Glenoid fossa fracture classification by fracture-line exit direction through the scapula
- The Ideberg classification describes six patterns of glenoid fossa fracture based on the fracture line exit through the scapula, originally described by Ideberg in 1984 and refined in 1995. It is the most widely used system for intra-articular scapular fractures.
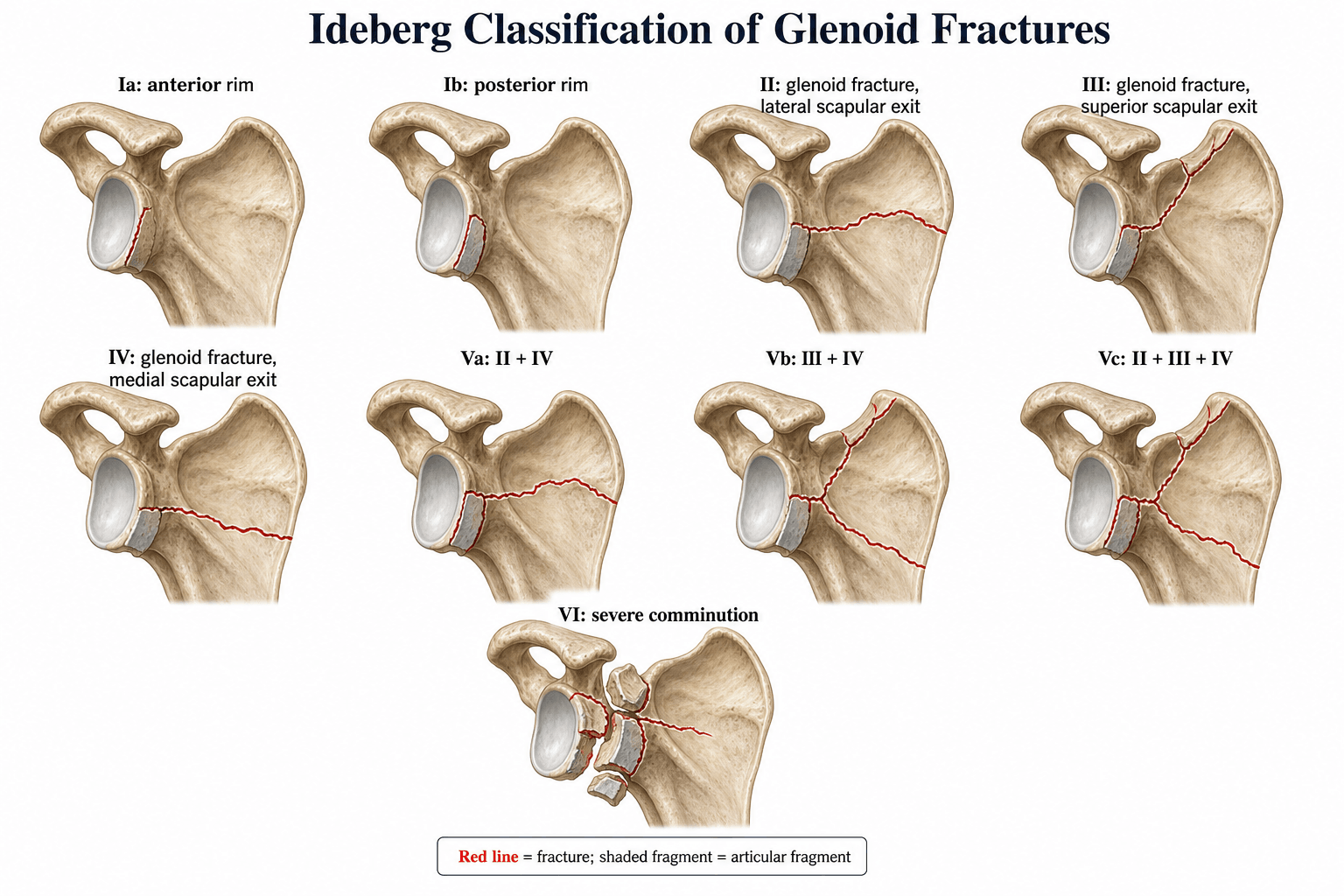
- Type I is a glenoid rim fracture (Ia anterior, Ib posterior) — essentially a bony Bankart or reverse bony Bankart variant. Types II through IV exit through the scapular body laterally, superiorly, or medially. Type V combines patterns, and Type VI is severe comminution.
- Operative fixation is indicated for displaced intra-articular fractures with greater than 2 mm articular step-off, glenohumeral instability, or a large rim fragment (typically greater than 20 percent of the glenoid arc). Non-operative management suits minimally displaced, stable patterns.
