Sole Motor Nerve to Gluteus Maximus
- The INFERIOR GLUTEAL NERVE arises from the sacral plexus from the roots L5, S1 and S2, and it is a PURELY MOTOR nerve (it has no cutaneous/sensory branch); it provides the SOLE motor supply to the GLUTEUS MAXIMUS muscle.
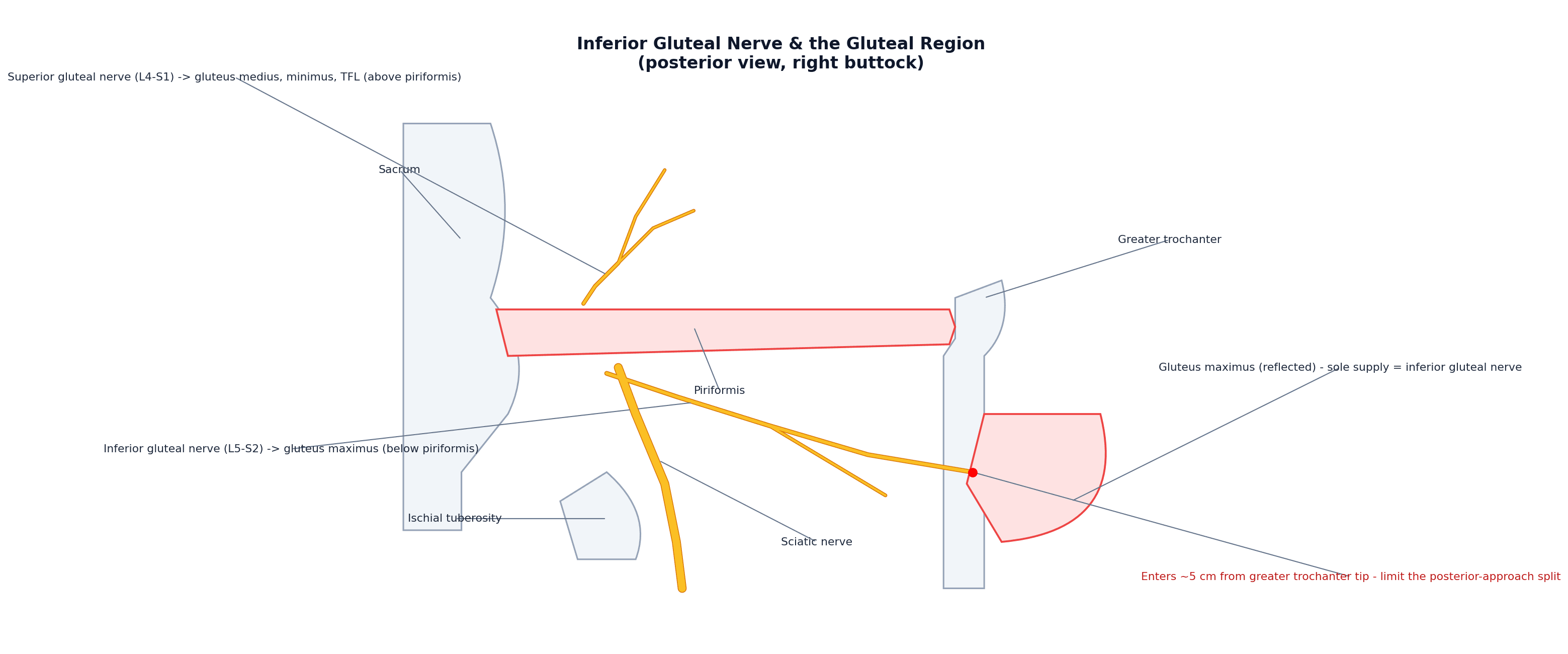
- It exits the pelvis through the greater sciatic foramen BELOW PIRIFORMIS (in contrast to the SUPERIOR gluteal nerve, which exits ABOVE piriformis), and then immediately breaks up into branches that enter the DEEP (anterior) surface of gluteus maximus.
