Coronal Condyle Fracture | Letenneur Classification | AP Lag Screws | AVN Risk
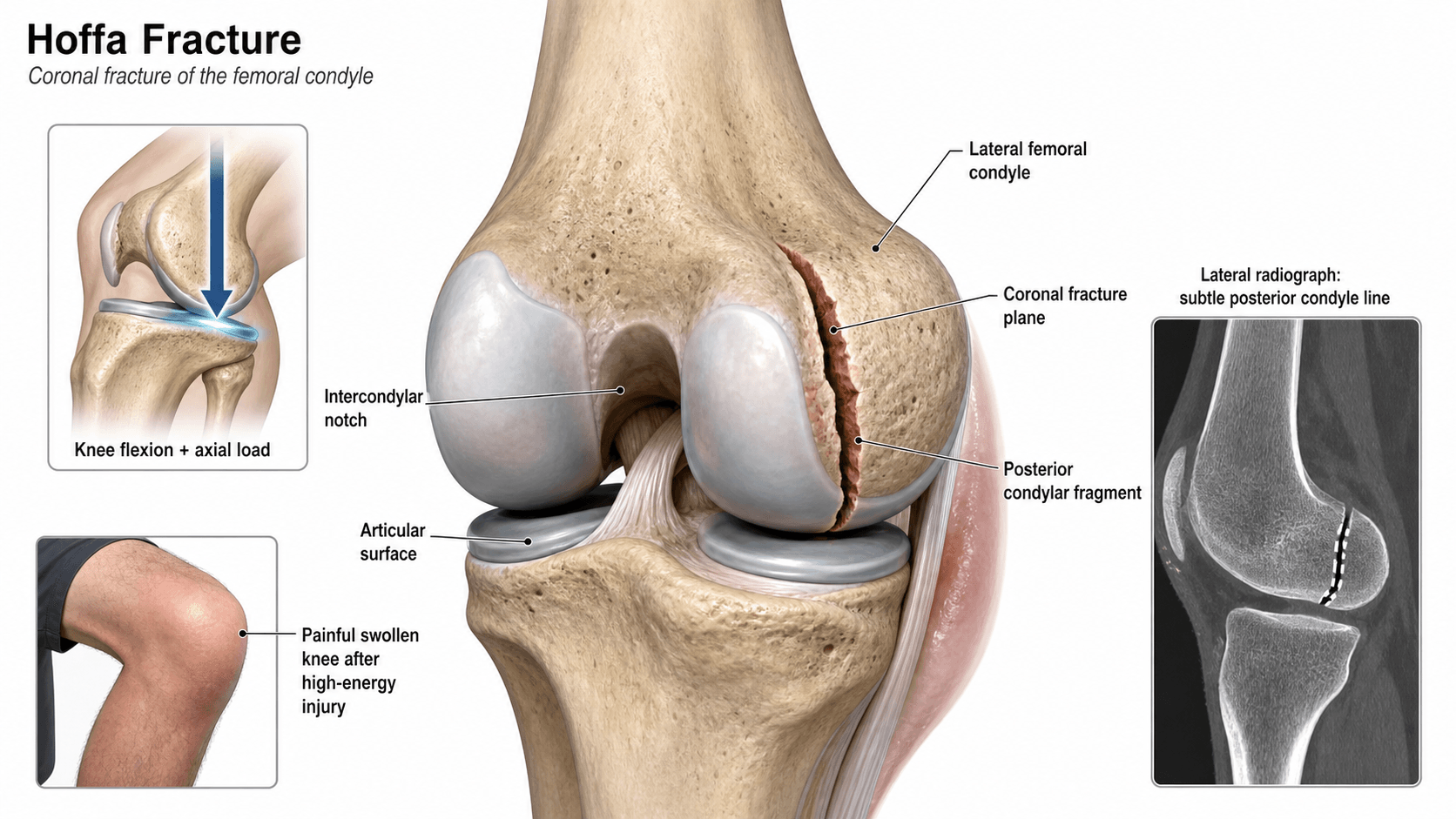
- A Hoffa fracture is a coronal-plane intra-articular fracture of the posterior femoral condyle; the lateral condyle is affected two to three times more often than medial.
