
- Cords (lateral, posterior, medial): named for their relation to the axillary artery, lying in the infraclavicular region.
- Branches: the terminal nerves - musculocutaneous, axillary, radial, median, ulnar.
Branches that come off very proximally are diagnostic flags. The dorsal scapular nerve (rhomboids) and long thoracic nerve (serratus anterior) arise from the roots themselves; the suprascapular nerve comes off the upper trunk. If these muscles are paralysed, the lesion is very proximal - pushing you toward a preganglionic root-level injury.
The dorsal root ganglion is the anatomical fulcrum of this whole topic. Sensory cell bodies live in the DRG. If the injury is proximal to the DRG (preganglionic), the peripheral sensory axon stays alive (so the SNAP is preserved) even though no signal reaches the cord. If it is distal to the DRG (postganglionic), the peripheral axon degenerates and the SNAP is lost. One anatomical fact explains a whole cluster of exam findings.
Pathophysiology: how the injury happens
Adult plexus injury is overwhelmingly a traction (stretch) injury. When the head and shoulder are forced apart - the classic motorcyclist thrown over the handlebars - the angle between neck and shoulder widens violently and the nerves are stretched beyond their limit.
- Where the nerve fails depends on the force and the anatomy. The upper roots (C5-C6) are tethered and tend to rupture distal to the DRG (postganglionic), whereas the lower roots (C8-T1) are less supported and are more prone to being avulsed from the cord (preganglionic). This is why a Horner's sign (T1) signals a severe, proximal, lower-root injury.
- Once an axon is disconnected from its cell body it undergoes Wallerian degeneration, and the denervated muscle it supplied begins an irreversible clock toward fibrosis. Regenerating axons advance only slowly (on the order of about a millimetre a day), which is precisely why reinnervation distance and timing dominate the surgical strategy - the closer and the sooner you can deliver new axons to a muscle, the better.
- Other mechanisms exist: a sharp/open laceration divides the plexus cleanly (favourable for early direct repair), and an infraclavicular injury is often produced by a shoulder dislocation or proximal humerus fracture dragging on the cords and branches.
Classification
Adult plexus injuries are classified in several overlapping ways. The exam wants you to combine them: where along the plexus, how severe the nerve lesion, and which functional pattern.
This is the decisive split - it determines whether direct repair is even possible.
- Preganglionic (root avulsion)
- Proximal to dorsal root ganglion - root torn from cord
- Postganglionic (distal to DRG)
- Distal to dorsal root ganglion - in trunk/cord/branch
- Preganglionic (root avulsion)
- No - there is no proximal stump to sew to
- Postganglionic (distal to DRG)
- Yes - if there is a healthy proximal stump
- Preganglionic (root avulsion)
- PRESERVED in an anaesthetic limb (cell body intact)
- Postganglionic (distal to DRG)
- Absent (peripheral sensory axon degenerates)
- Preganglionic (root avulsion)
- Horner's sign, paralysed rhomboids/serratus, pseudomeningocele, severe deafferentation pain
- Postganglionic (distal to DRG)
- Recovery may occur; signs localise more distally
- Preganglionic (root avulsion)
- Nerve TRANSFER (re-route a working donor)
- Postganglionic (distal to DRG)
- Neurolysis, direct repair, or nerve GRAFT
Clinical Assessment
A plexus assessment is a viva favourite because it is so structured. Frame it as history, then a systematic limb examination, then the special signs that localise the level.
These are high-energy poly-trauma patients - assess and resuscitate the whole patient first. Note the mechanism (motorcycle, fall, traction), associated fractures and vascular injury, and the time since injury (it drives the surgical clock).
Inspect for the posture (waiter's tip in upper injuries, flail arm in pan-plexus), wasting, a winged scapula (serratus/long thoracic), and swelling/bruising. Map the sensory loss by dermatome.
