When the Humeral Diaphysis Fails to Unite
- Humeral shaft nonunion is failure of the diaphysis to unite (no progressive healing, typically by around 6 months); the humeral shaft is relatively prone to nonunion with certain risk factors - TRANSVERSE fracture pattern, fracture DISTRACTION/gapping, proximal-third location, inadequate immobilisation, open fracture, infection, and patient factors (smoking, NSAIDs, obesity, diabetes, poor bone quality).
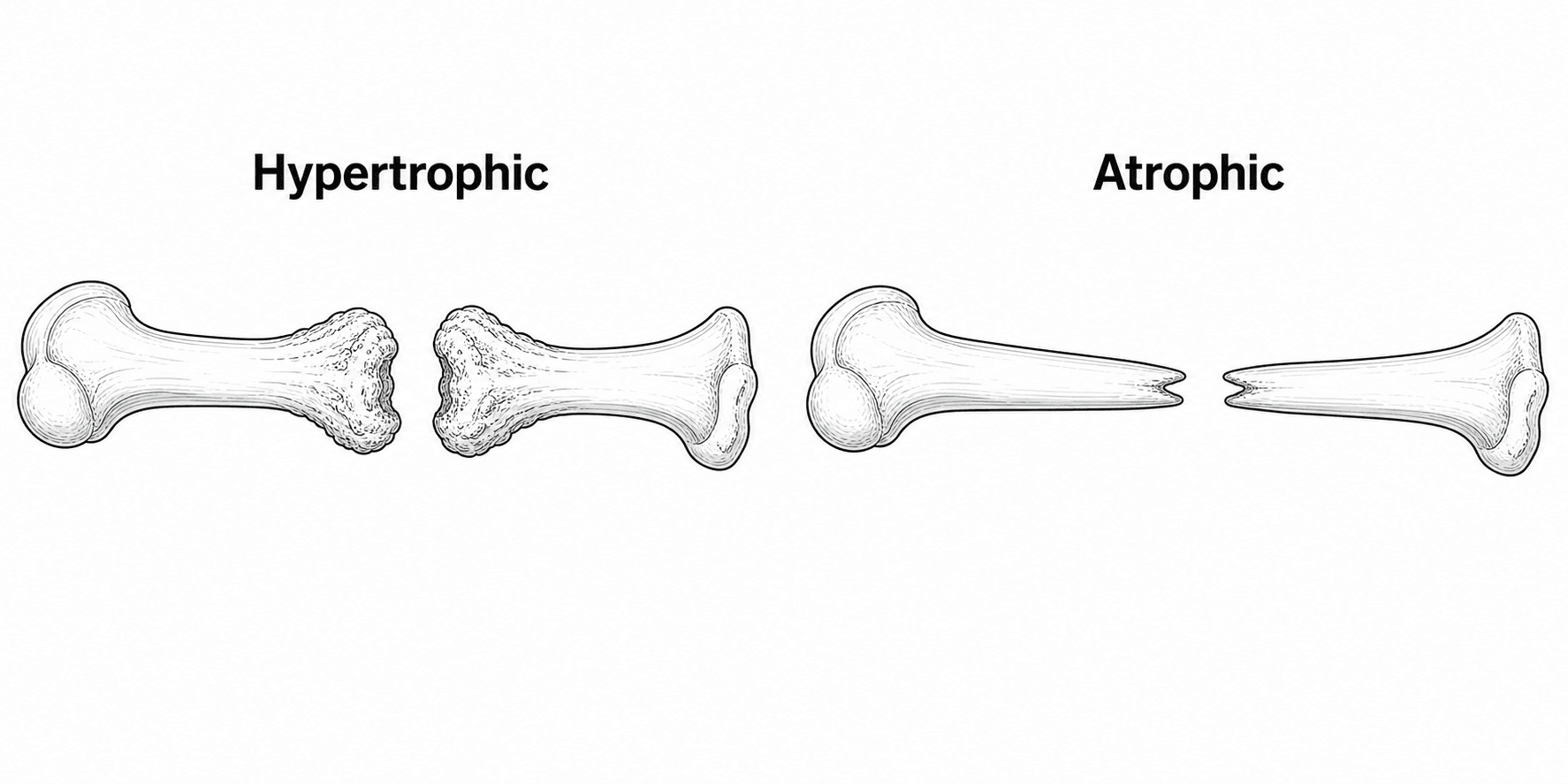
- Classify the nonunion: HYPERTROPHIC (abundant 'elephant-foot' callus that fails to bridge - a MECHANICAL/stability problem, with viable bone) versus ATROPHIC (tapered, sclerotic, avascular ends with a gap and little callus - a BIOLOGICAL problem) versus INFECTED.