- The AP radiograph misses the fracture because the fracture line is parallel to the beam; the true lateral film and CT are essential.
- ORIF with anterior-to-posterior lag screws from the intact anterior cortex is the standard; the posterior cortex is the fracture surface and offers poor fixation purchase.
- The Letenneur classification predicts AVN risk: Type I (no posterior cortex attachment) carries the highest risk because the fragment depends on capsular soft-tissue attachments alone.
- “Nork et al. found Hoffa fragments in 38 percent of supracondylar-intercondylar distal femoral fractures — always look for one on CT.
- “The mechanism is axial load through the femoral condyle with the knee flexed beyond 90 degrees — the tibial spine drives into the posterior condyle.
- “Headless compression screws (Acutrak or Herbert type) sit flush without countersinking and are a good alternative to standard lag screws.
- “Posterior approaches risk the popliteal vessels and common peroneal nerve and provide weaker fixation purchase.
The fracture line lies in the coronal plane, parallel to the X-ray beam on the AP view. A normal AP film does not exclude a Hoffa fracture. Lipohaemarthrosis on the AP film is the clue.
The true lateral shows the posterior condylar fragment as a double cortex or step. CT with sagittal and coronal reconstructions defines the fragment, displacement, comminution, and associated injuries.
Nork et al. found Hoffa fragments in 38 percent of supracondylar-intercondylar distal femoral fractures when CT was performed routinely. Any distal femoral fracture warrants CT to exclude one.
Even undisplaced fragments tend to shift under extensor mechanism forces and weight-bearing. Non-operative treatment has a high failure rate. ORIF is the standard for virtually all Hoffa fractures.
| Feature | Detail | Key Point |
|---|---|---|
| Fracture plane | Coronal (parallel to AP beam) | Easily missed on AP radiograph |
| Location | Lateral condyle (2-3x more than medial) | Lateral bears more load in deep flexion |
| Key imaging | True lateral + CT sagittal/coronal | AP film alone is inadequate |
| Classification | Letenneur I, II, III | Predicts AVN risk by posterior cortex attachment |
| Treatment | ORIF: AP lag screws, anterior approach | Anterior cortex intact — solid screw purchase |
HOFFARemember the key features of a Hoffa fracture
Hook:HOFFA fractures are Hidden On the AP, Found Only with Fluoroscopy and CT — Always fix!
LETLetenneur classification — AVN risk
Hook:LET the cortex guide you — Type I Lost it, Type II Earned it back, Type III is Third and rare.
APSCREWSurgical fixation principles
Hook:APSCREW: Anterior approach, Position flexed, Screws anterior-to-posterior, Countersink heads, Reduce first, Extend with plate if needed, Wound and rehab.
Overview and Epidemiology
A Hoffa fracture is an intra-articular coronal-plane fracture of the posterior femoral condyle. The fracture line runs roughly parallel to the sagittal axis of the knee, separating a posterior condylar fragment from the remaining distal femur. It was first described by Albert Hoffa in 1904.
Epidemiology
- Accounts for less than one percent of all distal femoral fractures — a genuinely rare injury.
- The lateral condyle is involved two to three times more often than the medial. Bicondylar Hoffa fractures (both condyles affected) are reported but uncommon.
- Bimodal age distribution: high-energy mechanisms in younger adults, lower-energy falls in elderly osteoporotic bone.
- More common in males, consistent with higher-energy trauma patterns.
Mechanism of injury
- The classically described mechanism is a direct axial load transmitted through the femoral condyle with the knee in greater than 90 degrees of flexion — the tibial spine or posterior rim of the tibial plateau drives into the posterior aspect of the femoral condyle, shearing off a coronal fragment.