Grade every key muscle (MRC scale) by root/nerve so you can plot the level: deltoid and supraspinatus (C5), biceps (C5-C6), wrist/finger extensors (C7), finger flexors (C8), intrinsics (T1). Test rhomboids and serratus - their loss flags a very proximal injury.
Check the distal pulses and perfusion - vascular injury demands urgent action. Look hard for a Horner's sign, and document the Tinel sign in the supraclavicular fossa (an advancing Tinel suggests a postganglionic lesion with regenerating axons).
A brachial plexus injury rarely travels alone. Associated subclavian/axillary artery injury can threaten the limb and must be identified and treated urgently - the dramatic neurological deficit can distract from a cold, pulseless hand. Likewise, exclude an associated cervical spine injury and other major trauma before focusing on the plexus.
Investigations
Investigations exist to answer one question: for each root, is the lesion preganglionic or postganglionic, and is there anything to repair?
Nerve conduction studies and EMG are central and are usually most informative from about 3 to 4 weeks, once Wallerian degeneration has declared itself.
- A preserved sensory nerve action potential (SNAP) in an anaesthetic dermatome is the classic marker of a preganglionic lesion (the DRG cell body is still attached to its peripheral axon).
- EMG maps which muscles are denervated and, on serial testing, can show early reinnervation (nascent motor units) that argues for watchful waiting rather than surgery.
- Loss of paraspinal muscle (erector spinae) activity points to a very proximal, root-level lesion.
No single test is perfect, and imaging can miss avulsions (false negatives at a level that is in fact avulsed at exploration). The robust exam answer is: combine serial clinical examination, neurophysiology, and imaging (MRI +/- CT myelography) to build a picture - and accept that intra-operative exploration with nerve action potential recording is the final arbiter.


Management
Management is best structured as who to operate on, when, and what to do - then the non-surgical care that runs alongside.
Timing is the decision that dominates outcome. A denervated muscle has a limited time before it becomes fibrotic and can no longer be re-animated by reinnervation, so the whole strategy is to reconnect the nerve before that happens.
- Timing
- Immediate or early (primary repair)
- Reasoning
- Clean-cut ends can be repaired directly while they are identifiable
- Timing
- Urgent (with the vascular repair)
- Reasoning
- Limb perfusion takes priority; the plexus can be tagged/explored at the same time
- Timing
- Early (around 6-12 weeks)
- Reasoning
- No spontaneous recovery is possible - do not waste the muscle's time window
- Timing
- Explore/reconstruct by 3-6 months if no recovery
- Reasoning
- Allows neurapraxic/recovering lesions to declare themselves while staying inside the window
- Timing
- Reconstruct function, not nerves
- Reasoning
- Denervated muscle is lost - shift to tendon transfer, fusion, or free muscle transfer
This is why early specialist referral matters so much and why a delay of many months is so damaging.
The commonest avoidable failure is delay. Once a muscle has been denervated for too long (roughly beyond a year), even a perfect nerve operation will not re-animate it - you are then limited to tendon transfers, joint fusions, or free muscle transfer. Refer early; reconstruct inside the window.
Deafferentation Pain and Its Management
Deafferentation (avulsion) pain is one of the most disabling features of a preganglionic injury and a major determinant of quality of life - the topic flags it repeatedly, so the viva expects you to set out how it is treated. It is a crushing or burning pain in the anaesthetic limb, generated by hyperactive deafferented neurons in the dorsal horn after the root is torn from the cord.
