Inflammation & Cytokines
Sustained pro-inflammatory cytokine signalling (TNF-α, IL-1, IL-6, IL-17) drives cartilage degradation, bone erosion and synovitis - the basis of rheumatoid arthritis, contributes to periprosthetic osteolysis and inflammatory bone loss.
The same cytokines initiate the inflammatory phase of fracture healing and host defence against infection. Inflammation is a necessary repair signal - the goal is to control excess, not abolish it.
Overview: The Inflammatory Response & Cytokines
Cytokines are small secreted signalling proteins that act in autocrine, paracrine and sometimes endocrine fashion to coordinate inflammation, immunity and tissue repair. They include the interleukins (IL), tumour necrosis factors (TNF), interferons, chemokines and growth factors. The acute inflammatory response to injury or infection (the classic rubor, calor, dolor, tumor, functio laesa) is orchestrated by them: tissue macrophages and recruited cells release pro-inflammatory cytokines (TNF-α, IL-1, IL-6) that cause vasodilation, increased vascular permeability, leukocyte recruitment and the systemic acute-phase response (fever, CRP). Resolution is driven by anti-inflammatory mediators (IL-10, TGF-β, IL-1Ra) and pro-resolution lipids.
- Main source
- Macrophages
- Principal actions
- Master pro-inflammatory; up-regulates RANKL/other cytokines; resorption
- Drug target
- Etanercept, infliximab, adalimumab
- Main source
- Macrophages
- Principal actions
- Cartilage degradation (MMPs), bone resorption, fever
- Drug target
- Anakinra (IL-1Ra); ACS
- Main source
- Macrophages, T cells, fibroblasts
- Principal actions
- Chronic inflammation, acute-phase (CRP), osteoclastogenesis
- Drug target
- Tocilizumab (anti-IL-6R)
- Main source
- Th17 cells
- Principal actions
- Promotes RANKL, joint inflammation (RA, spondyloarthritis)
- Drug target
- Secukinumab (anti-IL-17)
- Main source
- Tregs, macrophages
- Principal actions
- Anti-inflammatory / resolution
- Drug target
- (pro-resolution)
Before the cytokines are released, the innate immune system must sense danger — the examinable upstream step:
- Pattern-recognition receptors (chiefly Toll-like receptors, TLRs) on macrophages detect PAMPs (pathogen-associated molecular patterns, e.g. bacterial LPS) and DAMPs (damage-associated molecular patterns released by injured/necrotic cells) — the same sensing that lets wear debris act as a "sterile" danger signal in periprosthetic osteolysis.
- Engagement drives NF-κB transcription of pro-inflammatory genes, producing TNF-α, IL-6 and pro-IL-1β (an inactive precursor).
- The NLRP3 inflammasome is the second signal: it assembles and activates caspase-1, which cleaves pro-IL-1β into active IL-1β — the molecular origin of the IL-1 the rest of this topic discusses. This is the pathway that monosodium-urate crystals activate in gout (and a proposed mechanism for crystal- and particle-induced "sterile" inflammation), and the rationale for IL-1 blockade (anakinra) and colchicine.
So: TLR sensing of PAMPs/DAMPs → NF-κB → cytokine transcription, with the NLRP3 inflammasome/caspase-1 step specifically maturing IL-1β.
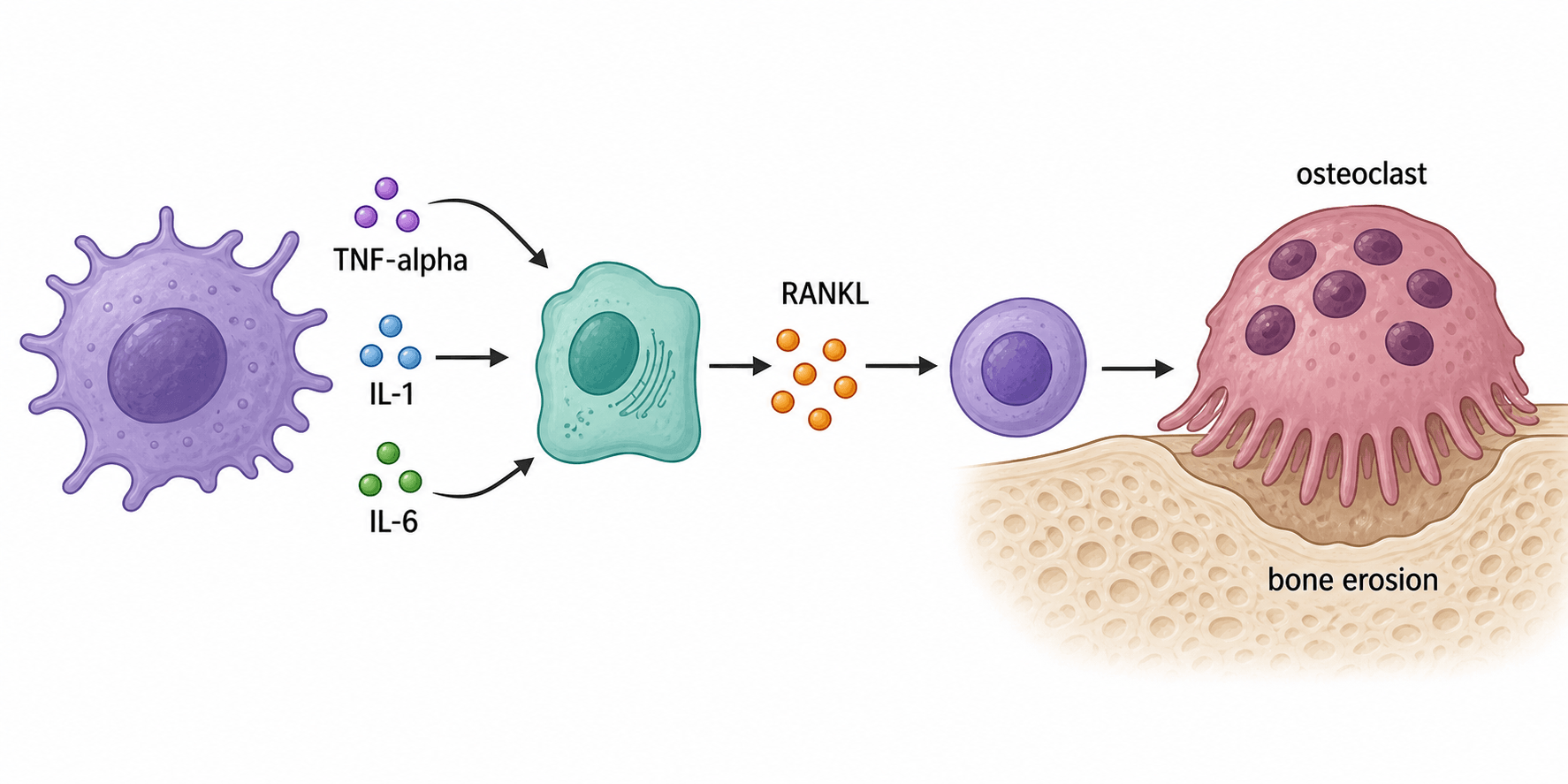