- FUNCTIONALLY, gluteus maximus is the principal HIP EXTENSOR - most important when extending the hip from a FLEXED position, such as rising from sitting, climbing stairs, and running/jumping - and it is also a lateral rotator of the hip, with its upper fibres assisting abduction (via the iliotibial band); the inferior gluteal nerve therefore powers powerful hip extension.
- INJURY to the inferior gluteal nerve causes weakness of hip extension - difficulty rising from a chair, climbing stairs and running - and a characteristic GLUTEUS MAXIMUS LURCH (a backward thrust of the trunk in stance to keep the hip extended over the limb), together with gluteus maximus atrophy/flattening of the buttock; it does NOT cause a Trendelenburg gait (that is the SUPERIOR gluteal nerve / hip abductors).
- The KEY SURGICAL-ANATOMY point is that the inferior gluteal nerve enters the deep surface of gluteus maximus approximately 5 cm from the tip of the GREATER TROCHANTER, so it is vulnerable in the POSTERIOR approach to the hip: if the gluteus maximus is split and parted MORE than about 5 cm from the greater trochanter tip, the nerve can be damaged before it is even seen, hence the recommendation to limit the proximal extent of the split (a modified/safe posterior approach).
- Across hip approaches, partial denervation of gluteus maximus is most associated with the POSTERIOR approach (EMG studies show partial gluteus maximus denervation in a majority of posterior-approach patients), whereas the anterolateral approach mainly threatens the superior gluteal nerve branch to tensor fasciae latae; reassuringly, in primary THA the clinical sequelae of these partial lesions are usually not significant, but the anatomy still guides a careful approach.
- “Inferior gluteal nerve (L5-S2) = SOLE motor supply of GLUTEUS MAXIMUS; purely MOTOR; exits BELOW piriformis (superior gluteal nerve exits ABOVE).
- “Gluteus maximus = main HIP EXTENSOR (from flexion: rising/stairs/running) + lateral rotator. Injury -> weak hip extension + GLUTEUS MAXIMUS LURCH (NOT Trendelenburg - that's superior gluteal nerve).
- “Enters gluteus maximus ~5 cm from the GT tip -> in the POSTERIOR hip approach, don't split the muscle more than ~5 cm from the GT (safe split).
L5-S2, purely motor, the sole supply to gluteus maximus; exits below piriformis. Powers hip extension (rising/stairs/running) and lateral rotation.
Injury -> weak hip extension + gluteus maximus lurch (NOT Trendelenburg). Enters maximus ~5 cm from the GT tip -> safe-split limit in the posterior hip approach.
Origin, Function & the Safe Split
The inferior gluteal nerve (L5, S1, S2) is a purely motor nerve and the sole motor supply to gluteus maximus. It exits the pelvis through the greater sciatic foramen below piriformis (the superior gluteal nerve exits above), and enters the deep surface of gluteus maximus. Gluteus maximus is the principal hip extensor, most important from a flexed position (rising from sitting, stairs, running/jumping), and a lateral rotator (upper fibres assist abduction via the iliotibial band). Injury therefore causes weak hip extension and a gluteus maximus lurch (backward trunk thrust), with buttock atrophy - but NOT a Trendelenburg gait (that is the superior gluteal nerve/abductors). Surgically, the nerve enters gluteus maximus about 5 cm from the greater trochanter tip, so in the posterior hip approach the muscle split should not extend more than ~5 cm proximal to the greater trochanter, to avoid damaging the nerve before it is seen.
