Hypothenar Hammer Syndrome
- The THUMB is spared (radial artery / deep arch) - the ulnar artery feeds the ulnar digits (ring/little ± middle). A thumb-and-index pattern is NOT HHS. This thumb-sparing, ulnar-sided, unilateral, dominant-hand pattern is the whole diagnosis.
- Don't call it Raynaud's - true Raynaud's is usually bilateral, symmetrical and involves the thumb. HHS is secondary, unilateral and occupational.
- Angiography is the reference standard (corkscrew ulnar artery, occlusion, aneurysm); duplex/Allen's are first-line screens. Don't stop at a normal plain radiograph.
- An aneurysm is an ongoing EMBOLIC SOURCE - resect it; don't just anticoagulate and watch if there is ongoing embolisation/critical ischaemia.
- Before LIGATING, prove collateral supply (Allen's to the radial side / imaging); reconstruct (interposition vein/arterial graft) if collaterals are inadequate AND distal targets are good - a graft into poor runoff thromboses.
- Stop the trauma and stop smoking in EVERY patient - without these, recurrence is likely whatever the index treatment (recurrence ~28% in the long-term series).
- The ulnar artery at the wrist is the commonest site of an upper-limb arterial aneurysm - a favourite one-liner.
Overview & Epidemiology
Hypothenar hammer syndrome (HHS) is the classic occupational vascular hand condition - an uncommon but high-yield cause of ulnar-sided digital ischaemia that the exam loves because the history, the localising pattern and the mechanism are so distinctive.