- Always EXCLUDE INFECTION before treating (history, inflammatory markers, prior surgery), and document RADIAL NERVE function pre-operatively - the nerve is intimately related to the shaft and at risk both from the nonunion and during surgery.
- The GOLD-STANDARD treatment of aseptic humeral shaft nonunion is OPEN reduction with COMPRESSION PLATING (dynamic compression/locking plate) plus AUTOGENOUS (iliac crest) BONE GRAFT - this achieves UNION in the large majority (around 90-100% in series), restoring shoulder and elbow function.
- Unlike the femur and tibia, EXCHANGE NAILING is UNRELIABLE for humeral shaft nonunion; a failed nail is best converted to COMPRESSION PLATE FIXATION WITH BONE GRAFT rather than a larger nail.
- Atrophic and gap nonunions need the BIOLOGY addressed (autograft, and biological adjuncts such as BMP where appropriate); infected nonunions require infection ERADICATION (debridement, culture-directed antibiotics, sometimes staged reconstruction) alongside stabilisation - following the 'diamond concept' of stability + biology + a viable host.
- “Hypertrophic = stability problem (give compression); atrophic = biology problem (give compression PLUS bone graft).
- “In the HUMERUS, exchange nailing does NOT reliably achieve union - convert to compression plate + autograft.
- “Always exclude infection and check/protect the radial nerve before and during surgery.
For diaphyseal nonunion after nailing, exchange nailing (a larger reamed nail) is often effective - it adds stability and reams in biology.
Exchange nailing is UNRELIABLE in the humerus. A failed humeral nail (or a nonunion) is best treated by conversion to COMPRESSION PLATING with autogenous bone graft, which is the gold standard.
Risk Factors & Patterns
Most humeral shaft fractures heal with non-operative (functional bracing) or operative care, but nonunion occurs with identifiable risks:
- Fracture-related: a transverse fracture pattern, distraction/gapping (e.g. over-distraction in a brace or by gravity, soft-tissue interposition), proximal-third fractures, comminution/bone loss, open fractures and infection.
- Treatment-related: inadequate immobilisation/instability, and (with surgery) inadequate fixation.
- Patient-related: smoking, NSAIDs, diabetes, obesity, poor bone quality and other comorbidities. Recognising these helps both prevention and the management plan.
Classification & Assessment
- Hypertrophic - exuberant callus ('elephant-foot') but no bridging. The biology is intact; the problem is mechanical (insufficient stability). Providing rigid compression alone usually achieves union.
- Atrophic - tapered, avascular, sclerotic bone ends with a gap and little/no callus. The problem is biological (and often mechanical too); treatment must add bone graft / biology to stability.
- Infected (septic) nonunion - must be recognised and the infection eradicated as part of the plan.
- Radiographs (+/- CT) to confirm nonunion, characterise it (hyper/atrophic), and assess any implant/bone loss
- EXCLUDE INFECTION - history (wound problems, prior surgery), CRP/ESR/FBC, and intra-operative cultures where suspicion exists
- Document RADIAL NERVE function (and other neurovascular status) pre-operatively
- Optimise patient factors (stop smoking, review NSAIDs, correct metabolic/endocrine causes)
Successful union needs mechanical stability, osteogenic cells, an osteoconductive scaffold, osteoinductive signals (growth factors) and an adequate vascular/host environment - the framework guiding what each nonunion needs.