- Inferior gluteal nerve
- L5, S1, S2
- Superior gluteal nerve
- L4, L5, S1
- Inferior gluteal nerve
- Below piriformis
- Superior gluteal nerve
- Above piriformis
- Inferior gluteal nerve
- Gluteus maximus (sole supply)
- Superior gluteal nerve
- Gluteus medius, gluteus minimus, tensor fasciae latae
- Inferior gluteal nerve
- Hip extension (from flexion), lateral rotation
- Superior gluteal nerve
- Hip abduction (pelvic stabiliser in stance)
- Inferior gluteal nerve
- Gluteus maximus lurch (backward trunk thrust)
- Superior gluteal nerve
- Trendelenburg gait/lurch
Gluteus Maximus: The Muscle the Nerve Powers
Because the inferior gluteal nerve is the sole supply of gluteus maximus, its functional importance follows from the muscle's attachments - high-yield anatomy in its own right.
- Origin (broad): the posterior gluteal line of the ilium and bone behind it, the posterior aspect of the lower sacrum and coccyx, the sacrotuberous ligament, and the thoracolumbar fascia.
- Dual insertion: the upper roughly three-quarters of the muscle inserts into the iliotibial tract, and the deep lower quarter inserts into the gluteal tuberosity of the femur.
- It is the largest and most superficial gluteal muscle and the body's most powerful hip extensor.
- Via its iliotibial-tract insertion, gluteus maximus tenses the fascia lata and helps stabilise the extended knee and the lateral hip - so its weakness affects more than straight-line extension.
- Upper fibres (above the hip-joint axis) assist abduction through the ITB; lower fibres assist adduction; the whole muscle is a lateral rotator.
- As the only powerful extensor of the flexed hip, gluteus maximus (and therefore the inferior gluteal nerve) is indispensable for rising from sitting, stair-climbing and running - exactly the activities lost when the nerve is injured.
Injury & Surgical Relevance
- Deficit: weak hip extension - difficulty rising from a chair, climbing stairs and running - with a gluteus maximus lurch (backward trunk thrust in stance) and gluteus maximus atrophy.
- Distinguish from the superior gluteal nerve: that causes hip-abductor weakness and a Trendelenburg gait, not a gluteus maximus lurch.
- Posterior hip approach: the nerve enters gluteus maximus ~5 cm from the greater trochanter tip - limit the proximal split to avoid injuring it; partial gluteus maximus denervation is most associated with the posterior approach.
- Reassurance: in primary THA the clinical sequelae of partial gluteal denervation are usually not significant, but the anatomy still guides a careful, 'safe-split' approach.
- Also at risk in sacral/pelvic surgery and deep gluteal procedures around the greater sciatic foramen.
Two points distinguish the inferior gluteal nerve in the exam and in theatre. First, its injury produces a GLUTEUS MAXIMUS LURCH - a backward thrust of the trunk in stance to keep the centre of gravity behind the hip - together with weak hip extension (trouble rising from a chair, on stairs, and running) and buttock atrophy, and it must NOT be confused with the Trendelenburg gait of superior gluteal nerve (abductor) injury. Second, because the nerve enters the deep surface of gluteus maximus about 5 cm from the tip of the greater trochanter, the posterior approach to the hip must respect this 'safe split': parting the muscle more than ~5 cm proximal to the greater trochanter risks dividing the nerve before it is visualised. Knowing that the inferior gluteal nerve exits below piriformis and is the sole supply of gluteus maximus is what underlies both the clinical sign and the surgical precaution.
Examining Gluteus Maximus and the Differential of Weak Hip Extension
Testing the muscle and placing the deficit in a differential is the clinical counterpart of the anatomy.
- Isolated power test: patient prone with the knee flexed to 90 degrees (this slackens the hamstrings so they cannot substitute as hip extensors), then ask them to lift the thigh off the couch against resistance - this isolates gluteus maximus.
- Inspect/palpate for buttock flattening and atrophy; compare sides.
- Gait: the gluteus maximus lurch is a posterior trunk thrust at heel-strike, bringing the line of gravity behind the hip so the weak extensor is not needed - distinct from the lateral trunk lurch/Trendelenburg of abductor (superior gluteal nerve) weakness.
- Isolated inferior gluteal nerve palsy: pure motor maximus weakness, no sensory loss, normal hamstrings and ankle.