Mechanism: Osteoimmunology — How Cytokines Erode Bone
Osteoimmunology describes the shared signalling between the immune and skeletal systems. The unifying mechanism of inflammatory bone loss is that pro-inflammatory cytokines (TNF-α, IL-1, IL-6, IL-17) up-regulate RANKL (and reduce OPG) on osteoblast-lineage/stromal cells, tipping the RANKL:OPG ratio toward osteoclast formation and activity - producing bone erosion. TNF-α and IL-1 can also act more directly on osteoclast precursors and impair osteoblastic repair, so erosions both enlarge and fail to heal. This is the molecular engine behind the joint destruction of inflammatory arthritis.
Clinical Correlations

Cells in the inflamed synovium and pannus elaborate TNF-α, IL-1, IL-6 and IL-17, which drive synovitis and, through the RANK/RANKL/OPG pathway, articular bone erosions and periarticular osteoporosis; the cytokines also impair osteoblastic repair of erosions. This mechanistic understanding underpins biologic therapy.
The systemic arm of the cytokine response is the acute-phase response, driven chiefly by IL-6 acting on hepatocytes - and it is what gives you the two inflammatory markers used daily in orthopaedics. Knowing their kinetics is the examinable point:
- CRP is a hepatocyte-synthesised acute-phase protein: it rises within about 6 hours, peaks around 48 hours, and has a short half-life (~19 hours), so it falls quickly once inflammation settles. That fast on/off makes it the marker for monitoring an acute process - post-operative course, response to treatment, and suspected periprosthetic joint infection.
- ESR is an indirect marker (it reflects fibrinogen and immunoglobulin-driven red-cell rouleaux): it rises and falls slowly over weeks and is confounded by age, anaemia, pregnancy and paraproteins - so it lags and is less useful for tracking rapid change.
- Orthopaedic use: a normal CRP and ESR together have a high negative predictive value for screening PJI; a persistently rising or non-falling CRP after arthroplasty raises the suspicion of infection. Remember tocilizumab (anti-IL-6R) suppresses CRP, so the marker can be falsely reassuring in patients on that biologic.
Biologic Therapies
- Drug(s)
- Etanercept, infliximab, adalimumab
- Mechanism
- Anti-TNF (receptor-fusion or monoclonal antibody)
- Key caveat
- Infection risk (incl. TB reactivation); screen first
- Drug(s)
- Tocilizumab
- Mechanism
- Blocks IL-6 signalling (also lowers CRP)
- Key caveat
- Infection; may mask CRP rise
- Drug(s)
- Anakinra (IL-1 receptor antagonist)
- Mechanism
- Competitively blocks IL-1
- Key caveat
- Injection-site reactions; infection
- Drug(s)
- Secukinumab
- Mechanism
- Anti-IL-17 (spondyloarthritis, psoriatic)
- Key caveat
- Infection; candidiasis
- Drug(s)
- Denosumab
- Mechanism
- Antiresorptive (downstream of cytokines)
- Key caveat
- Rebound on cessation
Biologics are immunosuppressive, so a key orthopaedic consideration is peri-operative management - balancing infection/wound-healing risk against disease flare, typically by timing surgery around the drug's dosing interval and following rheumatology/society guidance. Always screen for latent infection (e.g. TB) before starting anti-TNF therapy.
