Schwannoma | Meningioma | Neurofibroma | Myxopapillary Ependymoma
- Schwannoma vs Meningioma: Schwannoma is T2 hyperintense, meningioma is T2 iso/hypointense
- Dural tail sign: Suggestive of meningioma (contrast-enhancing dura adjacent to tumor)
- Dumbbell tumors: Neural foraminal extension, most commonly schwannoma (69%)
- Gross total resection: Curative for most benign IDEM tumors
- NF2 association: Multiple schwannomas/meningiomas, consider NF2 screening
- “T2 bright = schwannoma, T2 iso/dark = meningioma
- “Thoracic location + female = think meningioma
- “Dumbbell shape + cervical = think schwannoma
- “NF1 = neurofibromas, NF2 = schwannomas and meningiomas
Schwannoma: T2 hyperintense, may have cystic change, heterogeneous enhancement. Meningioma: T2 iso/hypointense, homogeneous enhancement, dural tail sign. Signal intensity ratio on T2 differentiates reliably.
Meningioma: 80% thoracic, lateral or posterolateral, 80% female. Schwannoma: Any level, often cervical/lumbar, equal gender. Ependymoma: Lumbar, filum terminale.
Neural foraminal extension creates dumbbell shape. Most common cause is schwannoma (69%). Consider stability if large extraforaminal component. May need combined anterior-posterior approach.
NF1 (von Recklinghausen): Neurofibromas, plexiform neurofibromas. NF2: Bilateral vestibular schwannomas PLUS spinal schwannomas/meningiomas. Multiple tumors = screen for NF2.
- Schwannoma
- HYPERINTENSE (bright)
- Meningioma
- Iso/HYPOINTENSE (dark)
- Schwannoma
- Heterogeneous, may be cystic
- Meningioma
- Homogeneous
- Schwannoma
- Absent/rare
- Meningioma
- Present (64%)
- Schwannoma
- Any level, cervical common
- Meningioma
- 80% thoracic
- Schwannoma
- M = F
- Meningioma
- 80% female
- Schwannoma
- Common (29%)
- Meningioma
- Rare (3%)
- Schwannoma
- Common (96%)
- Meningioma
- Rare (24%)
- Schwannoma
- Yes (displaced/encased)
- Meningioma
- No (dural origin)
- Compartment
- IDEM
- Discriminating Features
- T2 bright, cystic, foraminal extension, eccentric to root
- Key Pitfall
- Mistaking for neurofibroma when solitary
- Compartment
- IDEM
- Discriminating Features
- T2 iso/dark, broad dural base, dural tail, thoracic, female
- Key Pitfall
- Calcified plaque mimicking bone lesion
- Compartment
- IDEM
- Discriminating Features
- Target sign, nerve fibres pass through tumor, NF1, plexiform
- Key Pitfall
- Plexiform lesion harbouring MPNST
- Compartment
- IDEM (filum)
- Discriminating Features
- Filum terminale, sausage-shaped, mucin, may bleed
- Key Pitfall
- Piecemeal removal causing CSF seeding
- Compartment
- Intramedullary
- Discriminating Features
- Cord expansion, central location, syrinx
- Key Pitfall
- Calling an intramedullary tumor IDEM
- Compartment
- IDEM (multiple)
- Discriminating Features
- Multiple nodules, nerve-root coating, sugar-coating
- Key Pitfall
- Single deposit mimicking primary tumor
- Compartment
- IDEM
- Discriminating Features
- CSF signal, no enhancement, cord displacement
- Key Pitfall
- Cyst masquerading as cystic schwannoma
- Compartment
- Extradural
- Discriminating Features
- Bone destruction, epidural soft tissue, restricted diffusion (abscess)
- Key Pitfall
- Missing infection in a diabetic patient
IDEMIDEM Tumors - By Frequency
Hook:SMNE - Schwannoma Most common, Neurofibromas with NF1, Ependymoma at filum
NF1NF1 vs NF2 Features
Hook:NF1 = Neurofibromas (type 1), NF2 = schwannomas times 2 (bilateral)
Overview and Epidemiology
Intradural extramedullary (IDEM) tumors are located within the dural sac but outside the spinal cord parenchyma. They account for 55-75% of all intradural spinal tumors and are predominantly benign.
Distribution of IDEM Tumors:
- Frequency
- 40%
- Peak Age
- 30-60
- Gender
- M = F
- Frequency
- 25%
- Peak Age
- 40-70
- Gender
- F more than M (4:1)
- Frequency
- 15%
- Peak Age
- 30-50
- Gender
- M = F
- Frequency
- 10%
- Peak Age
- 20-40
- Gender
- M more than F
- Frequency
- 10%
- Peak Age
- Variable
- Gender
- Variable
Key Epidemiological Points:
Meningiomas show strong female predominance (80%) and thoracic predilection. Schwannomas affect males and females equally and occur at any spinal level. Ependymomas of the filum terminale (myxopapillary type) are the most common primary tumor of the conus/cauda equina region.