Excluding infection properly
"Exclude infection" is the instruction; these are the specifics, and the shoulder girdle has its own trap.
- Normal inflammatory markers do not exclude it. CRP and ESR are insensitive for the low-grade infection that causes a nonunion, so a normal CRP in a patient with previous surgery is reassurance you have not earned. Treat any nonunion after prior internal fixation as infected until proven otherwise.
- Take multiple separate deep cultures at surgery - conventionally five or more, each with fresh instruments and sent separately - because a single positive is usually contamination while two or more matching isolates indicate genuine infection.
- Ask the laboratory to hold cultures for 14 days. This is the point specific to the humerus and shoulder: Cutibacterium acnes is the region's characteristic low-virulence organism, it grows slowly, and a standard 48-hour culture will miss it. Failing to request extended culture is how a "presumed aseptic" nonunion gets plated over an occult infection.
- Expect some unexpected positives. A proportion of clinically aseptic nonunions grow an organism on intra-operative culture, which is why samples are taken even when infection is not suspected - the result changes antibiotic management afterwards even if the reconstruction proceeds.
- Send tissue for histology alongside culture where suspicion is real.
The metabolic screen the "optimise patient factors" line refers to
Where a nonunion is genuinely unexplained, the yield of screening is high enough that it is negligent to skip it. In the series that established this, 84% of carefully selected patients had at least one previously undiagnosed metabolic or endocrine abnormality - most often vitamin D deficiency (68%), along with calcium imbalance, central hypogonadism, and thyroid and parathyroid disorders. Most strikingly, eight patients united with medical treatment alone and no further surgery.
Read that number carefully, because it is easy to misquote: the 84% applies to selected patients meeting specific criteria - only 37 of 683 consecutive nonunions were referred - not to nonunions in general. The criteria are what to remember:
- Why it raises suspicion
- The mechanics were right, so the failure is likely to be in the host
- Why it raises suspicion
- Suggests a systemic bone problem rather than an isolated injury
- Why it raises suspicion
- A fracture that should heal on its own failing to do so points away from mechanics entirely
The practical screen is vitamin D and calcium, parathyroid hormone, thyroid function, and testosterone in men, with endocrinology referral rather than self-management when something is abnormal. A transverse humeral shaft fracture that was distracted in a brace is a mechanical explanation and does not need this; a well-fixed, well-reduced humerus that will not unite does.
Management
The gold-standard treatment of aseptic humeral shaft nonunion is open reduction and internal fixation with a COMPRESSION PLATE (dynamic compression or locking plate, achieving direct compression across the nonunion) supplemented with AUTOGENOUS (iliac crest) BONE GRAFT - especially for atrophic/gap nonunions. This combination addresses both stability and biology and achieves union in the large majority of cases (around 90-100% in large series), with restoration of shoulder and elbow function. The nonunion site is freshened/decorticated, any sclerotic/avascular bone and interposed tissue removed, and the canal reopened.
The biology is fine - provide rigid stability and compression (compression plating). Bone graft is often not essential but may be added. Union is highly reliable once stability is restored.
The radial nerve spirals around the humeral shaft and is intimately related to the mid/distal diaphysis (and to the nonunion and any callus). Document its function pre-operatively, identify and protect it intra-operatively (it may be encased in callus/scar at the nonunion), and counsel the patient about the risk of (usually transient) radial-nerve palsy, which is the commonest neurological complication of humeral nonunion surgery.
Approach & Finding the Radial Nerve
- Anterolateral (brachialis-splitting) suits proximal- and mid-third nonunions and gives an anterior surface for plating; the radial nerve is at risk distally, where it pierces the lateral intermuscular septum to enter the anterior compartment.