- Demographics: predominantly men in manual occupations (factory workers, masons, carpenters, mechanics, metalworkers) using the heel of the hand as a tool, plus vibrating-tool users and some athletes (martial arts, baseball, mountain biking, handball). A recognised occupational disease.
- Long exposure: in the largest long-term series the mean duration of repetitive palmar trauma at diagnosis was ~21 years, and HHS accounted for only ~1% of Raynaud-phenomenon referrals.
- Laterality: typically unilateral (~87%), affecting the dominant hand (~93%).
- Why examiners care: it is the prototypical hammer-and-anvil vascular injury, with a clean localising pattern (thumb-sparing, ulnar digits) and a real conservative-vs-surgical debate.
Pathophysiology & anatomy
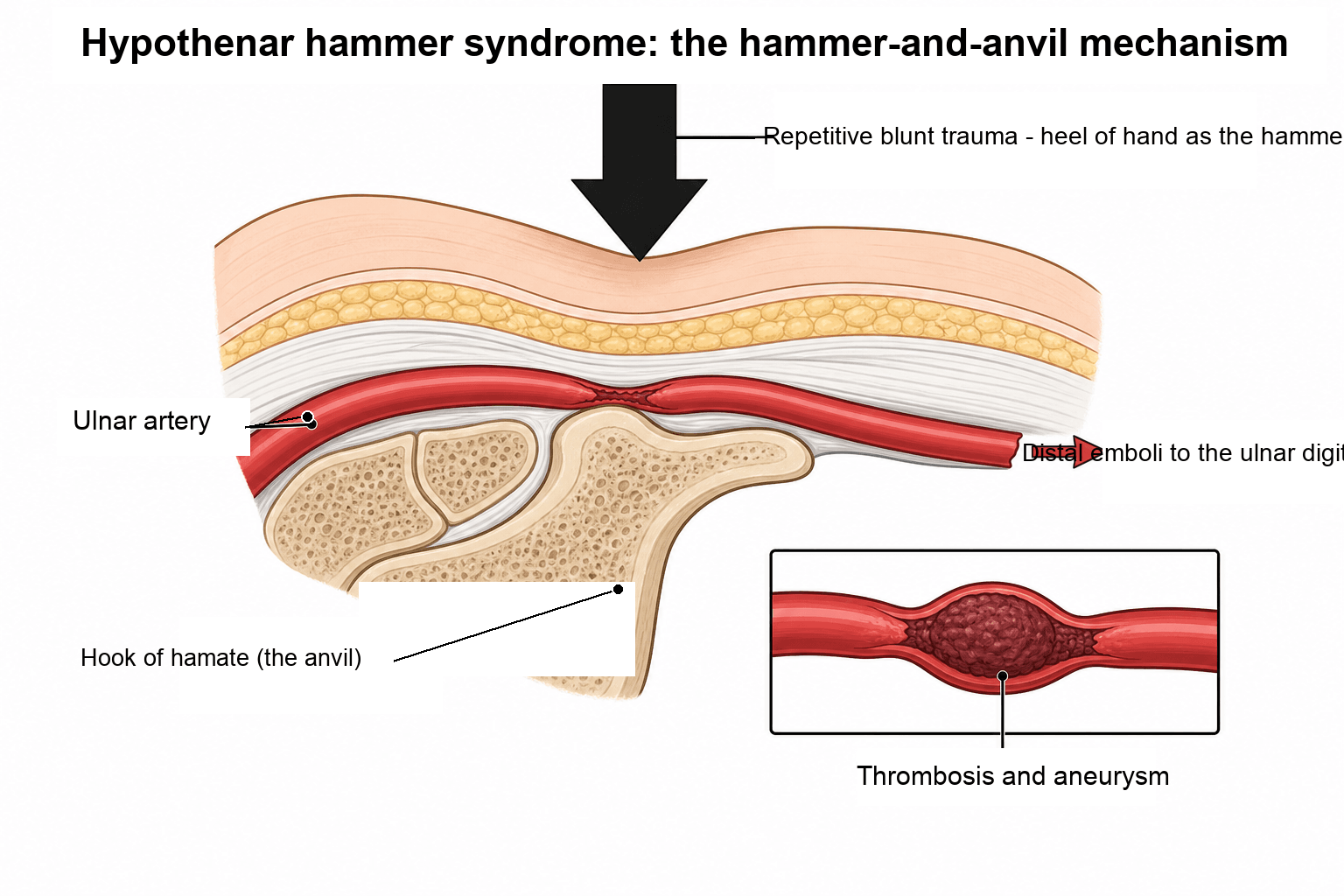
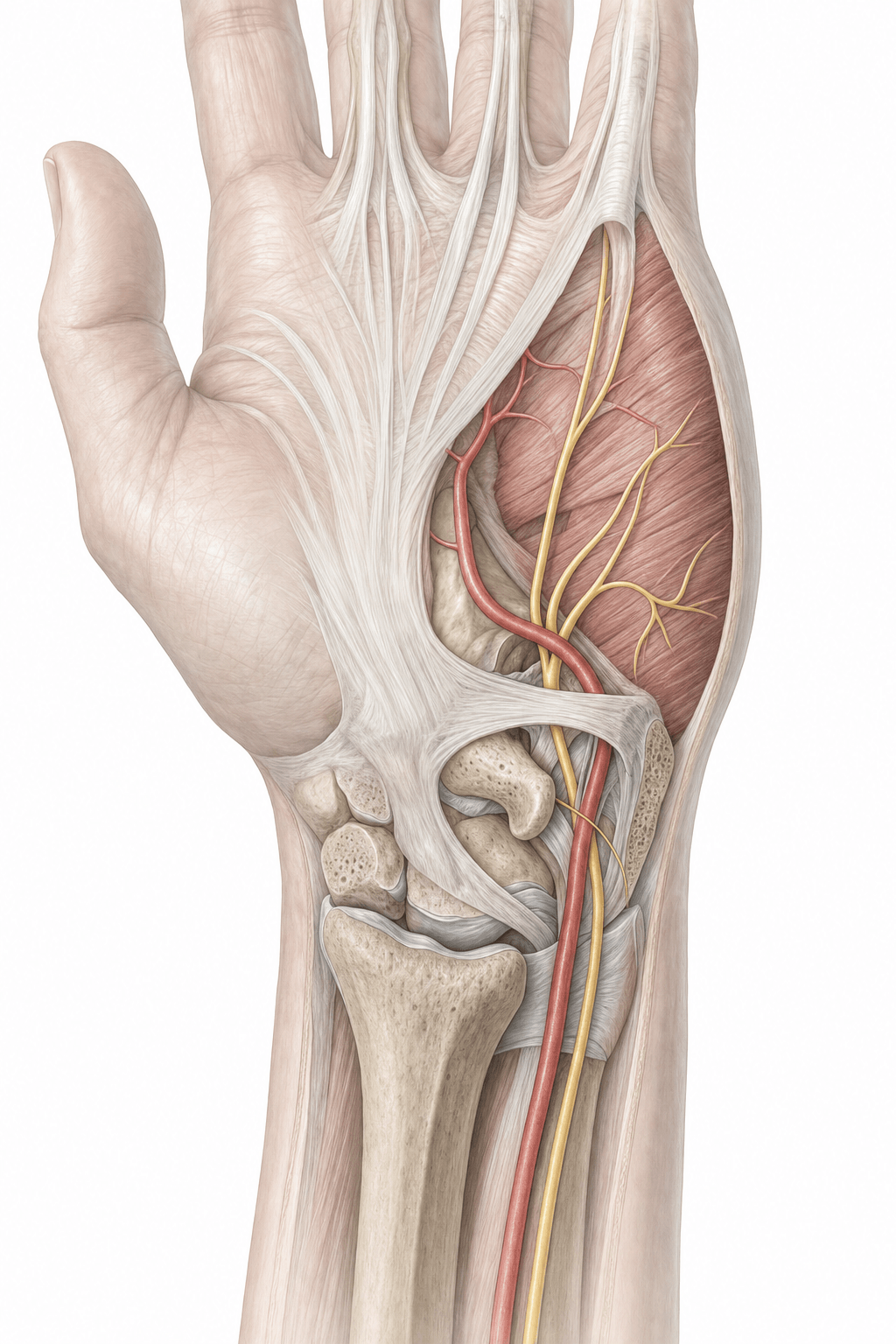
The ulnar artery and nerve enter the hand through Guyon's canal. Beyond the canal the ulnar artery passes superficial to the hook of the hamate before becoming the dominant contributor to the superficial palmar arch — here it is poorly protected, covered only by skin, fat and palmaris brevis. Repetitive blunt trauma — pushing, pounding, twisting or vibration transmitted through the hypothenar eminence — crushes the artery against the rigid hook of hamate, damaging the intima and media and leading to thrombosis, aneurysmal degeneration, or both. Mural thrombus then embolises distally into the digital arteries, producing the ischaemic fingertips. Underlying arterial-wall fragility (and the strong association with smoking) is thought to predispose susceptible individuals.
