Dorsal Wrist Overuse Tenosynovitis | 1st Crosses 2nd Compartment | Crepitus and Squeak | Proximal vs Distal
- Friction tenosynovitis where 1st compartment (APL, EPB) crosses over 2nd (ECRL, ECRB)
- Pain and swelling 4-6 cm PROXIMAL to the wrist - not over the radial styloid
- Classic crepitus or audible squeak ('wet leather' sign)
- Key differential is de Quervain (which is at the radial styloid)
- Treatment is conservative - rest, splint, NSAIDs, then injection if needed
- “Proximal intersection is more proximal than de Quervain
- “Rowers, weightlifters, racquet sports, skiers
- “Distal intersection = EPL crossing the radial wrist extensors
- “Surgery is rarely needed
- “Asymptomatic peritendinous fluid is common in elite rowers
Pain and swelling sit 4-6 cm PROXIMAL to the wrist, over the dorsoradial forearm. This is the single best way to separate it from de Quervain, where pain is directly over the radial styloid.
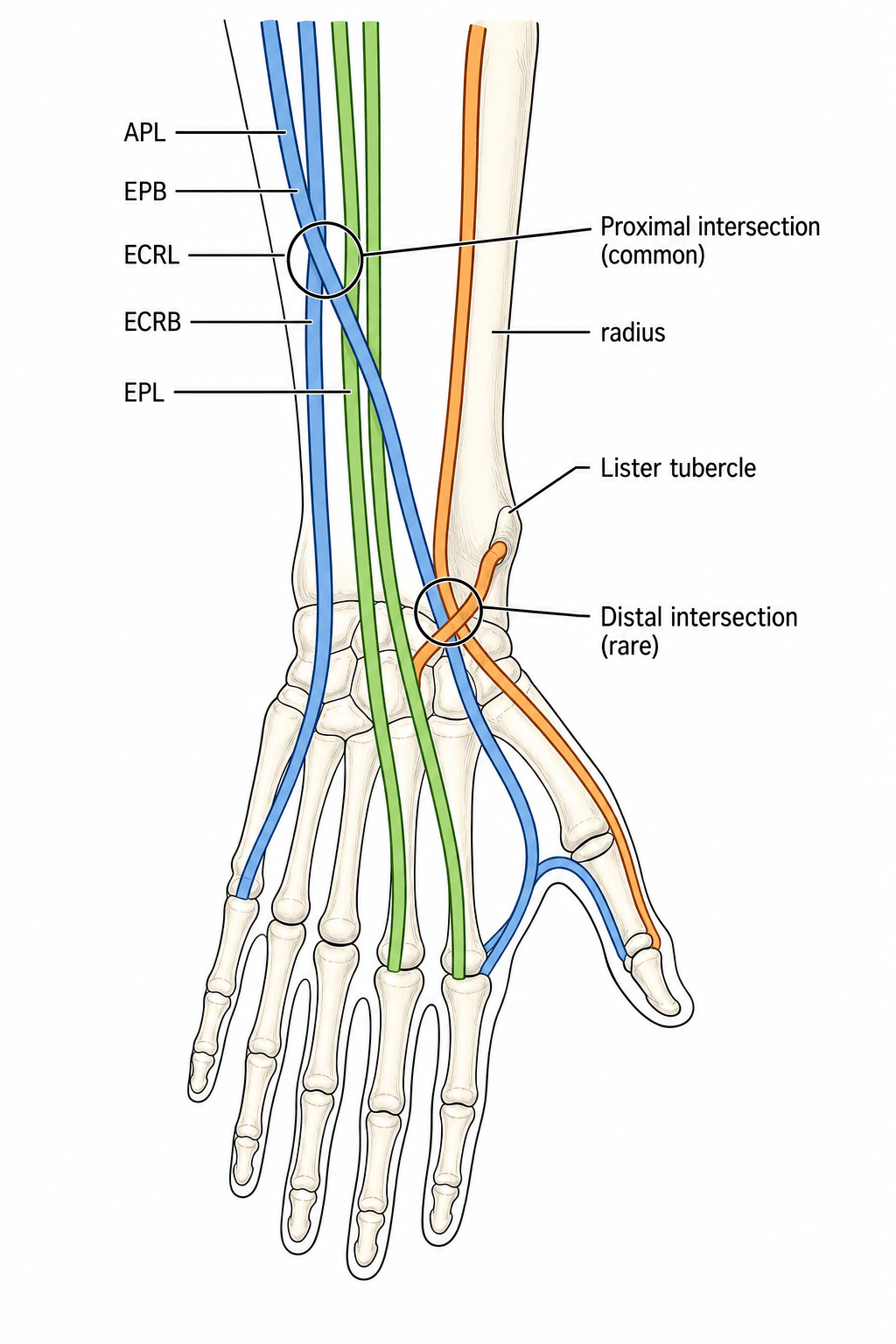
Proximal intersection syndrome occurs where the first compartment (APL and EPB) crosses superficially over the second compartment (ECRL and ECRB). Friction here produces a tenosynovitis.