- Dashboard injury: the patella is driven posteriorly against the distal femur with the knee flexed in a motor vehicle collision, compressing the posterior condyle against the tibial plateau.
- Falls from height and sporting injuries in young patients; ground-level falls in the elderly.
- The lateral condyle is more vulnerable because it bears a greater proportion of the transmitted load, is more anteriorly prominent, and the tibial spine preferentially contacts it in deep flexion.
The Hoffa fracture is far more common as a component of a supracondylar-intercondylar distal femoral fracture than as an isolated injury. Nork et al. identified Hoffa fragments in 38 percent of such injuries when CT was performed routinely. Always request CT for any distal femoral fracture pattern.
Pathophysiology and Mechanism
Why the coronal plane fractures In deep knee flexion (beyond 90 degrees), the posterior aspect of the femoral condyle is the primary weight-bearing surface and bears the full brunt of the transmitted axial load through the tibial plateau. The tibial spine contacts the lateral condyle preferentially because it is more anteriorly prominent. When the force exceeds the bone's resistance — either acutely in normal bone or with lower energy in osteoporotic bone — a coronal shear fracture occurs through the posterior condyle.
Why the lateral condyle predominates
- The lateral femoral condyle is broader, more anteriorly prominent, and projects further posteriorly than the medial condyle in deep flexion.
- In the flexed knee, the mechanical axis shifts laterally, concentrating more load on the lateral side.
- The tibial eminence contacts the lateral condyle earlier and with greater force during axial loading.
Associated injuries and patterns
- Hoffa fragments are frequently associated with supracondylar, intercondylar, or bicondylar distal femoral fractures (Nork: 38 percent of such patterns).
- The coronal fragment may be the only fracture component (isolated Hoffa), but this is less common.
- In polytrauma, always check for ipsilateral femoral shaft fractures, patellar fractures, ligamentous injuries, and neurovascular compromise.
Classification Systems
The Letenneur classification (1978) is the most widely used system and groups Hoffa fractures by the fracture plane and its relationship to the posterior femoral cortex, which directly predicts the vascular supply to the fragment and the risk of avascular necrosis.
| Type | Location | Fracture Plane | Posterior Cortex | AVN Risk |
|---|---|---|---|---|
| Type I | Lateral condyle | Fracture line parallel to posterior femoral cortex; fragment entirely distal with no cortical bridge | Fragment detached from posterior cortex | Highest — supplied only by posterior soft-tissue attachments |
| Type II | Lateral condyle | Oblique fracture from posterior cortex to articular surface; fragment retains partial posterior cortex attachment | Fragment retains posterior cortex attachment | Lower — capsular vessels along posterior cortex preserved |
| Type III | Medial condyle | Fracture involves the medial femoral condyle; plane similar to Type I or II on the medial side | Variable | Generally lower — medial genicular supply tends to be preserved |
In the viva, explain why the Letenneur classification matters for prognosis. The distinction between Type I and Type II is not merely anatomical — it predicts the residual blood supply. A Type I fragment stripped from the posterior cortex depends on flimsy capsular attachments for viability. A Type II fragment keeps a cortical bridge that preserves the capsular vascular leash.
Clinical Presentation
History
- High-energy mechanism in a young patient (road traffic crash, fall from height, sport) or a low-energy fall in an elderly patient.
- Pain, swelling, and inability to weight-bear.
- The knee is typically held in a slightly flexed, painful position.
- Often an associated injury: other lower-limb fractures, ipsilateral femoral shaft fracture, or intra-abdominal and chest injuries in polytrauma.
Physical examination — practical sequence
- Look: knee swelling (haemarthrosis), bruising over the distal thigh and knee, visible deformity if displaced or if associated with a supracondylar component.
- Feel: diffuse tenderness over the distal femur; focal tenderness over the posterior or posterolateral condyle is suggestive but difficult to elicit in an acute swollen knee. A large haemarthrosis is present. A palpable gap or step is rarely detectable clinically.
- Move: painful and restricted range of motion, especially flexion. Passive flexion reproduces condylar loading and pain.