- Option
- Neuropathic agents - gabapentinoids (gabapentin, pregabalin), a tricyclic (amitriptyline) or an SNRI (duloxetine)
- Note
- Opioids are relatively ineffective for deafferentation pain and are avoided long term
- Option
- TENS, physiotherapy, and crucially a multidisciplinary pain service with psychological support
- Note
- Pain is a major quality-of-life issue in a young patient and needs active, holistic management
- Option
- Successful reinnervation often reduces the pain
- Note
- A further reason to reconstruct early rather than wait
- Option
- Dorsal root entry zone (DREZ) lesioning - ablation of the hyperactive dorsal-horn neurons at the avulsed levels
- Note
- The most effective procedure specifically for root-avulsion pain; spinal cord stimulation is generally less effective for avulsion pain
For refractory pain after root avulsion, the specific surgical answer is DREZ (dorsal root entry zone) lesioning. It targets the hyperactive deafferented neurons in the dorsal horn at the avulsed segments and gives the best results for this particular pain; spinal cord stimulation, which works for many neuropathic pains, is comparatively disappointing for avulsion pain because the dorsal columns themselves are disconnected.
Complications
- Why it happens
- Severe avulsion, late surgery, distal (hand) targets
- Key point
- Hand reinnervation is the least reliable goal of all
- Why it happens
- Loss of sensory input after root avulsion
- Key point
- Severe, common, and a major hit to quality of life - treat actively
- Why it happens
- A flail limb left unmoved while awaiting reinnervation
- Key point
- Preventable with early, ongoing physiotherapy
- Why it happens
- Borrowing a working nerve/muscle
- Key point
- Choose expendable donors; deficit is usually minor but must be consented
- Why it happens
- Avulsion severity, late referral, target muscle loss
- Key point
- Salvage with tendon transfers, fusions, free muscle transfer, or prosthetics
- Why it happens
- Young, working patients with a disabled dominant limb
- Key point
- Often life-changing; needs holistic, multidisciplinary support
Prognostic Factors
The threads of prognosis are scattered through this topic; pulling them together into a single framework is exactly what a strong viva answer does when asked "what determines the outcome?".
- Favourable
- Upper plexus (C5-C6) - shoulder and elbow targets recover well
- Unfavourable
- Lower plexus (C8-T1) or pan-plexus - hand recovery is the least reliable goal of all
- Favourable
- Postganglionic with a healthy proximal stump (graftable)
- Unfavourable
- Multiple root avulsions - no proximal stump and few intraplexal donors
- Favourable
- Lower-energy or sharp/open (clean, early repair)
- Unfavourable
- High-energy traction (worse recovery, longer zone of injury)
- Favourable
- Reconstruction within the 3-6 month window
- Unfavourable
- Delay beyond about a year - denervated muscle is lost
- Favourable
- Proximal targets close to the donor (elbow, shoulder)
- Unfavourable
- Distal targets (hand intrinsics) - axons may not arrive before the muscle dies
- Favourable
- Several healthy expendable donors for transfer
- Unfavourable
- Few donors (extensive injury) forcing extraplexal donors or free muscle transfer
Whatever the pattern, hand reinnervation is the hardest and least reliable goal, because the regenerating axons must travel the greatest distance and arrive before the intrinsic muscles fibrose. This is why the reconstructive priorities are elbow flexion first, then shoulder, and why honest counselling aims for a useful "helper arm" rather than a normal hand. High energy and delay are the two most modifiable predictors of a poor result - hence the emphasis on early referral.
Clinical Relevance
Adult brachial plexus injury is a high-yield exam topic precisely because it integrates so much: applied neuroanatomy (the five sections and the dorsal root ganglion), examination skills (the special signs that localise a lesion), investigation logic (why a preserved SNAP in a numb limb means an avulsion), the physiology of denervation and the time window, and a clear reconstructive ladder. It is also a topic where the examiner wants to see judgement - recognising the limb-threatening vascular injury first, knowing when to wait and when not to, refusing to promise a normal arm, and referring early to a specialist centre. Master the preganglionic/postganglionic split, the timing principle, and the elbow-shoulder-hand order of priorities, and you can reason through almost any scenario they set you.
Guidelines, Registries and Global Practice
- Specialist, multidisciplinary care is the consistent global message: traumatic adult plexus injuries do best when managed early in dedicated centres combining orthopaedic/hand, plastic, and peripheral-nerve neurosurgery, with physiotherapy and pain services. Delayed referral is documented as common and as a driver of poorer results.