- These are high-energy injuries: up to 80 to 90 percent of patients have associated injuries — ribs, lung, clavicle, brachial plexus. Always complete a full trauma survey and do not be distracted by the scapular fracture from life-threatening thoraco-abdominal pathology.
- “Greater than 2 mm articular displacement or instability means operate
- “Type Ia/Ib: rim fractures — fix if greater than 20-25 percent of glenoid arc
- “Type IV exits medially (through scapular body) — posterior Judet approach
- “Always complete ATLS survey first — 80 to 90 percent have associated injuries
An intra-articular glenoid fracture with greater than 2 mm of articular displacement or glenohumeral instability is generally an indication for operative fixation. Type I rim fractures associated with shoulder dislocation need fixation if the fragment involves greater than 20 to 25 percent of the glenoid arc (risk of recurrent instability). For Types II through V, the goal is anatomic restoration of the joint surface with stable internal fixation to allow early mobilisation. Type VI (comminuted) may require arthroplasty if reconstruction is impossible.
The Ideberg Classification
The Ideberg classification categorises glenoid fossa fractures by the direction the fracture line exits the scapula. The mechanism differs by type and this drives both the fracture pattern and the associated soft-tissue injuries.
- Fracture Pattern
- Anterior glenoid rim
- Mechanism
- Shoulder dislocation (anterior)
- Key Feature
- Bony Bankart equivalent — anterior inferior glenoid rim avulsed with labrum and capsule
- Fracture Pattern
- Posterior glenoid rim
- Mechanism
- Shoulder dislocation (posterior) or direct posterior force
- Key Feature
- Reverse bony Bankart — posterior rim fragment with posterior capsulolabral complex
- Fracture Pattern
- Transverse fracture through glenoid fossa exiting laterally through the lateral scapular border
- Mechanism
- Axial load through humeral head (fall on outstretched hand or direct lateral shoulder impact)
- Key Feature
- Inferior glenoid fragment displaced laterally with humeral head
- Fracture Pattern
- Transverse fracture through glenoid fossa exiting superiorly through the superior scapular angle
- Mechanism
- Axial load with superior shear component
- Key Feature
- Superior fragment may include coracoid; associated with acromioclavicular and coracoclavicular ligament disruption
- Fracture Pattern
- Transverse fracture through glenoid fossa exiting medially through the scapular body (spine of scapula)
- Mechanism
- Axial load with strong medial vector
- Key Feature
- Fracture crosses the scapular spine; medial displacement of the glenoid fragment; often high-energy
- Fracture Pattern
- Combination of II and IV
- Mechanism
- Severe axial load with lateral and medial components
- Key Feature
- Lateral and medial exits — inferior and medial fragments
- Fracture Pattern
- Combination of III and IV
- Mechanism
- Severe axial load with superior and medial components
- Key Feature
- Superior and medial exits — superior and medial fragments
- Fracture Pattern
- Combination of II, III, and IV
- Mechanism
- Extreme violence
- Key Feature
- Three exits — inferior, superior, and medial fragments; very unstable
- Fracture Pattern
- Severe comminution of the glenoid fossa
- Mechanism
- Extreme high-energy crush or blast
- Key Feature
- No single identifiable fracture line; articular surface shattered — worst prognosis
Rim — Lateral — Superior — Medial — Combo — CrushThe six Ideberg types in order
Hook:RLSMCC: Rim Lateral Superior Medial Combo Crush — exit direction from simple to devastating
The key to remembering the Ideberg classification is the exit direction of the fracture line. Type II exits laterally (inferior fragment goes lateral). Type III exits superiorly (superior fragment includes coracoid region). Type IV exits medially (through the scapular body and spine). Type V combines these exit points. Type VI is comminuted beyond classification.
Clinical Presentation and Diagnosis
- Mechanism: These are overwhelmingly high-energy injuries — motor vehicle collisions, falls from height, pedestrian versus vehicle. A low-energy mechanism should prompt suspicion of a glenoid rim fracture (Type I) in the context of a shoulder dislocation rather than a true glenoid fossa fracture.
- Associated injuries are the rule, not the exception: ipsilateral rib fractures, pneumothorax or haemothorax, pulmonary contusion, clavicle fracture, brachial plexus injury, vascular injury (subclavian/axillary artery), and head injury are all common. Up to 80 to 90 percent of patients with a glenoid fossa fracture have at least one associated injury.
