Surgical-Neck Nonunion & Tuberosity Malunion
- Nonunion of the proximal humerus most often occurs at the SURGICAL NECK (a two-part surgical-neck nonunion is the classic), and corresponds to a BOILEAU TYPE-3 fracture sequela; it presents with pain, instability/'pseudoparalysis' and a mobile, painful nonunion months after the injury.
- Risk factors include DISPLACED/comminuted fractures, metaphyseal comminution, OSTEOPOROSIS, inadequate fixation/stability, soft-tissue interposition, and patient factors (smoking) - the elderly osteoporotic two-part surgical-neck fracture is the typical setting.
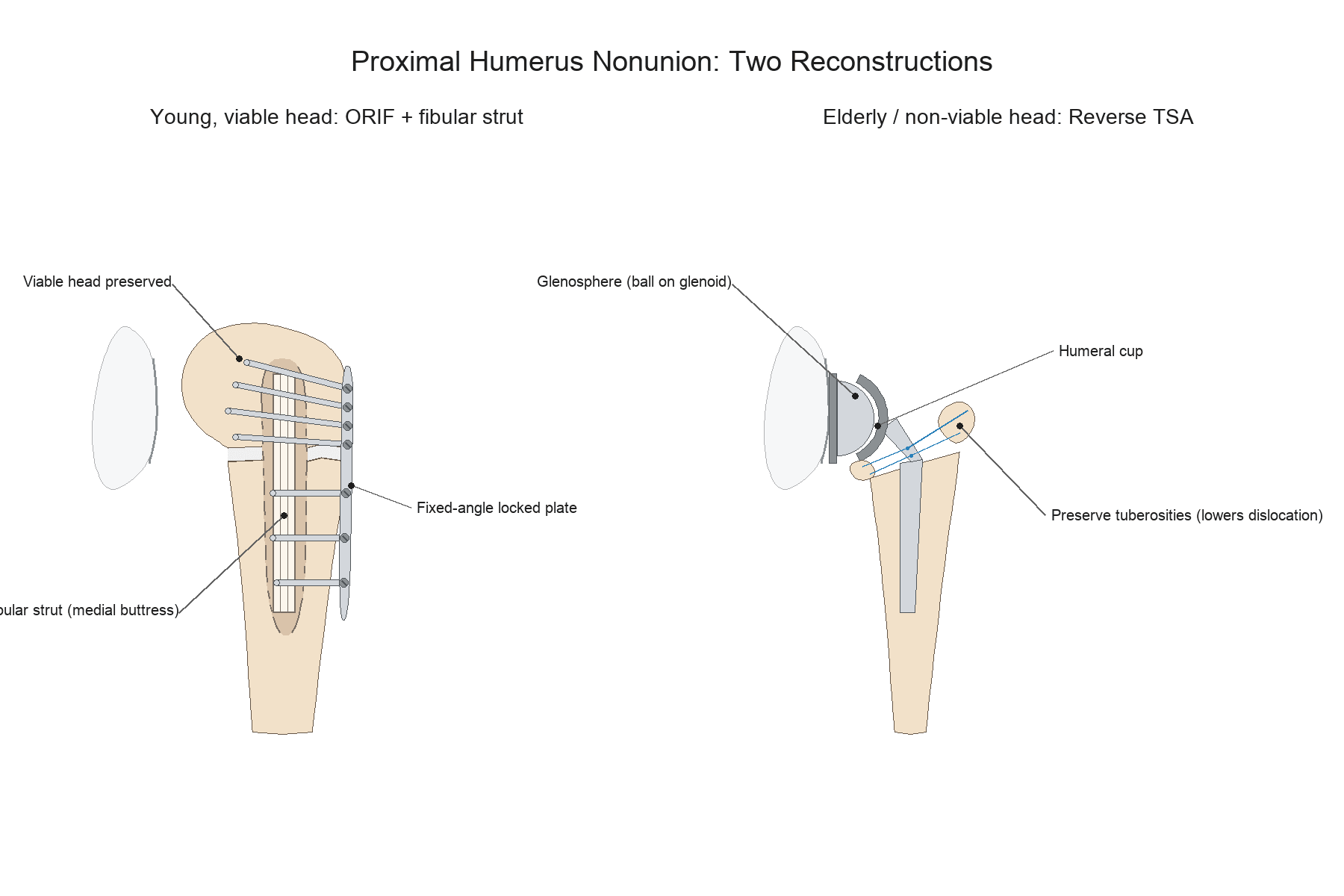
- Treatment is driven by AGE, HUMERAL HEAD VIABILITY, BONE STOCK and the ROTATOR CUFF: a YOUNGER patient with GOOD bone stock, a VIABLE head and an intact cuff is best treated by HEAD-PRESERVING ORIF - a fixed-angle LOCKED PLATE (or blade plate) plus BONE GRAFT (often an intramedullary FIBULAR STRUT and/or cancellous graft) - which reliably unites the surgical neck.