- Posterior (triceps-splitting or paratricipital/triceps-sparing) is favoured for mid- and distal-third nonunions: it gives a broad, flat posterior surface for a long plate and lets you identify the radial nerve directly in the spiral groove. The nerve crosses the posterior humerus in the spiral groove (with the profunda brachii vessels) in the middle third and pierces the lateral intermuscular septum roughly a hand's breadth above the lateral epicondyle.
The cardinal rule: find the nerve in normal tissue away from the nonunion and trace it into the scar or callus - never dissect blindly at the nonunion, where it may be encased in callus. If there is a pre-operative radial palsy or the nerve is tethered in callus, formally explore and neurolyse it as part of the procedure. A nerve that is identified, mobilised and protected throughout reduces the (usually transient) post-operative palsy that is the commonest neurological complication. (The detailed course of the nerve is in Radial Nerve Anatomy, and reconstruction of an established palsy in Tendon Transfers for Radial Nerve Palsy; the point here is finding and protecting it during nonunion surgery.)
Find the radial nerve in healthy tissue and trace it into the callus - never dissect blindly at the nonunion. Posterior approach (broad surface plus direct spiral-groove access) for mid/distal nonunions, anterolateral for proximal/mid; neurolyse a nerve entrapped in callus.
The Construct: More Than 'a Plate'
"Compression plate" is the headline, but the construct is what delivers union:
- A long, strong plate - a broad large-fragment (4.5 mm) dynamic-compression or locking plate spanning well beyond the nonunion, with adequate fixation in each main fragment (aim for at least three bicortical screws / six cortices each side, often more).
- Absolute stability with interfragmentary compression - compress a transverse or short-oblique nonunion through the plate (compression mode) or with a lag screw across an oblique nonunion, giving the rigid, gap-free environment that a hypertrophic nonunion needs for primary (direct) bone healing.
- Dual / orthogonal plating or a longer, stronger construct for osteopenic bone, rotational instability, or when a single plate is insufficient; locking screws improve fixation in osteoporotic bone.
- The autograft is packed at the freshened, decorticated nonunion (with the canal reopened), addressing biology while the construct delivers the mechanics.
This is why simply "putting on a plate" without compression or with too short a construct fails - the hypertrophic nonunion is a mechanical problem and needs genuine absolute stability. (General plate biomechanics - working length, stress concentration - are covered in Bending Moment Distribution.)
Specify the construct, not just "a plate": a long compression (or locking) plate with absolute stability / interfragmentary compression and at least three bicortical screws each side; reach for dual/orthogonal plating and locking screws in osteopenic or rotationally unstable nonunions.
Afterwards: Rehabilitation and What to Expect
Union is not the end of the operation - the commonest residual complaint after a successfully united humeral nonunion is a stiff shoulder or elbow, and that is determined by what happens in the weeks after surgery.
Post-operative course after compression plating and grafting
Sling for comfort only, not for immobilisation - a construct that achieved absolute stability does not need protecting from gravity. Document radial nerve function on waking and record it, since a new post-operative palsy needs to be distinguished from a pre-existing one. Iliac crest donor site is often the dominant early pain complaint; warn about this beforehand.
Immediate active-assisted shoulder and elbow motion within comfort - pendulum exercises, elbow flexion-extension and forearm rotation. The whole point of a rigid compression construct is that it permits early motion; nursing the arm in a sling for six weeks converts a united humerus into a stiff one.
Progress to active and then resisted exercise as pain allows. Avoid heavy lifting and torsional loading - a rotational force is what breaks a humeral plate - until there is radiographic bridging. Serial radiographs at roughly 6, 12 and 24 weeks.
Union in reported series averages around 16 weeks (roughly 10 to 26). Failure of progression by this point should prompt reassessment for occult infection or a metabolic cause rather than simply waiting longer.
Expect a period of shoulder and elbow stiffness, donor-site discomfort that can persist for months, and a visible scar. Plate removal is not routine and carries its own radial nerve risk - reserve it for genuinely symptomatic hardware after union is secure.