Predominantly men in manual occupations using the heel of the hand as a tool — mechanics, carpenters, metalworkers, machinists, stonemasons — plus vibrating-tool users and certain athletes (martial arts, baseball, mountain biking, handball, volleyball). Typically unilateral, affecting the dominant hand. A recognised occupational disease.
The injured ulnar artery feeds the superficial palmar arch and thus the ulnar digits (ring, little, often middle), so thrombosis and emboli produce ulnar-sided ischaemia, while the thumb and index (radial artery / deep arch) are usually spared — a useful localising clue.
Why arch completeness decides the operation
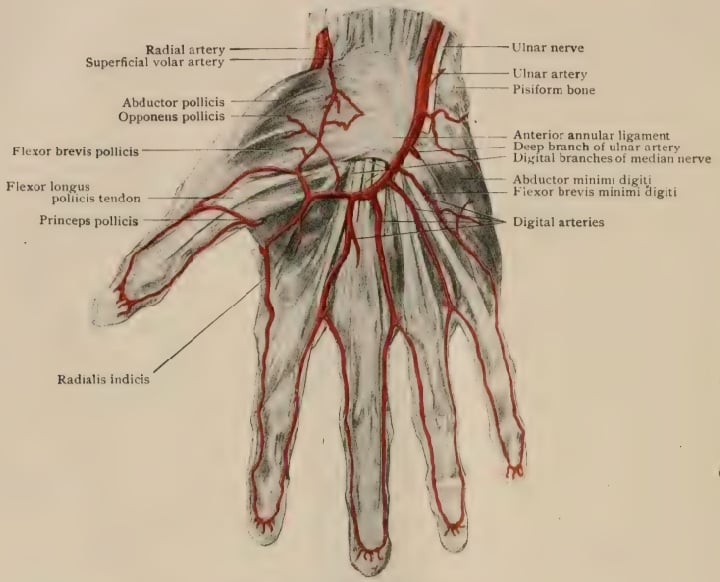
The whole ligate-versus-reconstruct decision rests on an anatomical fact worth stating explicitly, because examiners ask for it. The hand is supplied by two interconnected arches. The superficial palmar arch lies distally, is formed predominantly by the ulnar artery and completed by the superficial palmar branch of the radial, and gives off the common digital arteries. The deep palmar arch lies more proximally, is formed predominantly by the radial artery and completed by the deep branch of the ulnar. Where the two systems anastomose freely, the radial system can take over the ulnar territory, and a diseased ulnar segment can simply be resected and ligated.