- Special tests: valgus and varus stress tests in full extension to assess collateral ligament integrity (unreliable in the acute setting). A Lachman test is usually not possible or interpretable due to pain.
- Always: assess neurovascular status (popliteal pulse, dorsalis pedis pulse, capillary refill, sciatic and common peroneal nerve function) and check compartments, particularly after high-energy mechanisms.
A Hoffa fracture is a clinical chameleon — the patient presents like any distal femoral fracture with a swollen, painful knee and haemarthrosis. The coronal component is invisible on the AP film. The diagnosis depends on a high index of suspicion, correct imaging, and routine CT for any distal femoral injury.
Investigations
| View | What It Shows | Role |
|---|---|---|
| AP radiograph | Often normal or shows only a subtle sclerotic line; fracture plane parallel to the beam | Routine but insensitive — never exclude the fracture on AP alone |
| True lateral radiograph | Coronal fragment separation, double cortex sign, posterior condyle displacement | Key plain-film view; examine carefully for posterior condylar step |
| Oblique views (internal and external rotation) | May improve visualisation by angulating beam relative to fracture plane | Helpful but not a substitute for CT |
The double cortex sign on the true lateral view is the characteristic finding: a second cortical line is visible posterior to the normal posterior femoral cortex, representing the displaced fragment. A lipohaemarthrosis (fat-fluid level in the suprapatellar pouch on the lateral or cross-table lateral film) confirms an intra-articular fracture and should prompt CT even if no fracture is clearly seen.
Management
| Factor | Non-Operative | Operative (ORIF) |
|---|---|---|
| Indications | Exceptional only: truly undisplaced, patient absolutely not surgical candidate (critical illness, end-of-life) | Virtually all Hoffa fractures; any displacement greater than 2 mm, most undisplaced fractures in active patients |
| Regimen | Strict non-weight-bearing 8-12 weeks, long leg cast or hinged brace in extension | ORIF then early CPM; non-weight-bearing 6-8 weeks progressing to full |
| Secondary displacement rate | High — extensor mechanism forces and weight-bearing shift the fragment | Low with stable fixation and protected weight-bearing |
| Outcome | Poor in most series — residual pain, stiffness, secondary arthritis | Good to excellent in 70-80 percent with anatomical reduction |
Complications and Prognosis
| Complication | Details | Management |
|---|---|---|
| Avascular necrosis of the fragment | Up to 10-15 percent; commonest with Letenneur Type I; presents weeks to months post-fixation as fragment collapse or persistent pain | MRI for detection; small collapsed fragment may be excised; larger viable fragment with early changes monitored |
| Post-traumatic osteoarthritis | Common medium to long term; strongly correlated with residual articular step greater than 2 mm | Monitor and manage symptomatically; arthroplasty reserved for end-stage disease in older patients |
| Knee stiffness | Loss of flexion from intra-articular scarring, adhesions, and prolonged immobilisation | Early CPM and physiotherapy; manipulation under anaesthesia after confirmed union (approximately 6 months) |
| Hardware irritation | Prominent anterior screw heads palpable beneath extensor mechanism | Hardware removal after confirmed union (12-18 months) |
| Infection | Deep infection rate approximately 2-5 percent after distal femoral ORIF | Urgent washout and debridement; retain hardware if stable; culture-directed antibiotics |
| Malunion and nonunion | Usually from inadequate reduction or fixation, or premature weight-bearing | Revision ORIF with bone grafting for nonunion |
| Neurovascular injury | Popliteal artery, tibial nerve, common peroneal nerve at risk from injury and posterior approaches | Pre-operative vascular assessment essential; CT angiogram if pulses absent or ankle-brachial index abnormal |
| Compartment syndrome | Rare but possible with high-energy mechanisms and associated soft-tissue injury | Vigilance and serial compartment checks mandatory; fasciotomy if confirmed |
Functional outcome is strongly correlated with: the quality of articular reduction (residual step greater than 2 mm predictably leads to earlier arthritis), the Letenneur type (Type I carries worse prognosis), the time to diagnosis (delayed diagnosis worsens outcome), and the presence of comminution or associated distal femoral fracture patterns. Good to excellent results are reported in 70 to 80 percent of cases with anatomical reduction and stable fixation.