- Timing principles are broadly agreed: explore sharp/open and vascular injuries early; reconstruct closed traction injuries inside roughly a 3 to 6 month window before denervated muscle is lost; shift to reconstructive (tendon transfer, fusion, free muscle transfer) options for late presentations.
- Nerve transfers have shifted global practice over recent decades: distal nerve transfers (such as the Oberlin transfer for elbow flexion and spinal-accessory-to-suprascapular transfer for the shoulder) are now widely used, shortening reinnervation distance and improving outcomes, while nerve grafting remains the answer for graftable postganglionic ruptures.
- Outcome variation reflects injury severity and access: upper-plexus injuries reliably regain elbow and shoulder function, whereas hand recovery after lower-plexus or pan-plexus injury remains poor everywhere - so realistic goal-setting (a useful helper arm) is a universal part of consent and care.
- Mechanism and demographics differ by region: motorcycle and road-traffic trauma dominate in many low- and middle-income settings, shaping a younger, predominantly male, higher-severity caseload - a global epidemiological pattern rather than any single country's experience.
Memory aids
HARMSSigns of a Preganglionic (Avulsion) Injury
Hook:HARMS spells the harm of an avulsion - the most proximal, least repairable injury that forces you toward nerve transfer.
ESHReconstruction Priorities (in order)
Hook:Build the arm from the elbow out: Elbow, Shoulder, Hand - ESH. Get the elbow working and the patient gains a functional helper limb.
NGTFThe Reconstructive Ladder
Hook:Climb the ladder NGTF: Neurolysis, Graft, Transfer, Free muscle - escalating answers as the proximal nerve becomes less usable.
MCQ Practice Points
High-yield, single-best-answer style points that examiners turn into questions.
Q: A young man has an anaesthetic arm after a motorcycle crash, yet nerve conduction shows preserved sensory action potentials. What does this mean? A: A preserved SNAP in an insensate limb indicates a preganglionic (root avulsion) lesion - the dorsal root ganglion cell body keeps the peripheral sensory axon alive even though no signal reaches the cord. It points toward nerve transfer, not graft.
Q: Which clinical sign best indicates a T1 root avulsion? A: A Horner's sign (ptosis, miosis, anhidrosis) - it reflects disrupted T1 sympathetic outflow and flags a severe, proximal, lower-root preganglionic injury.
Q: Is a pseudomeningocele proof of root avulsion? A: No. It is a strong but imperfect sign - it is absent in a substantial proportion of genuine avulsions, so imaging is never a substitute for operative exploration with nerve action potential testing.
Q: What is the first reconstructive priority and the workhorse procedure for it? A: Elbow flexion, classically restored by the Oberlin transfer (ulnar nerve fascicle to the biceps motor branch) in an upper plexus injury with an intact C8-T1.
Q: Why does timing dominate the plan in a closed traction injury? A: Denervated muscle has a time limit before irreversible fibrosis - so closed traction injuries are generally reconstructed by 3 to 6 months, and beyond roughly a year the strategy shifts to tendon transfers, joint fusions, or free functioning muscle transfer.
At a Glance
- Answer
- Young man, high-energy traction (motorcycle crash)
- Answer
- Preganglionic (avulsion = transfer) vs postganglionic (graftable)
- Answer
- Numb limb with a PRESERVED sensory action potential (SNAP)
- Answer
- By about 3-6 months, before denervated muscle is lost
- Answer
- Elbow flexion, then shoulder, then hand (least reliable)
- Answer
- Oberlin transfer (ulnar fascicle to biceps motor branch)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old man is brought in after a high-speed motorcycle crash. His right arm hangs limp and he cannot move it. How do you assess and work him up?”
“The examiner asks you to explain the difference between a preganglionic and a postganglionic brachial plexus injury and why it changes your operation.”