The biologics above are extracellular antibodies; examiners also want the intracellular signalling pathways and the oral drug class that blocks them:
- TNF-α (via TNFR) and IL-1 (via IL-1R/MyD88) signal mainly through NF-κB and the MAPK cascades to switch on inflammatory genes.
- IL-6 (via IL-6R/gp130) and the interferons signal through the JAK-STAT pathway (notably STAT3).
- JAK inhibitors (tofacitinib, baricitinib, upadacitinib) are oral targeted-synthetic DMARDs that block Janus kinases and so dampen JAK-STAT-dependent cytokine signalling intracellularly — a different mechanism from the injectable biologics but the same anti-cytokine goal.
- Caveats: like the biologics they are immunosuppressive (serious infection, herpes-zoster reactivation) and carry class warnings for VTE and major cardiovascular events/malignancy (the ORAL Surveillance signal); the ACR/AAHKS perioperative guideline withholds JAK inhibitors before elective arthroplasty (unlike traditional DMARDs, which are continued).
Mnemonics & Memory Aids
HOT
Hook:Inflammation is HOT: the trio, the osteoclast link, and the targeted treatments.
TANK
Hook:TANK: the cytokine-blocking biologics and the RANKL knock-on they all converge on.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Which cytokines drive the joint destruction of rheumatoid arthritis, by what mechanism is bone eroded, and how do biologic drugs intervene?”
“Is inflammation always harmful in orthopaedics? Give examples where cytokines are necessary and where they cause harm.”
The key cytokines
- Pro-inflammatory trio: TNF-α (master), IL-1 (cartilage/MMPs), IL-6 (acute-phase/CRP); plus IL-17
- Anti-inflammatory/resolution: IL-10, TGF-β, IL-1Ra
- Sources mainly macrophages (and T cells/fibroblasts)
Osteoimmunology
- Cytokines up-regulate RANKL (lower OPG) to osteoclasts to bone erosion
- Also impair osteoblastic repair (erosions enlarge, don't heal)
- Mechanism of RA erosions and wear-debris osteolysis
Clinical links
- RA: synovial/pannus cytokines to erosions + periarticular osteoporosis
- Periprosthetic osteolysis: wear debris to macrophage cytokines to RANKL
- Infection: acute-phase response (CRP/ESR); fracture healing needs early inflammation
Biologic targets
- Anti-TNF (etanercept/infliximab/adalimumab); anti-IL-6R (tocilizumab); IL-1Ra (anakinra); anti-IL-17 (secukinumab)
- Immunosuppressive: screen TB before anti-TNF; peri-operative timing (infection vs flare)
- Denosumab blocks RANKL downstream
Evidence & Key Studies
Bone damage in rheumatoid arthritis: mechanistic insights and approaches to prevention
- Cells in the inflamed RA synovium/pannus elaborate TNF-α, IL-1, IL-6 and IL-17 that contribute to inflammation and directly affect bone.
- The RANK/RANKL/OPG pathway is critical in regulating osteoclastogenesis at articular bone erosions; pro-inflammatory cytokines modulate this pathway.
- These cytokines also impair the osteoblast's ability to repair bone at erosion sites - explaining why erosions enlarge and fail to heal.
Paget's disease of bone: an osteoimmunological disorder?
- Osteoimmunology arises from cross-talk between bone and immune systems; RANK/RANKL/OPG plus TNF-α, IL-1, IL-6 and IL-17 are pivotal.
- Osteoimmunological disorders (rheumatoid arthritis, osteoporosis, periodontitis) can be characterised by patterns of cytokine/serum biomarkers.
- Targeted therapies against RANKL and IL-6 signalling exemplify treating bone disease via immune pathways.
The central role of wear debris in periprosthetic osteolysis
- Identifies the macrophage as the central cellular target of wear debris in periprosthetic osteolysis - the commonest cause of aseptic loosening and revision after total hip arthroplasty.
- Wear particles activate pro-inflammatory signalling (TNF and others) driving osteoclast recruitment, AND inhibit protective anti-osteoclastogenic cytokines such as interferon-gamma - both increasing bone resorption via MAPK/NF-κB cascades.
- Anti-TNF, bisphosphonates and RANKL-blocking agents reduce osteolysis in animal models, but no approved drug therapy for established osteolysis yet exists - prevention (low-wear bearings) remains key.
The RA cytokine-to-RANKL erosion mechanism comes from the Gravallese-group review (Karmakar et al., DOI), the broader osteoimmunology framing from Numan et al. (DOI), and the periprosthetic-osteolysis application from Purdue et al. (DOI). The specific cytokine sources/actions and the biologic drug targets are standard, well-established immunology and pharmacology used throughout the literature, not findings of any single study.