Evidence Base
The association between supracondylar-intercondylar distal femoral fractures and coronal plane (Hoffa) fractures
- Hoffa fractures identified in 38 percent of supracondylar-intercondylar distal femoral fractures when CT was routinely performed
- The coronal fragment was missed on initial radiographs in a significant proportion of cases
- Lateral Hoffa fragments were more common than medial
Coronal fractures of the lateral femoral condyle
- Clinical series of coronal lateral femoral condyle fractures treated with ORIF
- Good or excellent results in the majority of patients with anatomical reduction and stable fixation
- Outcome correlated with the quality of articular reduction rather than the Letenneur type alone
Plate fixation for Letenneur type I Hoffa fracture: a biomechanical study
- Biomechanical comparison of fixation constructs for Letenneur type I Hoffa fractures using cadaveric specimens
- Anterior plate with lag screws provided superior stability compared with lag screws alone or posterior plate constructs
- Anterior-to-posterior lag screw orientation was biomechanically stronger than posterior-to-anterior screw placement
Hoffa Fractures: Current Understanding and Surgical Treatment Strategies
- Comprehensive modern review of Hoffa fracture classification, imaging, fixation strategies, and outcomes
- ORIF via an anterior approach with AP lag screws remains the standard; headless compression screws and anterior buttress plates recommended for specific patterns
- Non-operative treatment has a high failure rate and is reserved only for undisplaced fractures in non-surgical candidates
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 26-year-old motorcyclist is brought to the emergency department after a high-speed collision. He has a painful, swollen left knee and cannot weight-bear. AP radiographs of the knee appear normal apart from a small lipohaemarthrosis. What would you do next?”
“A 42-year-old woman is referred to your clinic 4 months after internal fixation of a lateral Hoffa fracture. Her wound has healed but she reports persistent anterior knee pain on stairs and deep flexion, and her range of motion is limited to 90 degrees. Radiographs show the condylar fragment in position but with screw heads prominent at the anterior cortex. How would you assess and manage this?”
Definition and key facts
- Coronal-plane intra-articular fracture of the posterior femoral condyle (lateral commonest, 2-3:1)
- Less than one percent of distal femoral fractures; rare but easily missed
- Mechanism: axial load through the condyle with the knee in greater than 90 degrees of flexion
Imaging essentials
- AP radiograph: frequently misses the fracture — fracture line is parallel to the beam
- True lateral radiograph: the key plain-film view; look for posterior condylar separation or double-density sign
- CT with sagittal and coronal reconstructions: mandatory for all suspected cases
- Associated Hoffa fragment in 38 percent of supracondylar-intercondylar distal femoral fractures (Nork)
Letenneur classification
- Type I (lateral): fragment detached from posterior cortex — highest AVN risk
- Type II (lateral): fragment retains posterior cortex attachment — capsular vessels preserved
- Type III (medial): rare; generally better vascularised via medial genicular supply
Surgical fixation
- ORIF is the standard for virtually all Hoffa fractures
- Anterior approach (lateral or medial parapatellar); posterior approach reserved for specific indications
- AP lag screws from intact anterior cortex: two to three 6.5 mm or 4.0 mm cancellous screws or headless compression screws
- Countersink screw heads or use headless screws to prevent extensor mechanism irritation
Complications
- Avascular necrosis: up to 10-15 percent, especially Letenneur Type I; investigate with MRI
- Post-traumatic osteoarthritis: correlated with residual articular step greater than 2 mm
- Knee stiffness: early CPM and physiotherapy are critical; manipulation under anaesthesia if needed
- Hardware irritation: prominent anterior screw heads may need removal after confirmed union