Crepitus, and sometimes an audible squeak ("wet leather" sign), can be felt or heard over the area on wrist movement. It is a classic clinical clue.
Rest, activity modification, thumb spica splint and NSAIDs settle most cases. A corticosteroid injection is reserved for failure; surgery is rarely required.
PROXIMALIntersection vs De Quervain
Hook:Intersection is PROXIMAL - de Quervain is at the styloid!
1 over 2Tendons That Cross
Hook:The mobile thumb tendons rub OVER the radial wrist extensors.
1-2-3-4-5-6Dorsal Compartments (for orientation)
Hook:Compartment 1 crosses 2 proximally; compartment 3 crosses 2 distally.
Overview and Epidemiology
Intersection syndrome is an overuse tenosynovitis of the dorsal wrist caused by friction where the muscle bellies and tendons of the first dorsal extensor compartment (abductor pollicis longus, APL, and extensor pollicis brevis, EPB) cross superficially over the tendons of the second compartment (extensor carpi radialis longus, ECRL, and extensor carpi radialis brevis, ECRB). This crossing point lies in the dorsoradial distal forearm, roughly 4 to 6 cm proximal to the wrist joint (proximal to Lister tubercle) - clearly more proximal than de Quervain disease, which sits at the radial styloid.
It is uncommon. According to PubMed, a review of more than a thousand hand and wrist ultrasound examinations found intersection syndrome in only about 1.9 percent of patients evaluated in a specialised setting. It is best regarded as a repetitive-strain condition of the active and the athletic rather than a degenerative disease of older patients.
- Typically active adults, mean age around the fourth to fifth decade
- Reported with a male predominance in imaging series
- Rowers are the classic athletes (it is sometimes called "oarsman's wrist")
- Also weightlifters, racquet-sport players, skiers, horse riders, and occupations with repetitive wrist extension
- Repetitive resisted wrist extension and radial deviation
- Sudden increase in training load or new activity
- Sports involving a strong, repeated wrist-extension stroke (rowing, weight training)
- Repetitive occupational tasks (e.g. racquet sports, manual repetitive work)
The classic patient is a rower or weightlifter with dorsoradial forearm pain a few centimetres proximal to the wrist, plus crepitus or a squeak on moving the wrist. Note that peritendinous fluid in these tendons is common even in asymptomatic elite rowers, so imaging findings must be matched to symptoms.
Pathophysiology and Anatomy
Proximal Intersection
The first compartment muscle bellies and tendons (APL, EPB) pass obliquely over the second compartment tendons (ECRL, ECRB) about 4-6 cm proximal to the wrist.
Repetitive wrist extension makes the two tendon groups rub against each other. This produces a friction tenosynovitis with peritendinous oedema and fluid.
Two mechanisms are described - friction/abrasion between the crossing tendons, and a stenosing tenosynovitis of the second compartment as it runs deep to the first. Both result in the same clinical picture.
Classification
Proximal vs Distal
- Crossing tendons
- 1st (APL, EPB) over 2nd (ECRL, ECRB)
- Location
- 4-6 cm proximal to wrist
- Frequency
- Common (classic)
- Crossing tendons
- 3rd (EPL) over 2nd (ECRL, ECRB)
- Location
- At Lister tubercle
- Frequency
- Rare
When the exam says "intersection syndrome" without qualification, it means the proximal type (first crossing second). Mention the distal variant to score extra marks.