Mnemonics & Memory Aids
UNITE
Hook:To UNITE a humeral nonunion: type it, protect the nerve, exclude infection, compression-plate + graft, don't re-nail.
DIAMOND
Hook:The DIAMOND concept applied: stability + biology + viable host - and plate, don't re-nail, the humerus.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a humeral shaft nonunion 8 months after a transverse mid-shaft fracture treated in a brace. How do you classify and assess it, and what is the gold-standard treatment?”
“How does your management differ for a hypertrophic versus an atrophic versus an infected humeral nonunion, and why is the humerus different from the femur?”
Risk factors
- Transverse pattern, distraction/gapping, proximal-third, open, infection, comminution
- Inadequate immobilisation/instability
- Smoking, NSAIDs, diabetes, obesity, poor bone quality
Classify & assess
- Hypertrophic (elephant-foot callus = stability problem) vs atrophic (tapered/avascular = biology) vs infected
- EXCLUDE infection (CRP/ESR, cultures); document RADIAL NERVE
- Diamond concept: stability + cells + scaffold + signals + viable host
Treatment
- Gold standard (aseptic): compression plate + autogenous iliac-crest bone graft (~90-100% union)
- Hypertrophic: compression often suffices; atrophic/gap: add graft (+/- BMP/structural/transport)
- Infected: eradicate infection (staged) + stabilise + graft
Key pitfalls
- Exchange nailing UNRELIABLE in the humerus - convert to compression plate + graft
- Radial nerve at risk (commonest neuro complication) - protect it
- Don't reconstruct over unrecognised infection
Evidence & Key Studies
Treatment of nonunion of humeral shaft fracture with dynamic compression plate and cancellous bone graft
- In 105 humeral shaft nonunions (67 atrophic, 20 hypertrophic) treated with a dynamic compression plate plus cancellous bone graft, ALL united, at an average of 16 weeks (range 10-26).
- Complications were limited to 4 temporary radial-nerve palsies and 3 wound infections; shoulder and elbow function were satisfactory at follow-up.
- Compression plating with supplemental cancellous bone graft is a reliable, effective treatment for humeral shaft nonunion.
Repair of humeral shaft nonunion with plate and screw fixation and iliac crest bone graft
- Describes the technique for humeral shaft nonunion repair: nonunion-site preparation, direct compression of the fracture using plate osteosynthesis, and iliac crest bone graft harvest/utilisation.
- Reinforces compression plating with autogenous bone graft as the management approach for humeral shaft nonunion.
- Emphasises freshening the nonunion and achieving direct compression across the site.
Metabolic and endocrine abnormalities in patients with nonunions
- 37 patients selected from 683 consecutive nonunions by three criteria - an unexplained nonunion despite adequate reduction and fixation, multiple low-energy fractures with at least one nonunion, or nonunion of a non-displaced pubic ramus or sacral ala fracture - were referred for endocrine evaluation.
- 31 of 37 (84%) had at least one NEW metabolic or endocrine diagnosis; vitamin D deficiency was commonest at 25 of 37 (68%), with calcium imbalance, central hypogonadism, and thyroid and parathyroid disorders also found.
- Eight patients achieved union with medical treatment alone and no further surgery, at a mean of 7.6 months after seeing the endocrinologist.
The high union rates and complication profile of compression plating plus cancellous bone graft come from the cited Hsu series, and the technique (nonunion preparation, direct compression, iliac-crest autograft) from the cited Egol-group description. The hypertrophic/atrophic classification, the diamond concept, and the unreliability of exchange nailing in the humerus are standard, well-established teaching, as are the infection work-up specifics and the post-operative course. The metabolic and endocrine screening criteria, the 84% and 68% figures and the eight patients who united medically come from the cited Brinker series. (See also Nonunion Management, Humeral Shaft Fractures, Proximal Humerus Nonunion and Bone Grafts.)