- Examination: localised posterior or lateral shoulder pain, swelling, and ecchymosis. The arm is typically held adducted and internally rotated. Palpate the entire shoulder girdle, clavicle, and chest wall. Perform a thorough neurovascular examination — particularly assess the axillary, suprascapular, musculocutaneous, and brachial plexus distributions.
- Imaging cascade:
- AP and axillary radiographs of the shoulder are the initial study but frequently underestimate the fracture. The axillary view is essential to assess glenohumeral alignment and anterior/posterior rim involvement.
- CT with 3D reconstruction is mandatory for all glenoid fossa fractures. It delineates the fracture pattern, degree of articular displacement, fragment size, and comminution. It is the study that determines the Ideberg type.
- MRI is useful for associated soft-tissue injuries (labral tears, rotator cuff, ligamentous disruption) but is not the primary classification tool.


AP — Axillary — CT 3D — Full Trauma SurveyEssential imaging work-up
Hook:AACT: AP Axillary CT Trauma-survey — never skip the CT for glenoid fractures
Management: Operative versus Non-operative
- Non-operative Criteria
- Fragment less than 20 percent of glenoid arc, no instability, no dislocation
- Operative Indications
- Greater than 20 to 25 percent of glenoid arc, glenohumeral instability, recurrent dislocation
- Typical Approach
- Arthroscopic or open reduction and internal fixation with suture anchors or mini-fragment screws; address labrum and capsule
- Non-operative Criteria
- Less than 2 mm displacement, stable glenohumeral joint, intact lateral column
- Operative Indications
- Greater than 2 mm articular step-off, glenohumeral subluxation, displaced inferior fragment
- Typical Approach
- Open reduction via deltopectoral or posterior approach; plate and screw fixation of the inferior glenoid fragment
- Non-operative Criteria
- Minimally displaced, coracoid and AC joint stable
- Operative Indications
- Displaced superior fragment, coracoid displacement, AC joint disruption
- Typical Approach
- Superior approach (supraspinatus split or deltoid-split); lag screw or plate fixation; address AC/coracoclavicular instability
- Non-operative Criteria
- Non-displaced transverse fracture, intact scapular body
- Operative Indications
- Medial displacement of glenoid fragment, articular incongruity, scapular spine disruption
- Typical Approach
- Posterior approach (Judet or modified Judet); plate fixation of glenoid to scapular body; may need dual approach
- Non-operative Criteria
- Rarely non-operative — most are displaced and unstable
- Operative Indications
- Almost always operative due to multi-fragment instability and articular incongruity
- Typical Approach
- Combined anterior and posterior approaches; plate and screw reconstruction; strategies tailored to the specific sub-type
- Non-operative Criteria
- Not reconstructible (definition)
- Operative Indications
- Attempted ORIF if any large articular fragments salvagable; otherwise consider arthroplasty
- Typical Approach
- Individualised — may require total shoulder arthroplasty or reverse total shoulder arthroplasty if the glenoid is beyond reconstruction
Beyond intra-articular step-off, scapular geometry on imaging guides operative decision-making, especially for fractures extending into the scapular neck and body:
- Glenopolar angle (GPA): the angle on a true AP (Grashey) view between a line along the longest axis of the glenoid and a line from the cranial-most point of the glenoid to the most caudal point of the scapular body. Normal is roughly 30 to 45 degrees; a GPA below about 20 to 22 degrees signifies significant angular deformity (the glenoid tilting caudally) and is a commonly cited operative indication for scapular neck/body fractures.
- Translation and angulation: widely quoted operative thresholds for displaced extra-articular scapular neck/body fractures include medial/lateral translation greater than about 2 cm and angulation greater than about 45 degrees (the Cole/Jones-type criteria), in addition to the greater than 2 mm intra-articular step-off used for the glenoid fossa itself.
- These measures matter in Ideberg Type II–V fractures where the glenoid fragment displaces relative to the scapular body; they complement — they do not replace — the assessment of glenohumeral stability and articular congruity.
Do not be distracted by the scapular fracture. These patients are multiply injured. Complete ATLS primary and secondary surveys. Life-threatening thoraco-abdominal injuries take precedence. The scapular fracture is often a marker of significant energy transfer and should prompt a thorough search for occult chest, abdominal, and neurovascular injuries.
The Superior Shoulder Suspensory Complex (SSSC)
Goss described the superior shoulder suspensory complex (SSSC) — a bone–soft-tissue ring suspending the upper limb from the axial skeleton. It is the conceptual key to shoulder-girdle injury patterns and explains why some scapular fractures are stable and others (such as the floating shoulder) are not.