- S1 radiculopathy: added sensory loss (posterolateral leg/sole), a reduced ankle jerk and plantarflexion weakness, with back/leg pain (developed in the lumbar-radiculopathy topic).
- Proximal sciatic nerve / sacral plexus lesion: a wider deficit - hamstrings and the sciatic distribution (foot drop, sensory loss) involved alongside the maximus.
- Hamstring injury: knee-flexion weakness with hip extension largely preserved by the maximus (developed in the hamstring-injury topics).
To test gluteus maximus in isolation, examine the patient prone with the knee bent - this removes the hamstrings' contribution to hip extension, so residual extension power is the maximus. The gluteus maximus lurch (trunk thrown backwards at heel-strike) signals inferior gluteal nerve / maximus weakness, whereas the trunk thrown sideways over the stance leg (Trendelenburg) signals superior gluteal nerve / abductor weakness. If the weak extension comes with sensory loss, a reduced ankle reflex or distal weakness, look beyond the nerve to an S1 root or a proximal sciatic/sacral-plexus lesion.
Mnemonics & Memory Aids
IGN
Hook:IGN: Inferior to piriformis / Innervates gluteus maximus, Gluteus maximus extends the hip (lurch if injured), Near the GT (~5 cm safe split).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the inferior gluteal nerve and the effect of injuring it.”
Origin & course
- Sacral plexus (L5, S1, S2); purely motor (no cutaneous branch)
- Exits greater sciatic foramen BELOW piriformis
- Enters the deep surface of gluteus maximus (its sole motor supply)
Function
- Gluteus maximus = principal hip extensor (from flexion: rising/stairs/running)
- Lateral rotator; upper fibres assist abduction (via IT band)
- Powers powerful hip extension
Injury
- Weak hip extension (rising from chair, stairs, running)
- Gluteus maximus lurch (backward trunk thrust) + buttock atrophy
- NOT Trendelenburg (that is superior gluteal nerve/abductors)
Surgical relevance
- Enters gluteus maximus ~5 cm from the greater trochanter tip
- Posterior hip approach: limit the split to <~5 cm from the GT (safe split)
- Posterior approach most associated with gluteus maximus partial denervation
Evidence & Key Studies
The course of the inferior gluteal nerve in the posterior approach to the hip
- In cadaveric dissection, the inferior gluteal nerve enters the deep surface of gluteus maximus approximately 5 cm from the tip of the greater trochanter.
- Its close relationship to the deep surface of gluteus maximus explains its susceptibility to injury during the posterior approach to the hip - it is easily damaged before it is seen if the muscle is split and parted more than 5 cm from the greater trochanter tip.
- A modified posterior approach limiting the proximal split is recommended to avoid damaging the nerve.
Lesion of gluteal nerves and muscles in THA through three surgical approaches (EMG study)
- Partial denervation of gluteus maximus was most associated with the posterior approach (about 71% of patients), whereas the transgluteal approach mostly affected gluteus medius and the anterolateral approach the superior gluteal nerve branch to tensor fasciae latae.
- The power of the hip abductors was not significantly reduced in partially denervated muscles, and clinical sequelae were not significant in primary THA.
- The approach-specific pattern of gluteal nerve/muscle lesions reflects the underlying nerve anatomy.
The inferior gluteal nerve entering the deep surface of gluteus maximus about 5 cm from the greater trochanter tip and its consequent vulnerability in the posterior approach (with the recommendation to limit the split) come from the cited Ling & Kumar cadaveric study; the approach-specific pattern of gluteal nerve/muscle denervation (posterior approach most associated with gluteus maximus denervation) and the usually insignificant clinical sequelae in primary THA from the cited Chomiak EMG study. The roots (L5-S2), the sole-motor-supply-to-gluteus-maximus, the exit below piriformis, the hip-extension function, and the gluteus maximus lurch (versus Trendelenburg) are standard, well-established anatomical teaching. (See also our Superior Gluteal Nerve and Posterior Hip Approach topics.)