The Big Picture
- High-energy traction injury, typically a young man on a motorcycle
- Decide preganglionic (avulsion) vs postganglionic FIRST
- Anatomy: Roots, Trunks, Divisions, Cords, Branches
- Patterns: upper (C5-6, best) / lower (C8-T1, worst) / pan-plexus
Signs of Avulsion (Preganglionic)
- Horner's sign (ptosis, miosis, anhidrosis) = T1 avulsion
- Preserved SNAP in an anaesthetic limb
- Paralysed rhomboids and serratus; winged scapula
- Pseudomeningocele on imaging; severe deafferentation pain
Investigations
- NCS/EMG from ~3-4 weeks (SNAP, denervation, reinnervation)
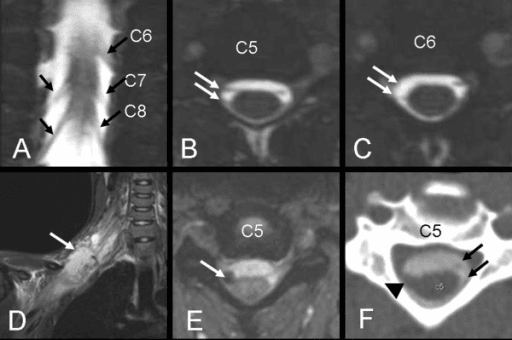
- MRI plexus + CT myelography for root avulsion
- Plain films/CT for fractures; chest film for phrenic palsy
- Exploration with NAP testing is the final arbiter
Management
- Sharp/open and vascular injuries = early/urgent surgery
- Closed traction: reconstruct by ~3-6 months (window!)
- Ladder: Neurolysis - Graft - Transfer - Free muscle (FFMT)
- Priorities: elbow flexion (Oberlin), then shoulder, then hand
Evidence
According to PubMed, the following studies support the key teaching points above.
Axial T2-DRIVE MR Myelography Is Highly Accurate for Preganglionic Injury
- Prospective study of 24 patients planned for brachial plexus reconstruction, with operative exploration as the reference standard
- Axial T2-DRIVE MR myelography accurately identified the specific avulsed roots in each patient (sensitivity 100%, specificity 97.1%, accuracy 98.1%)
- Absent or pauci-rootlet appearance was the most reliable sign of avulsion
- Pseudomeningoceles were present in only ~68% of avulsions, so the authors argue they should be a supporting (ancillary) sign rather than the primary one
Delayed Referral Is Common and Worsens the Achievable Outcome
- 84 adults with traumatic brachial plexus injury evaluated at two tertiary referral centres in a large US metropolitan area
- Nearly half (44%) presented to a plexus surgeon in a delayed time frame (more than 3 months from injury)
- Global palsy was the most common pattern (39%), followed by upper-trunk and infraclavicular patterns
- Motorcycle-accident mechanism and certain system/insurance factors were associated with delayed referral
Reconstruction Can Restore Useful Elbow Flexion Even in Older Patients
- 58 patients older than 50 underwent nerve grafting, nerve transfer, or free functioning muscle transfer for elbow flexion after traumatic brachial plexus injury
- Mean elbow flexion grade improved from 0.26 to 2.63; 60% achieved functional flexion of M3 or better, versus none preoperatively
- More patients reached M3 or better with nerve transfers (69%) than with free functioning muscle transfer (43%)
- High-energy injuries did worse, but age itself did not correlate with the flexion grade achieved
Global Plexus Injury: Nerve Transfers Restore Elbow and Shoulder, Hand Stays Hard
- Concise review of surgical approaches for traumatic global (pan-plexus) brachial plexus injury, which predominantly affects adults
- Primary reconstruction relies mainly on single or multiple nerve transfers, with or without nerve grafts, to power targeted muscles
- Outcomes are best for restoring elbow flexion and shoulder abduction; wrist and hand function remain the hardest to recover
- Free functioning muscle transfer is the main option for delayed presentations or after failed nerve transfer