- The ring: the glenoid process, the coracoid process, the coracoclavicular ligaments, the distal clavicle, the acromioclavicular joint, and the acromion.
- The two struts (links to the trunk): a superior strut — the middle third of the clavicle — and an inferior strut — the lateral border of the scapular body and the scapular spine.
- Single versus double disruption: a single break in the ring is usually stable and treated non-operatively. A double disruption (two breaks in the ring or its struts) destabilises the complex, allows the glenoid segment to displace under muscle pull and arm weight, and is a relative indication to stabilise at least one — often both — of the disruptions to restore the suspensory mechanism.
- The floating shoulder is the classic double disruption: an ipsilateral mid-clavicle fracture (superior strut) plus a scapular neck or glenoid fracture (the ring/inferior strut). Restoring the clavicle alone often realigns the glenoid by ligamentotaxis; some patterns need both fixed.
- Relevance to Ideberg: Type III fractures can disrupt the coracoid and the AC/coracoclavicular ligaments — several SSSC components in one injury; Types IV and V combined with a clavicle fracture create a floating shoulder. Recognising the double disruption converts an apparently isolated scapular fracture into an unstable girdle injury that may need fixation.
Surgical Approaches and Fixation Principles
The surgical approach is dictated by the Ideberg type and the location of the fracture fragments.
- Access
- Anterior glenoid, coracoid, superior glenoid
- Ideal For
- Type Ia, Type III
- Key Risks
- Cephalic vein, musculocutaneous nerve, axillary nerve (retraction)
- Access
- Posterior glenoid, scapular body, scapular spine
- Ideal For
- Type Ib, Type IV, Type V
- Key Risks
- Axillary nerve, suprascapular nerve and artery, circumflex scapular artery
- Access
- Full access to glenoid circumference and scapular body
- Ideal For
- Type V (complex), selected Type VI
- Key Risks
- Positioning challenges; prolonged operative time; increased blood loss
- Access
- Anterior and posterior rim, labrum, articular surface visualisation
- Ideal For
- Type Ia/Ib (rim fractures), assessment of articular reduction
- Key Risks
- Learning curve; limited ability to address comminuted or medially displaced fragments
Fixation principles:
- Anatomic reduction of the articular surface is paramount — any residual step-off greater than 2 mm increases the risk of post-traumatic glenohumeral arthritis.
- Use lag screws for simple fracture patterns and neutralisation or buttress plates for comminuted or vertically oriented fracture lines.
- For Type IV fractures with medial exit, restore the relationship between the glenoid fragment and the scapular body — this re-establishes the glenoid version and the medial-lateral column.
- In Type V variants, stabilise each exit point individually before linking them with a reconstructive plate across the scapular body.
- Type VI may not be reconstructible. If ORIF is attempted, the goal is containment of articular fragments. Definitive treatment may be delayed arthroplasty once the soft tissues have healed.
Lateral exit — Anterior. Superior exit — Anterior or Superior split. Medial exit — Posterior (Judet). Combined exits — Combined approaches.Approach selection by exit direction
Hook:LASM: Lateral=Anterior, Superior=Anterior/Split, Medial=Posterior — match approach to exit direction
Outcome and Complications
- Post-traumatic glenohumeral arthritis is the most significant long-term complication, particularly when articular reduction is imperfect. Studies report degenerative changes in a substantial proportion of patients followed beyond five years.
- Shoulder stiffness and loss of motion — prolonged immobilisation worsens this; stable internal fixation should allow early passive range of motion within the limits of the construct.
- Neurovascular injury — the suprascapular nerve is at risk during posterior approaches as it traverses the spinoglenoid notch. The axillary nerve is vulnerable during both anterior and posterior dissection. Pre-operative neurovascular assessment and intra-operative identification are essential.
- Non-union is uncommon but reported, particularly in Type IV and V fractures where the medial fragment loses its soft-tissue attachments. Rigid fixation and bone grafting of gaps may be required.
- Heterotopic ossification can occur after extensile approaches (Judet). Prophylaxis with indometacin or single-dose radiation is used in some centres for high-risk patients.
- Associated injuries dominate the early outcome — the scapular fracture itself may not be the limiting factor for functional recovery; concomitant brachial plexus injury, chest trauma, or head injury often determine the final result.
Limitations and Modern Context
- The Ideberg classification is anatomically descriptive but does not directly dictate treatment. The decision to operate rests on articular displacement, glenohumeral stability, fragment size, and patient factors — not the Ideberg type alone.