In a significant minority of hands the superficial arch is incomplete — the radial and ulnar contributions do not connect — leaving the ulnar artery as the effective sole supply to the ulnar digits. Ligating it in that hand produces the ischaemia the operation was meant to prevent. This is why a normal radial-side Allen's test is not a formality but the permission slip for ligation, and why arch completeness and digital filling should be confirmed on imaging before committing, given how operator-dependent the bedside test is.
Clinical presentation
- Cold intolerance and colour change (pallor/cyanosis) of the ulnar digits
- Pain, paraesthesiae and digital ischaemia (ring/little ± middle finger)
- A tender, sometimes pulsatile hypothenar mass (aneurysm)
- Splinter haemorrhages / fingertip ulceration or necrosis from emboli in severe cases
- Thumb usually spared (radial supply) — a key discriminator
- Allen's test: delayed or absent refill on releasing the ulnar artery indicates ulnar inflow compromise
- Hypothenar tenderness and a possible palpable/pulsatile mass
- Digital pressure / capillary refill asymmetry favouring the ulnar digits
- Look for a manual occupation/sport and smoking history
Consider other causes of digital ischaemia and a hypothenar mass: Raynaud's phenomenon / connective-tissue disease (usually bilateral, symmetrical, thumb involved), Buerger's disease (thromboangiitis obliterans), atherosclerotic/embolic disease from a proximal source, vasculitis, a ganglion or giant cell tumour of the tendon sheath (mass but no ischaemia), and ulnar nerve compression at Guyon's canal (neurological, not ischaemic). The unilateral, dominant-hand, ulnar-digit, thumb-sparing pattern with an occupational history points to HHS.
The other vascular condition of the manual worker is hand-arm vibration syndrome (HAVS) — distinct from HHS, frequently examined alongside it, and able to co-exist in the same patient.
- Cause: chronic hand-transmitted vibration from power tools (grinders, chainsaws, jackhammers, polishers) — not a single localised arterial crush.
- Three components: a vascular component (episodic, cold-induced finger blanching — "vibration white finger", a secondary Raynaud's phenomenon from digital-artery vasospasm/wall thickening); a sensorineural component (numbness, tingling, reduced dexterity and grip); and a musculoskeletal component.
- Pattern that separates it from HHS: HAVS is typically bilateral, affects multiple fingers of the vibration-exposed hand(s), is episodic and vasospastic (provoked by cold), and carries a sensorineural deficit. HHS is unilateral, ulnar-localised, a structural ulnar-artery lesion (thrombosis/aneurysm with distal emboli), and is not primarily vasospastic.
- Grading: severity is staged by the Stockholm Workshop scale, which scores the vascular and sensorineural components separately.
- Status & management: a recognised prescribed/notifiable occupational disease in many jurisdictions; management is reduce vibration exposure, keep the hands warm, stop smoking, and treat vasospasm — overlapping with, but not the same as, the HHS pathway.
Investigations
- Allen's test at the bedside (screening).
- Duplex ultrasonography — shows ulnar artery occlusion, aneurysm and flow; first-line imaging.
- Acral plethysmography / digital pressures — quantify distal perfusion.
- Screen for vasospastic/connective-tissue disease where the picture is atypical (autoimmune serology).
- Elevate the hand and ask the patient to clench the fist firmly several times to exsanguinate the palm.
- The examiner occludes BOTH the radial and ulnar arteries at the wrist with firm thumb pressure.
- The patient opens the hand — the palm is pale. Avoid forced wide-spreading/hyperextension of the fingers, which can produce a false pallor.
- Release ONE artery and time the return of colour: brisk refill (about 5 to 7 seconds) means that vessel is patent and supplies the palm; delayed or absent refill (e.g. beyond about 10 to 15 seconds) indicates inflow compromise through that vessel.
- In HHS: releasing the ulnar artery shows delayed/absent ulnar refill — the lesion. Before ligation, release the radial artery to confirm the radial artery/deep arch alone adequately supplies the whole hand (good collateral) — this is exactly what justifies simple ligation rather than reconstruction.
- The digital Allen's test assesses the two proper digital arteries of a single finger (occlude both at the finger base, blanch the pulp, release one and watch refill).
- Caveat: Allen's test is operator-dependent with imperfect reliability — confirm with duplex/angiography before acting on it.
Management
Several principles apply to every patient regardless of the definitive strategy: remove/modify the repetitive trauma (occupational change, padded gloves, tool redesign), hand protection, and smoking cessation. Beyond these, the optimal treatment — especially the indication for surgery — remains controversial because the evidence is limited to case series with no randomised trials.