- An ELDERLY patient with POOR bone stock, a NON-VIABLE or small head fragment, a DEFICIENT rotator cuff, or a FAILED ORIF is best treated by ARTHROPLASTY - REVERSE total shoulder arthroplasty (RSA), which is cuff-independent and gives reliable pain relief and improved function; a LONG-STEM RSA is used for metadiaphyseal extension.
- A KEY LESSON with RSA for nonunion: PRESERVE the TUBEROSITIES and attached rotator cuff if possible - intra-operative RESECTION of the tuberosities markedly INCREASES the DISLOCATION rate (which is already high in this group); surgical-neck nonunion and tuberosity malunion (Boileau 3 and 4) have worse arthroplasty outcomes than impacted-collapse sequelae because they require tuberosity osteotomy.
- MALUNION of the proximal humerus - GREATER-TUBEROSITY malunion (causing subacromial/internal impingement and lost motion) or SURGICAL-NECK angulation - is managed by tuberosity osteotomy/excision/acromioplasty, corrective osteotomy, or arthroplasty depending on severity and joint condition.
- “The proximal humerus nonunion is usually a SURGICAL-NECK nonunion (Boileau type-3 sequela).
- “Decide by age/head viability/bone stock/cuff: young+viable -> ORIF (locked plate) + bone graft (fibular strut); elderly/non-viable/cuff-poor/failed -> reverse TSA.
- “With RSA for nonunion, PRESERVE the tuberosities - resecting them greatly raises the dislocation rate.
Good bone stock, a viable head and an intact cuff favour head-preserving ORIF - a fixed-angle locked plate (or blade plate) with bone graft (intramedullary fibular strut / cancellous graft) to unite the surgical neck.
Poor bone stock, a non-viable/small head, a deficient cuff, or a failed ORIF favour reverse total shoulder arthroplasty (cuff-independent) - PRESERVE the tuberosities to limit the high dislocation rate; long-stem for metadiaphyseal extension.
The Surgical-Neck Nonunion (Boileau Type 3)
The proximal humerus most commonly fails to unite at the surgical neck - the classic two-part surgical-neck nonunion, designated a Boileau type-3 fracture sequela. Contributing factors are displacement and comminution (especially metaphyseal comminution), osteoporosis, inadequate fixation or stability, soft-tissue interposition, and the deforming muscle forces (pectoralis major pulling the shaft medially, the cuff abducting/rotating the head) that distract the fracture. The typical patient is elderly and osteoporotic. Patients present with pain, weakness/pseudoparalysis and a mobile, painful nonunion months after the fracture.
Assessment
- Radiographs (+/- CT) to confirm nonunion, characterise the fragments and assess bone stock
- Head viability (AVN/cephalic collapse) and head-fragment size (can it hold fixation?)
- Rotator cuff integrity (clinical +/- imaging) - central to the ORIF-vs-RSA decision
- Patient age, demand, comorbidities; exclude infection before reconstruction
Boileau type 1 (impacted cephalic collapse) does well with prosthesis without tuberosity osteotomy; types 3 (surgical-neck nonunion) and 4 (severe tuberosity malunion) require tuberosity osteotomy and have worse arthroplasty outcomes - informing expectations and technique.