- Inter-observer reliability is moderate. Studies show better agreement for Type I (rim) and Type VI (comminuted) than for the intermediate types, particularly distinguishing Type II from Type IV and subtyping Type V. CT with 3D reconstruction improves agreement.
- The OTA/AO classification (14-F) and the Mayo classification are alternatives that some surgeons prefer for operative planning, but the Ideberg system remains the most frequently tested in fellowship examinations.
- Modern trends favour arthroscopic-assisted reduction for rim fractures (Type I), minimally invasive plate osteosynthesis for selected Type II and IV patterns, and reverse total shoulder arthroplasty for unreconstructible Type VI fractures in older patients.
- 3D printing and patient-specific instrumentation are increasingly used for pre-operative planning in complex Type V patterns, allowing surgeons to rehearse reduction strategies before entering the theatre.
Guidelines, Registries and Global Practice
- No single international guideline exists specifically for glenoid fossa fractures. Management is guided by expert consensus, institutional protocols, and the principles outlined above.
- AO Foundation principles emphasise anatomic articular reduction, stable fixation, and early mobilisation — these apply directly to Ideberg Type II through V fractures. The AO Trauma community provides online decision-making tools and surgical planning resources.
- Boehler's principle of restoring the articular surface underpins the operative threshold: greater than 2 mm displacement is the most widely cited cut-off, used across North American, European, and Australasian trauma centres.
- Registry data on scapular fractures specifically are sparse because these injuries are uncommon and captured within broader polytrauma registries. The German TraumaRegistry DGU and the NTDB (National Trauma Data Bank, US) record scapular fractures as part of polytrauma datasets, and their data consistently confirm the high-energy mechanism and high rate of associated injuries.
- Global practice variation: Some centres in Europe and North America favour more aggressive operative management of all displaced glenoid fractures, while some Asian and Australasian centres are more selective, operating only when instability or significant articular incongruity is demonstrated. Arthroscopic expertise is a key determinant — centres with established shoulder arthroscopy programmes treat more Type I fractures arthroscopically. Access to 3D CT reconstruction and modern mini-fragment fixation systems also influences operative rates.
- Reverse total shoulder arthroplasty for unreconstructible Type VI fractures is increasingly reported, particularly in older patients, following the same principles used for comminuted proximal humerus fractures where ORIF is not feasible.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 34-year-old man is involved in a high-speed motorcycle collision. He has a right pneumothorax (already drained), a clavicle fracture, and CT demonstrates a fracture line through the glenoid fossa exiting medially through the scapular body with approximately 4 mm of displacement of the glenoid fragment. Classify this fracture and outline your management plan.”
“A 28-year-old woman presents after a seizure with a posterior shoulder dislocation. Reduction is achieved, but the post-reduction CT shows a posterior glenoid rim fracture involving approximately 30 percent of the glenoid arc. How do you classify this injury and what is your management?”
The six types (by exit direction)
- Type I: Rim fracture — Ia anterior (bony Bankart), Ib posterior (reverse bony Bankart)
- Type II: Transverse glenoid, exits laterally through lateral scapular border
- Type III: Transverse glenoid, exits superiorly through superior scapular angle
- Type IV: Transverse glenoid, exits medially through scapular body (crosses scapular spine)
- Type V: Combination — Va (II plus IV), Vb (III plus IV), Vc (II plus III plus IV)
- Type VI: Severe comminution — unreconstructible; consider arthroplasty
Operative thresholds
- Articular step-off greater than 2 mm: fix (applies to all Types II through V)
- Rim fragment greater than 20 to 25 percent of glenoid arc: fix (Type I)
- Glenohumeral instability: fix regardless of fragment size
- Floating shoulder (clavicle plus scapular fracture): fix both to restore the superior suspensory complex
Approaches and pearls
- Anterior (deltopectoral): Type Ia, Type III
- Posterior (Judet): Type Ib, Type IV, Type V
- Combined: complex Type V patterns
- CT with 3D reconstruction is mandatory for classification and surgical planning
- Always complete ATLS survey first — associated injuries are the rule (80 to 90 percent)
Evidence Base
Epidemiology of scapular fractures: incidence and classification of 338 fractures
- Population series of 338 scapular fractures in 322 patients (two Swedish counties, 10 years); annual incidence about 10 per 100,000, of which 30 percent involved the glenoid cavity
- The most common intra-articular glenoid fracture was the anterior chip fragment, associated with a shoulder dislocation in roughly two-thirds of cases
- Provided the epidemiological underpinning for the Ideberg classification of intra-articular glenoid fractures (originally five types, later extended to six with the comminuted Type VI added by Goss)