If a patient presents with multiple schwannomas or meningiomas, screen for Neurofibromatosis Type 2. NF2 is characterized by bilateral vestibular schwannomas and multiple spinal tumors. Chromosome 22 mutation.
Pathophysiology
Tumor Origins
Nerve Sheath Origin
Schwannomas arise from Schwann cells of spinal nerve roots. They are encapsulated tumors that displace rather than infiltrate nerve fibers.
- Antoni A areas: Cellular, organized palisading (Verocay bodies)
- Antoni B areas: Loose, myxoid, less cellular
- S-100 protein positive
- Eccentric growth from nerve root
- Nerve fibers displaced around capsule
- Usually single nerve root involved
- Nerve can often be preserved at surgery
Malignant transformation is extremely rare in sporadic schwannomas but may occur in NF2.
Classification
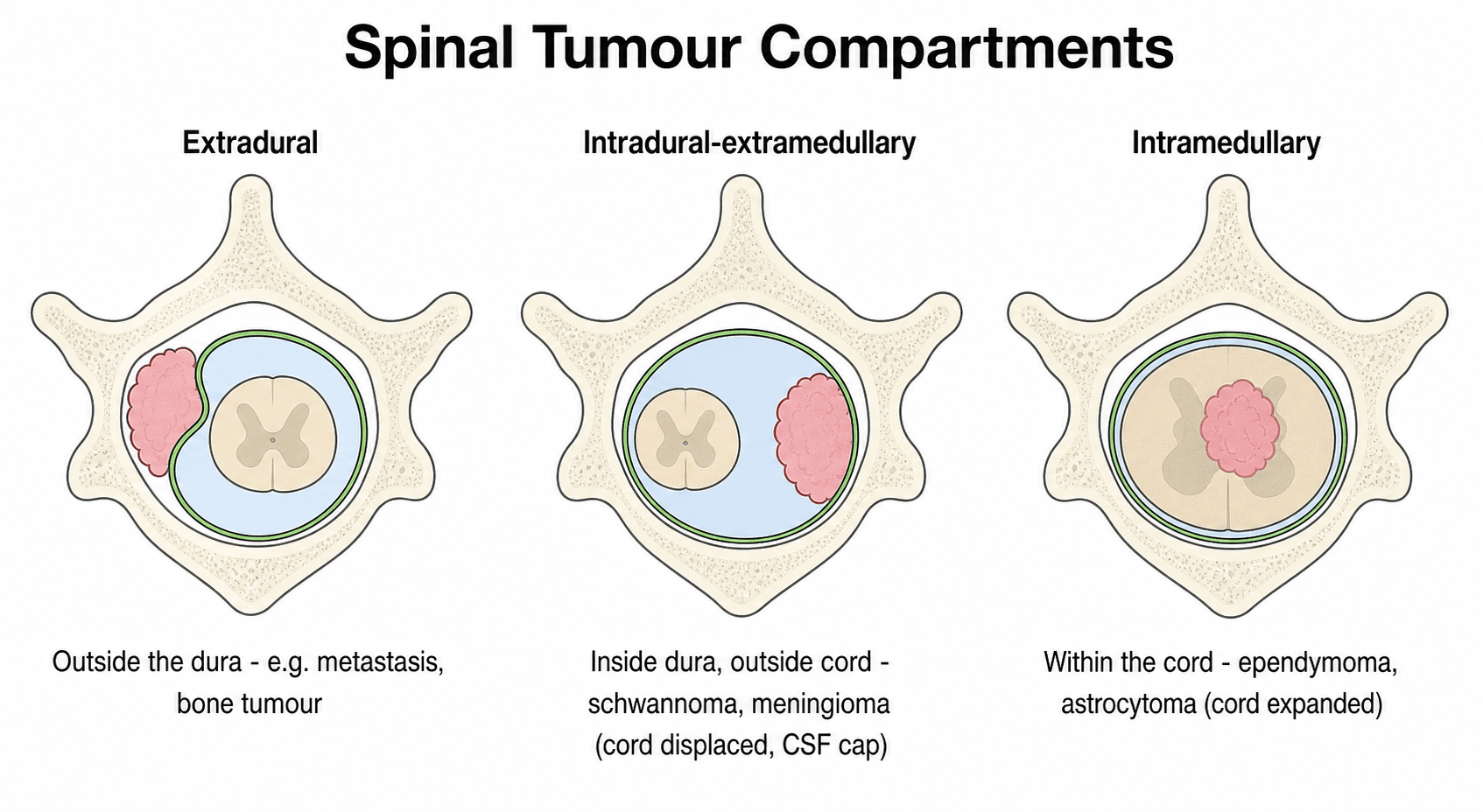
Spinal Tumor Compartments
- Location
- Outside dura
- Common Tumors
- Metastases, primary bone tumors
- Location
- Inside dura, outside cord
- Common Tumors
- Schwannoma, meningioma, neurofibroma
- Location
- Within spinal cord
- Common Tumors
- Ependymoma, astrocytoma, hemangioblastoma
IDEM tumors displace the spinal cord rather than infiltrate it. This generally allows preservation of cord function with surgical resection.