Management
Head-preserving open reduction and internal fixation with a fixed-angle locked plate (or blade plate), combined with bone grafting - commonly an intramedullary FIBULAR STRUT (provides a medial buttress and improves fixation in osteoporotic/comminuted metaphysis) and/or cancellous autograft. Requires a viable head with a fragment large enough to hold fixation and adequate bone stock. Achieves reliable union and preserves the native joint.
Excluding Infection Before You Reconstruct
Infection must be excluded before reconstruction, because an unrecognised low-grade (septic) nonunion will defeat both ORIF and arthroplasty. The shoulder's defining caveat is the organism: Cutibacterium (formerly Propionibacterium) acnes is the predominant indolent shoulder pathogen, and it characteristically produces few clinical signs and normal or only mildly raised CRP/ESR, so a "clean" blood panel does not exclude infection - maintain a high index of suspicion in any failed-fixation or recurrent nonunion.
- Screen: history (rest/night pain, prior surgery, wound-healing problems), examination, and inflammatory markers (CRP/ESR) - useful when raised but unreliable when normal for C. acnes.
- Sample properly: consider pre-operative aspiration, and at surgery take multiple separate deep tissue samples for microbiology and histology, held for prolonged (around two-week) culture to capture the slow- growing C. acnes; do not rely on a single swab.
- If infected: treat as a septic nonunion - debridement, organism-directed antibiotics and a staged reconstruction rather than a one-stage definitive procedure. The detailed C. acnes microbiology and management is developed in Cutibacterium acnes Shoulder Infection, and the general principles in Nonunion Management. The infection work-up belongs in the reconstruction decision itself, not after it.
"Exclude infection" in the shoulder specifically means think Cutibacterium acnes: normal CRP/ESR does not clear it, so take multiple deep cultures held ~14 days before committing to a definitive ORIF or arthroplasty. A missed indolent infection is a leading cause of recurrent nonunion and of early prosthetic failure.
Optimise the Host, Not Just the Construct
The typical patient here is described throughout as elderly and osteoporotic, and that is not only an explanation for why the fracture failed - it is a list of things to correct before and after reconstruction. Re-operating on an unoptimised host repeats the conditions that produced the nonunion.
- Threshold or action
- Target above 75 nmol/L; replace if below
- Why it matters here
- Deficiency is common in this population and impairs mineralisation of any callus the graft is meant to generate
- Threshold or action
- Screen for occult metabolic bone disease
- Why it matters here
- Hyperparathyroidism and osteomalacia present as fragility and failed healing, and are treatable
- Threshold or action
- Correct deficiency before elective reconstruction
- Why it matters here
- Malnutrition and endocrine disturbance both impair union
- Threshold or action
- Cessation - not merely recorded as a risk factor
- Why it matters here
- Nicotine vasoconstriction is one of the few modifiable causes of atrophic nonunion, and this is the moment the patient is most likely to act
- Threshold or action
- A fragility fracture that then failed to unite is an unambiguous indication to assess and treat the bone
- Why it matters here
- The same skeleton will be asked to hold the revision fixation
These figures and the wider work-up follow Nonunion Management, so the same thresholds apply whichever bone has failed to unite. The point specific to the proximal humerus is that the demographic makes every item on the list more likely to be abnormal, not less.
The Nonunion's Biology: Why Fixation Alone Is Not Enough
Bone graft, a fibular strut and inadequate stability are best understood through the hypertrophic-versus-atrophic framework of nonunion (developed in full in Nonunion Management):
- Hypertrophic nonunion (abundant "elephant-foot" callus) signals adequate biology but inadequate mechanical stability - it usually unites with stable fixation alone, no graft needed.
- Atrophic / oligotrophic nonunion (little or no callus) signals failed biology - it needs biological augmentation (graft, and correction of any instability), not just more metalwork.
The proximal-humerus surgical-neck nonunion is typically atrophic/oligotrophic: it occurs in osteoporotic bone with metaphyseal comminution, poor metaphyseal vascularity and deforming muscle pull, so simply re-fixing it (revision plating alone) tends to fail. That is exactly why head-preserving ORIF must combine a fixed-angle locked (or blade) plate for stability with biological and structural augmentation - an intramedullary fibular strut to restore the medial calcar buttress and grip in osteoporotic bone, plus cancellous autograft at the nonunion (graft choice is covered in Bone Grafts). Address both the mechanics and the biology, or the nonunion recurs.