Clinical Assessment
- Dorsoradial forearm pain, 4-6 cm proximal to the wrist
- Worse with wrist extension and gripping
- A rubbing, squeaking or grating sensation on wrist movement
- Recent increase in training or repetitive activity
- Occupation or sport involving repeated wrist extension
Always ask about a change in load or a new activity.
- Tenderness and swelling over the intersection point (proximal to the radial styloid)
- Palpable crepitus on active wrist flexion/extension - the "wet leather" sign
- Sometimes localised erythema and warmth
- Pain reproduced by resisted wrist extension
- Finkelstein/Eichhoff may be mildly uncomfortable but pain is more proximal than in de Quervain
Locate the point of maximal tenderness carefully - it is the key to the diagnosis.
Site of maximal tenderness is everything. Intersection syndrome is proximal to the radial styloid (in the distal forearm); de Quervain is directly over the radial styloid at the first compartment. If you remember one thing, remember the location.
Investigations
Primarily Clinical
Intersection syndrome is largely a clinical diagnosis based on the site of pain and crepitus 4-6 cm proximal to the wrist.
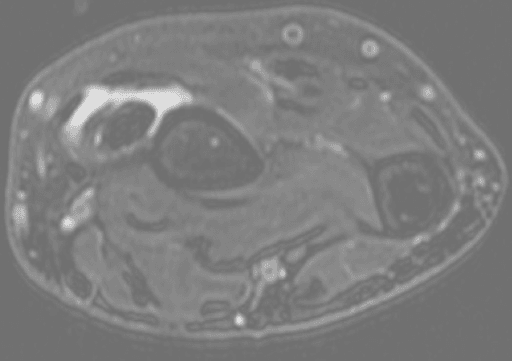
Imaging is used to confirm equivocal cases and to exclude alternatives (de Quervain, radial bone stress, compartment syndrome), not as a routine first step.
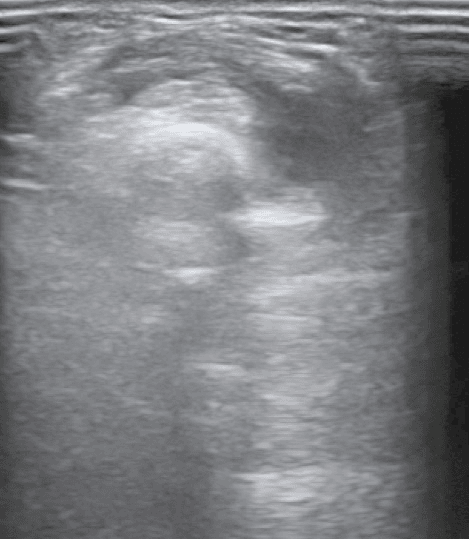
Asymptomatic peritendinous fluid around the radial wrist extensors is common in elite rowers. A positive ultrasound or MRI does not make the diagnosis on its own - it must match localised symptoms and signs.
Differential Diagnosis
- Distinguishing features
- Pain, swelling and crepitus 4-6 cm proximal to the wrist
- Discriminating clue
- Tenderness proximal to the radial styloid; wet-leather squeak
- Distinguishing features
- Pain and tenderness directly over the radial styloid
- Discriminating clue
- Positive Finkelstein/Eichhoff; tenderness at the styloid, not proximal
- Distinguishing features
- Dorsoradial numbness and paraesthesia, no true tendon swelling
- Discriminating clue
- Positive Tinel over the nerve; sensory rather than tendon-stretch pain
- Distinguishing features
- EPL crossing the radial wrist extensors at Lister tubercle
- Discriminating clue
- Pain at Lister tubercle; consider attrition/rupture risk of EPL
- Distinguishing features
- Pain at the thumb base or just distal to the scaphoid
- Discriminating clue
- Grind test; radiographs show joint OA, pain is distal not proximal
- Distinguishing features
- Diffuse exertional forearm pain in endurance athletes
- Discriminating clue
- Pain is diffuse and load-dependent, no localised crepitus
The examiner almost always wants you to contrast intersection syndrome with de Quervain. Lead with location (proximal forearm vs radial styloid), then the crossing tendons (1st over 2nd), then the crepitus sign. Mention Wartenberg syndrome to show breadth.
Management
First-Line (almost everyone)
- Stop or modify the provoking activity
- Correct technique and training-load errors
- Thumb spica or wrist (cock-up) splint with the wrist in slight extension for 2-3 weeks
- NSAIDs and ice for the inflammatory phase
- After 2-3 weeks, progressive stretching and graded strengthening before return to sport
Most patients settle with this approach.