Clinical Presentation
Presenting Symptoms
- Localized back pain (70%)
- Radicular pain following nerve root distribution
- May precede neurological deficit by months to years
- Night pain common
- Sensory changes (numbness, paresthesias)
- Motor weakness (progressive)
- Bladder/bowel dysfunction (late)
- Gait disturbance
Tumor-Specific Presentations
- Radicular pain in dermatomal distribution
- May have sensory loss in affected root
- Motor weakness if motor root involved
- Often presents with progressive myelopathy
- Gait disturbance, spasticity
- Brown-Sequard syndrome if lateral compression
- May have minimal radicular symptoms
- Low back pain
- Cauda equina symptoms (bowel/bladder, saddle anesthesia)
- Often long history before diagnosis
Examination Findings
- Spasticity, hyperreflexia below lesion
- Positive Babinski
- Clonus
- Weakness in myotomal distribution
- Hyporeflexia at affected level
- Muscle atrophy
Tumors of the lumbar spine may cause cauda equina syndrome with saddle anesthesia, urinary retention, and bilateral leg weakness. This is a surgical emergency requiring urgent decompression.
Investigations
MRI - Gold Standard
Standard Sequences
Essential for IDEM tumor assessment.
- Tumors usually isointense to cord
- Defines anatomical relationships
- Pre-contrast baseline
- Schwannoma: Hyperintense
- Meningioma: Iso/hypointense
- Key differentiating sequence
- Shows cord edema
- All IDEM tumors enhance
- Schwannoma: Heterogeneous
- Meningioma: Homogeneous + dural tail
Whole spine MRI to exclude skip lesions or NF2.
Additional Investigations
- Bone erosion (dumbbell tumors)
- Calcification (meningioma)
- Pre-operative planning
- Routine pre-operative workup
- Consider genetic testing if NF suspected

Management
Surgical Management
Standard Posterior Approach
Most IDEM tumors approached posteriorly.
- Laminectomy: Standard approach
- Laminoplasty: May reduce post-laminectomy kyphosis
- Consider instrumented fusion if extensive laminectomy (3+ levels)
- Posterior midline incision
- Laminectomy/laminoplasty
- Durotomy (midline or paramedian)
- Tumor identification
- Microsurgical resection
- Watertight dural closure
- Bone replacement if laminoplasty
Intraoperative neurophysiological monitoring (SSEP, MEP) recommended.
Non-Surgical Management
- Small, asymptomatic tumors
- Elderly or medically unfit patients
- Slow-growing tumors (serial MRI monitoring)
- Rarely used for benign IDEM tumors
- Consider for recurrent/incompletely resected meningioma
- SRS (stereotactic radiosurgery) for small recurrences
- Primary treatment if patient not surgical candidate
For schwannomas, the parent nerve root can often be preserved because the tumor displaces rather than infiltrates nerve fibers. For neurofibromas, nerve fibers pass through the tumor, and root sacrifice is often necessary for complete resection.
Calcified and Ventral Meningioma: The Difficult Subset
Most spinal meningiomas are soft, posterolateral, WHO Grade I lesions that are gross totally resected in 85-95 percent of cases. A minority behave very differently, and recognising them preoperatively changes the consent and the surgical plan.
- Surgical challenge
- The spinal cord lies between the surgeon and the tumour, so aggressive dural resection risks cord injury
- Strategy
- Often accept Simpson Grade II (coagulate the dural attachment) over a hazardous Grade I; consider a more lateral approach and gentle cord handling
- Surgical challenge
- Hard, adherent and cannot be debulked or rolled off the cord; higher rate of subtotal resection and neurological worsening
- Strategy
- Ultrasonic aspirator, patient piecemeal removal, leave an adherent calcified plaque rather than injure the cord
- Surgical challenge
- Can mimic a bony lesion or ossification and be under-recognised as a meningioma
- Strategy
- CT to characterise calcification; correlate with the dural-based enhancing mass on MRI
These features explain why a ventral calcified thoracic meningioma carries a higher recurrence and complication rate than the typical posterolateral lesion, and why surgeons trade a slightly higher recurrence risk (Simpson II) for cord safety.