- 1Universal basics for everyoneStop/modify the repetitive trauma (job, tools, padded gloves), hand protection, and smoking cessation — without these, recurrence is likely whatever else is done.
- 2Medical therapyVasodilators (e.g. calcium-channel blockers) and antiplatelet/anticoagulation to limit thrombus propagation and embolisation; catheter-directed thrombolysis in selected acute presentations; sympathetic modulation for vasospasm.
- 3Operate for aneurysm / embolisation / critical ischaemiaResection of the diseased segment removes the embolic source. Choose ligation vs reconstruction by collateral supply and distal targets.
- 4Ligate or reconstructResection + LIGATION when radial/collateral supply is adequate (normal Allen's to the radial side). Resection + INTERPOSITION GRAFT (reversed vein or arterial) when collateral flow is insufficient and distal targets are good; ± periarterial sympathectomy.
Suitable for many patients, particularly those without ongoing embolisation or critical ischaemia: hand protection and avoidance of the causative trauma; smoking cessation; vasodilators and antiplatelet/anticoagulation; catheter-directed thrombolysis in selected acute presentations; and sympathetic modulation (botulinum toxin / sympathetic block) for vasospasm.
Early diagnosis allows more effective treatment and helps prevent long-term sequelae. The single most important durable measures are eliminating the repetitive trauma and smoking cessation — without these, recurrence is likely whatever the index treatment. Complications include progressive ulceration/necrosis, recurrent embolisation, and after surgery, graft thrombosis (needs good distal runoff) or recurrence if trauma/smoking continue.
Complications
- Complication
- Digital ischaemia, ulceration and tip necrosis
- Note
- From ongoing embolisation into the ulnar digital arteries; can need amputative debridement
- Complication
- Recurrent embolisation / vasospasm + cold intolerance
- Note
- Persistent symptoms if the embolic source (aneurysm/thrombus) and trauma continue
- Complication
- Ulnar sensory nerve irritation
- Note
- The adjacent ulnar nerve in Guyon's canal can be involved
- Complication
- Graft thrombosis
- Note
- Interposition grafts fail without good distal runoff - check the targets first
- Complication
- Recurrence (~28%)
- Note
- Likely if the repetitive trauma and smoking are not stopped (median recurrence ~11 months)
The treatment fails if the trauma and smoking continue. Whatever the index procedure (medical, ligation or graft), recurrence is common (~28%) unless the occupational/recreational trauma is eliminated and the patient stops smoking - so make these non-negotiable and follow the patient up.
True, False and Digital Artery Aneurysms of the Hand
HHS is the commonest reason to meet an arterial aneurysm in the hand, but the examiner may widen the question, and the distinction between aneurysm types changes both the history you take and the operation you plan.
- Wall
- ALL layers of the wall, dilated but intact
- Typical cause
- Repetitive blunt trauma over the hook of hamate, on a possibly fibrodysplastic artery
- Implication
- Mural thrombus is an ongoing embolic source - resect it
- Wall
- Wall BREACHED; contained by surrounding tissue and haematoma
- Typical cause
- PENETRATING injury - laceration, stab, iatrogenic puncture or cannulation
- Implication
- Expanding, can rupture; the history is a single sharp injury, not years of pounding
- Wall
- Either, at the proper or common digital artery
- Typical cause
- Local trauma or repetitive injury to a single digit
- Implication
- A small pulsatile digital mass; the digital Allen's test assesses the two proper digital arteries
The practical points are these. A false aneurysm follows a penetrating injury, so a history of a single laceration, stab or arterial puncture rather than years of palmar pounding should shift the diagnosis away from HHS - though both thrombose and embolise distally, so the presentation can look identical. A digital artery aneurysm presents as a small pulsatile mass in the finger, and the relevant bedside test is the digital Allen's test on that finger's two proper digital arteries rather than the wrist-level test. And the one-liner worth keeping: the ulnar artery at the wrist is the commonest site of an upper-limb arterial aneurysm.
Mnemonics & Memory Aids
- Mechanism: repetitive blunt trauma to the ulnar artery over the hook of hamate (hand = hammer, hook = anvil) → thrombosis ± aneurysm with distal emboli.
- Pattern: unilateral, dominant-hand, ulnar-digit ischaemia (ring/little ± middle); thumb spared (radial supply); manual-working man; smoking-associated.
- The ulnar artery at the wrist is the commonest site of upper-limb arterial aneurysm.