Rest, splint in slight wrist extension, NSAIDs, then progressive rehab; corticosteroid injection (ideally ultrasound-guided) if it fails; surgical second-compartment release only for the rare refractory case.
Return to Sport: Load Management and Technique Correction
The topic repeatedly says to "correct technique and training-load errors" and warns that recurrence is common "if load is not corrected" — but the actual load and technique factors are what stop the "oarsman's wrist" coming back.
- The load spike is the cause. Intersection syndrome typically follows a sudden increase in volume or intensity — a pre-season ramp-up, a new training block, or a change of equipment. Recovery without addressing this simply sets up recurrence.
- Graded return, not calendar-based. After the initial 2-3 week rest/splint phase, progress through pain-free wrist-extension range, then graded loading, then sport-specific drills, advancing only while symptom-free and crepitus-free; a flare means dropping back a stage.
- Rowing-specific correction ("oarsman's wrist"). Address the feathering/squaring action that repeatedly loads wrist extension and radial deviation: coach a more neutral wrist through the drive and feather, review oar-handle size and grip and rigging (gearing, oar length, blade pitch), and discourage over-gripping. Cold, wet conditions and blistered hands worsen the grip and the friction.
- Other sports and occupations. Weightlifters: review wrist position and wrist-wrap use in pressing and curling; racquet sports: grip size and stroke mechanics; manual workers: tool ergonomics and task rotation.
- Periodise the load. Reintroduce training volume incrementally and monitor symptoms — the same load-management logic that prevents radial bone stress and forearm compartment syndrome in this rowing population (conditions studied alongside intersection syndrome in the imaging literature) applies here.
Q: How do you stop intersection syndrome recurring when an athlete returns to sport? A: Treat the load spike and technique, not just the tendons: a graded, symptom-guided return (range → load → sport-specific), correction of the wrist-extension mechanics (for rowers, a neutral wrist through the feather, plus grip/rigging review), and incremental load periodisation. Recurrence is common precisely when training load and technique are not addressed.
Complications
- Frequency
- Common if load not corrected
- Prevention / Management
- Graded return, technique and training-load review
- Frequency
- Uncommon
- Prevention / Management
- Injection, structured rehab, occasionally surgery
- Frequency
- Surgical risk
- Prevention / Management
- Careful dissection and nerve protection
- Frequency
- Rare
- Prevention / Management
- Recognise distal intersection; monitor EPL
- Frequency
- Possible
- Prevention / Management
- Counsel patient; avoid superficial injection
Outcomes and Prognosis
Prognosis
The outlook is generally excellent. Most patients recover fully with conservative treatment over a few weeks once the provoking load is removed.
early diagnosis, correction of the offending activity, structured graded return.
continued overload without rest, delayed diagnosis (often mislabelled de Quervain), and failure to address sporting technique.
Clinical Relevance and Exam Focus
It is the perfect "not de Quervain" trap. A candidate who reflexively says de Quervain for any radial wrist pain falls into it. The discriminator is the proximal location and the crepitus/squeak.
Know the six dorsal compartments, that 1 crosses 2 proximally and 3 crosses 2 distally (at Lister tubercle), and that the superficial radial nerve is at risk in surgery.
The rower/weightlifter story and the fact that asymptomatic fluid is common in elite rowers are favourite sports-medicine talking points.
Conservative first, ultrasound-guided injection second, surgery a distant last. Stating this ladder confidently signals a sensible clinician.
Guidelines, Registries & Global Practice
- Intersection syndrome is uncommon; an imaging series found it in about 1.9 percent of patients undergoing hand and wrist ultrasound in a specialised setting, with a mean age around 45 and a male predominance.
- It is concentrated in athletes and manual workers performing repetitive resisted wrist extension - rowers ("oarsman's wrist"), weightlifters, racquet-sport players and skiers feature repeatedly across reports worldwide.
- Asymptomatic peritendinous fluid around the radial wrist extensors is common in elite rowers, so the true symptomatic prevalence in athletic populations is hard to define.
No orthopaedic society publishes a dedicated, named intersection-syndrome guideline, so practice is anchored by reviews and primary-care guidance rather than a formal guideline document.