Classify the nonunion: hypertrophic = stability problem (fix it rigidly), atrophic = biology problem (graft it). The proximal-humerus surgical-neck nonunion is usually atrophic in osteoporotic bone, so ORIF pairs a fixed-angle plate with a fibular strut + cancellous graft (medial calcar support) - fixation alone recurs.
Mnemonics & Memory Aids
NECK
Hook:Proximal humerus NECK nonunion: evaluate, choose ORIF vs reverse TSA, and keep the tuberosities.
BOILEAU
Hook:Boileau sequelae 1-4: collapse, locked dislocation, nonunion, malunion - 3 and 4 are the hard ones.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old has a painful, mobile surgical-neck nonunion 8 months after a proximal humerus fracture, with a viable head and intact cuff on imaging. How would you classify and treat this?”
“An 80-year-old with osteoporotic bone, a small avascular head fragment and a deficient cuff has a surgical-neck nonunion. What would you do, and what is the key technical pitfall?”
Nonunion
- Commonest at the surgical neck (two-part); Boileau type-3 sequela
- Risk: displaced/comminuted, osteoporosis, poor fixation, soft-tissue interposition, deforming muscle pull
- Presents with pain, weakness/pseudoparalysis, mobile painful nonunion
Decision drivers
- Age, head viability, bone stock, rotator cuff; exclude infection
- Boileau type 1 does best with prosthesis (no tuberosity osteotomy); types 3-4 worse
- Assess radiographs + CT; head-fragment size for fixation
Treatment
- Young + viable head + intact cuff: ORIF (locked/blade plate) + bone graft (fibular strut + cancellous)
- Elderly / non-viable / cuff-deficient / failed ORIF: reverse TSA (cuff-independent); long-stem for metadiaphyseal
- PRESERVE the tuberosities (RSA) - resection raises dislocation rate (Raiss 34%)
Malunion
- Greater-tuberosity malunion -> impingement/lost motion (osteotomy/excision/acromioplasty)
- Surgical-neck angulation -> corrective osteotomy
- Severe malunion + joint damage -> arthroplasty (Boileau type 4)
Evidence & Key Studies
Reverse shoulder arthroplasty for the treatment of nonunions of the surgical neck of the proximal humerus (type-3 fracture sequelae)
- In 32 patients (mean age 68) with surgical-neck nonunion treated by reverse shoulder arthroplasty, the Constant score improved from 14.2 to 46.6 and flexion from 42.9 to 109.7 degrees.
- Complications occurred in 41% with revisions in 28%; dislocation (34%) was the most common complication.
- Intra-operative resection of the tuberosities was associated with increased dislocation risk - the tuberosities and attached cuff should be preserved when possible.
Cementless long-stem reverse total shoulder arthroplasty as primary treatment for metadiaphyseal humeral shaft fractures
- Cementless long-stem reverse TSA, with the stem spanning two canal diameters past the fracture and strut-allograft/cerclage augmentation as needed, treats complex metadiaphyseal proximal-humeral fractures in elderly osteoporotic patients.
- It addresses concomitant arthritis/cuff pathology that ORIF and nailing do not, with consistent healing (union ~13 months), pain relief and functional recovery.
- Combines arthroplasty (length restoration) with osteosynthesis principles (relative and absolute stability for the fragments).
The reverse-TSA outcomes for surgical-neck nonunion and the crucial tuberosity- preservation lesson come from the cited Raiss series, and the long-stem cementless RSA technique for metadiaphyseal extension from the cited Witt description. The Boileau classification of fracture sequelae, the ORIF-with-fibular-strut head-preserving option, and the malunion management are standard, well- established teaching. The complication, revision and dislocation percentages quoted in the management section are the Raiss figures and come from that single 32-patient series. The metabolic thresholds - the 75 nmol/L vitamin D target and the calcium, phosphate, alkaline phosphatase and PTH screen - are taken from Nonunion Management so the same numbers apply across every nonunion topic. (See also Proximal Humerus Fractures, Reverse Total Shoulder Arthroplasty, Humeral Shaft Nonunion and Bone Grafts.)