- Allen's test + duplex; angiography is the reference standard (corkscrew sign, occlusion, aneurysm).
- Universal basics: stop the trauma + smoking cessation.
- Surgery for aneurysm/embolisation/critical ischaemia: resect + ligate (good collaterals) or interposition graft (poor collaterals / good distal targets).
HAMMERThe syndrome
Hook:The hand is the HAMMER, the hook of hamate the anvil - and the ulnar artery pays the price.
ULNAREverything is ulnar
Hook:ULNAR everything: ulnar artery, ulnar digits, ulnar-sided ischaemia.
GRAFTLigate or reconstruct?
Hook:GRAFT decision: ligate if collaterals are Good, reconstruct if not - and always stop the trauma and smoking.
Evidence Base
Hypothenar hammer syndrome
- HHS should be considered in hand ischaemia among people who use the hypothenar region occupationally/recreationally as a 'hammer'.
- Routine diagnostics: physical examination including Allen's test, acral plethysmography and duplex sonography; angiography remains the gold-standard test for diagnosis.
- Basic principles apply to all patients - hand protection and smoking cessation; optimal treatment and the indication for surgery remain controversial due to a lack of sound data (no randomised trials).
Current options for treatment of hypothenar hammer syndrome
- A rare vascular condition from injury to the ulnar artery at Guyon's canal; the ulnar artery at the wrist is the most common site of upper-extremity arterial aneurysm and is particularly prone to injury.
- Signs/symptoms include a palpable mass, distal digital embolisation (long/ring/small fingers), pain, cyanosis, pallor, coolness and recurrent vasospasm.
- Diagnosis and surgical planning use duplex, contrast arteriography and CT angiography; management spans medical, non-operative and operative options.
Hypothenar hammer syndrome: proposed etiology
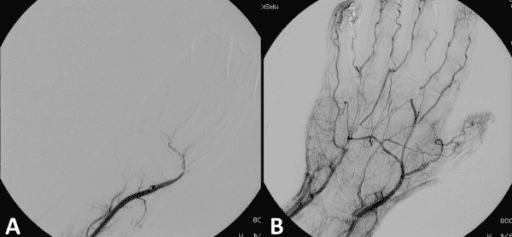
- 21 men with HHS, all with occupational/avocational repetitive palmar trauma; segmental ulnar occlusion or the characteristic 'corkscrew' elongation with alternating stenoses/ectasia on arteriography.
- Bilateral arteriographic abnormalities were present in 12 of 13 (92%) bilateral studies despite UNILATERAL symptoms; histology was compatible with fibromuscular dysplasia plus superimposed trauma.
- Vein-graft patency was 84% at 2 years; the authors propose HHS occurs when intrinsically abnormal (fibrodysplastic) ulnar arteries meet repetitive trauma.
Long-term follow-up of hypothenar hammer syndrome: a series of 47 patients
- 47 patients (1.13% of Raynaud-phenomenon referrals); 91.5% had occupational repetitive palmar trauma (mean exposure ~21 years); 87.2% unilateral, 93% dominant hand.
- Angiography: ulnar occlusion 59.6%, ulnar aneurysm 40.4%, multiple digital-artery emboli 57.4%; most managed conservatively (vasodilators, antiplatelets, risk-factor control) with favourable outcomes.
- HHS recurred in 27.7% (median 11 months), so close follow-up and elimination of the trauma are essential.
Coil embolisation with isolation technique of an ulnar artery aneurysm in hypothenar hammer syndrome
- Imaging showed a 15 mm ulnar artery aneurysm with the characteristic corkscrew deformity.
- Coil embolisation using an isolation technique achieved complete aneurysm occlusion while maintaining flow to all digits through collateral circulation from the radial artery via the palmar arch.
- Pre-procedural confirmation of adequate collateral circulation (selective compression on digital subtraction angiography) is essential before endovascular treatment.
The diagnostic pathway and the no-randomised-data caveat come from Schröttle et al. 2015 (DOI); the aneurysm/treatment-options detail from Hui-Chou & McClinton 2014 (DOI); the fibrodysplasia aetiology and bilateral-abnormality finding from Ferris et al. 2000 (DOI); the endovascular isolation technique and its collateral-circulation precondition from Yukimoto et al. 2025 (DOI); and the long-term/recurrence data from Marie et al. 2007 (DOI). The evidence base is limited to reviews and case series (Level IV-V) with no randomised trials, which is why the indication for and type of surgery remain debated.