- Position
- Rest, thumb spica splint, NSAIDs, then progressive rehab; injection for persistence; surgery if refractory
- Notes
- Most cited treatment ladder for the condition
- Position
- Conservative care first; ultrasound-guided glucocorticoid injection for non-responders
- Notes
- Contemporary primary-care framing
- Position
- Stepwise conservative-to-surgical management of dorsal compartment tenosynovitis
- Notes
- No condition-specific guideline; principles applied
- Position
- Conservative-first, decompression of second compartment reserved for refractory cases
- Notes
- Consistent with the above
Intersection syndrome is a soft-tissue overuse condition managed largely without surgery and is not captured by joint-replacement registries (NJR, AJRR, AOANJRR). Evidence therefore comes from imaging series, small case series and reviews rather than national implant registries.
- In well-resourced settings, ultrasound-guided injection is increasingly standard for non-responders, improving accuracy.
- In limited-resource settings the diagnosis remains clinical (proximal tenderness plus crepitus), and landmark-guided injection or simple conservative care is effective.
- Surgical release is rarely needed and, when performed, is a low-cost day-case procedure - so management is feasible across all resource levels.
Know that intersection syndrome is proximal forearm friction tenosynovitis (1st over 2nd compartment), distinguished from de Quervain by location and crepitus, managed conservatively first with ultrasound-guided injection for non-responders and surgery only for refractory disease.
Two Mechanisms, One Target: Why the Second Compartment Is Released
The pathophysiology above flags a "mechanism debate", and surgery "releases the second dorsal compartment" — a link worth making explicit, because the surgical target can seem counterintuitive.
- Mechanism 1 — friction/abrasion. The mobile first-compartment muscle bellies (APL, EPB) rub across the underlying second-compartment tendons during repetitive wrist extension, producing a peritendinous friction tenosynovitis at the crossing.
- Mechanism 2 — stenosing tenosynovitis of the second compartment. The second-compartment tendons (ECRL, ECRB) become constricted within their sheath as they run deep to the crossing first compartment — a stenosis analogous to de Quervain but one compartment over and more proximal.
- The unifying point. Whichever mechanism dominates, the symptomatic, constrained structure is the second compartment. That is why, although the first compartment is the crossing "aggressor", surgical treatment is decompression/release of the second dorsal compartment (fasciotomy of its sheath) with tenosynovectomy, freeing ECRL/ECRB — not release of the first compartment, which would be the de Quervain operation.
- Practical consequence. It also explains why the corticosteroid injection is placed into the second-compartment sheath / intercompartmental space at the intersection, not the first compartment: treat where the tendons are constrained, not merely where they cross.
Q: In intersection syndrome the first compartment crosses over the second — so why does surgery release the second compartment? A: Because whether the pathology is friction from the crossing first compartment or a stenosing tenosynovitis of the second compartment, the constrained, symptomatic structure is the second compartment (ECRL/ECRB). Surgery decompresses the second dorsal compartment with tenosynovectomy; releasing the first compartment is instead the operation for de Quervain. The injection targets the same second-compartment/intercompartmental space.
MCQ Practice Points
Q: Which tendons are involved in proximal intersection syndrome? A: The first compartment (APL and EPB) crossing over the second compartment (ECRL and ECRB).
Q: Where is the pain in intersection syndrome compared with de Quervain? A: About 4-6 cm proximal to the wrist (distal forearm), versus directly over the radial styloid in de Quervain.
Q: What is the classic clinical sign of intersection syndrome? A: Crepitus, often with an audible squeak ("wet leather" sign), over the crossing point on wrist movement.
Q: What is distal intersection syndrome? A: A rarer variant where the EPL (third compartment) crosses over the second compartment (ECRL, ECRB) at Lister tubercle.
Q: What is the first-line treatment for intersection syndrome? A: Conservative care - rest/activity modification, splinting in slight wrist extension, NSAIDs, then graded rehabilitation. Injection if it fails; surgery rarely.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old competitive rower presents with a 3-week history of dorsoradial forearm pain about 5 cm proximal to the wrist, with swelling and a squeaking sensation on moving the wrist. There is local crepitus. What is your diagnosis and how would you manage it?”
“An examiner asks you to compare intersection syndrome with de Quervain tenosynovitis. How do you tell them apart and why does it matter?”
“A 38-year-old manual worker has had intersection syndrome for 6 months despite rest, splinting, NSAIDs and one ultrasound-guided corticosteroid injection. He still has pain and crepitus. How would you proceed, and what are the surgical considerations?”
Anatomy
- 1st compartment (APL, EPB) crosses 2nd (ECRL, ECRB)
- Crossing point 4-6 cm proximal to wrist
- Distal variant: EPL crosses 2nd at Lister tubercle
- Superficial radial nerve at risk in surgery
Clinical
- Dorsoradial forearm pain proximal to styloid
- Crepitus / wet-leather squeak
- Rowers, weightlifters, racquet sports
- Worse with resisted wrist extension
Investigations
- Largely clinical diagnosis
- Ultrasound first-line: peritendinous fluid
- MRI for equivocal/refractory cases
- Caution: fluid common in asymptomatic rowers
Management
- Rest and activity modification
- Splint in slight wrist extension + NSAIDs
- Graded rehab before return to sport
- Ultrasound-guided injection if it fails
- Second-compartment release rarely needed
Differentials
- De Quervain (at the styloid)
- Wartenberg syndrome (sensory)
- Distal intersection (EPL)
- Radial bone stress / compartment syndrome
Key Points
- Location proximal = NOT de Quervain
- Crepitus is the classic sign
- Conservative care cures most
- Surgery is a rare last resort
Evidence Base and Key Studies
- Intersection syndrome is a rare sports overuse injury caused by friction at the crossing of the first and second dorsal compartments of the forearm
- Differential diagnosis from de Quervain tenosynovitis must be made carefully; clinical examination is central, with MRI and ultrasound as adjuncts
- First-line treatment is rest, thumb spica splinting, analgesia and oral NSAIDs, followed after 2-3 weeks by progressive stretching and strengthening
- Corticosteroid injection adjacent to the injury is useful for persistent symptoms; surgery is reserved for refractory cases
- Re-evaluation of 1,131 hand and wrist ultrasound reports identified 21 patients with intersection syndrome
- Intersection syndrome was found in about 1.9% of patients in a specialised hospital setting
- Mean age 45 years (range 22-60), with both proximal (more common) and distal forms identified
- Ultrasound is a non-invasive, simple and economical method to identify the syndrome, define tendon sheath anatomy and exclude other conditions
- Four patients with symptoms suggestive of intersection syndrome (pain, swelling, erythema, oedema of the wrist) were studied with ultrasound
- All four showed peritendinous oedema and synovial fluid within the tendon sheaths at the intersection of the first and second dorsal compartments
- The authors describe these as typical and reliable sonographic signs of the syndrome
- Ultrasound may eliminate the need for more expensive imaging tests
- 19 asymptomatic senior and under-23 elite rowers underwent ultrasound and MRI of the forearms
- Peritendinous fluid of ECRL (53%) or ECRB (32%) was a common finding on ultrasound
- MRI detected these changes at a higher rate than ultrasound
- Imaging findings seen in symptomatic populations were present in asymptomatic elite rowers, so caution is needed when diagnosing intersection syndrome on imaging alone
- A 26-year-old pregnant rower with dorsoradial wrist pain and a rubbing/squeaking sensation was initially treated as de Quervain
- Nine months of conservative de Quervain therapy and a landmark-guided corticosteroid injection failed
- In-clinic ultrasound showed tenosynovitis at the intersection of the first and second compartments, confirming intersection syndrome
- Ultrasound-guided saline hydrodissection of the intercompartmental space gave immediate relief and served as both a diagnostic and therapeutic tool
- Intersection syndrome is described as an overuse injury
- Management involves rest, activity adjustment, bracing, NSAIDs and physical or occupational therapy
- For symptoms not improved by these measures, an ultrasound-guided glucocorticoid injection may be administered
- Discussed alongside de Quervain and carpal tunnel as common injectable wrist conditions
- Three cases of distal intersection syndrome (DIS) between the second and third dorsal compartments, a rarer and more distal entity than the classic form
- Diagnosis was confirmed on MRI in all three patients
- Initial treatment was NSAIDs and immobilisation; one patient ultimately required surgical debridement and partial tenosynovectomy
- All patients improved and returned to baseline activity; the authors warn that extensor tendon rupture is possible