For a ventral or ventrolateral calcified thoracic meningioma, do not chase a Simpson Grade I dural excision across the front of the cord. Coagulating the dural attachment (Grade II) accepts a marginally higher recurrence rate in exchange for avoiding catastrophic cord injury - the right trade-off when the dura is ventral.
MRISchwannoma vs Meningioma MRI
Hook:SCHMD - Schwannoma is bright, Cystic, Heterogeneous; Meningioma is Dark with Dural tail
Spinal Stability and Post-Laminectomy Deformity
Resecting an IDEM tumour requires a laminectomy or laminoplasty, and the posterior approach itself can destabilise the spine. Post-laminectomy kyphosis (a swan-neck deformity in the cervical spine) is the chief late mechanical problem, so deciding when to add instrumented fusion is part of operative planning.
- Why it destabilises
- Loss of the posterior tension band over a long segment
- Action
- Strongly consider instrumented fusion or laminoplasty
- Why it destabilises
- Facet joints are key stabilisers; unilateral complete facetectomy is destabilising
- Action
- Add fusion, especially with a large extraforaminal component
- Why it destabilises
- High mechanical demand and transition in alignment
- Action
- Lower threshold to fuse
- Why it destabilises
- Highest rate of post-laminectomy kyphosis
- Action
- Favour laminoplasty; close deformity surveillance
- Why it destabilises
- Surgery unmasks or worsens it
- Action
- Correct and stabilise as indicated
Laminoplasty (replacing the lamina rather than removing it) preserves the posterior tension band and may reduce kyphosis, and is particularly favoured in children and across the cervical spine.
The highest risk of post-laminectomy kyphosis is in children and after cervical laminectomy. Preserve the facet joints where possible, favour laminoplasty over laminectomy in these groups, and add instrumented fusion when the laminectomy is long, crosses a junction, or requires more than half a facet.
Management Algorithm

Complications
Surgical Complications
- CSF leak (most common, 5-10%)
- Wound infection
- New neurological deficit (2-5%)
- Hematoma
- Post-laminectomy kyphosis
- Tumor recurrence
- Chronic pain
- Arachnoiditis
CSF Leak Prevention
- Meticulous dural closure
- Dural grafting if primary closure not possible
- Fibrin sealant augmentation
- Watertight closure in layers
- Wound care
- Lumbar drain (3-5 days)
- Re-exploration if conservative measures fail
Recurrence Rates
- GTR Recurrence
- Less than 5%
- STR Recurrence
- 30-40%
- GTR Recurrence
- 5-10%
- STR Recurrence
- 20-30%
- GTR Recurrence
- Variable
- STR Recurrence
- Higher with NF1
- GTR Recurrence
- Less than 10%
- STR Recurrence
- 50-70%
Guidelines, Registries & Global Practice
Global Epidemiology
IDEM tumors comprise roughly 55-75% of all intradural spinal tumors. Incidence of primary spinal tumours overall is about 0.5-2.5 per 100,000 person-years. Schwannoma and meningioma together account for the majority; spinal meningioma shows a 3:1 to 4:1 female predominance with a thoracic predilection, while nerve sheath tumours are evenly distributed by sex and across spinal levels. Myxopapillary ependymoma is the commonest tumour of the conus/filum and presents in young adults.
Society Guidance & Frameworks (side by side)
- Scope
- Histopathology
- Practical recommendation
- Grades schwannoma/meningioma/neurofibroma (Gr I), atypical meningioma (Gr II); myxopapillary ependymoma reclassified to WHO Grade 2
- Scope
- Meningioma
- Practical recommendation
- Surgery first-line for symptomatic lesions; radiotherapy for atypical/incompletely resected disease
- Scope
- Ependymoma
- Practical recommendation
- Maximal safe resection; adjuvant RT after subtotal resection or anaplastic histology
- Scope
- Suspected spinal tumour / cord compression
- Practical recommendation
- Urgent whole-spine MRI and specialist referral for new myelopathy or cauda equina features
- Scope
- NF2-related schwannomatosis
- Practical recommendation
- Coordinated genetics, audiology, ophthalmology; consider bevacizumab for progressive vestibular schwannoma
There is no single arthroplasty-style registry for IDEM tumours; outcome evidence derives from institutional series, the Rare Cancer Network (myxopapillary ependymoma) and national cancer/CNS-tumour registries (e.g. CBTRUS in the US) which inform incidence and survival rather than implant survival.
High- vs Limited-Resource Practice Variation
In well-resourced centres, microsurgery with the operating microscope, intra-operative neurophysiological monitoring (SSEP/MEP/D-wave), ultrasonic aspiration and ready access to MRI surveillance underpin gross total resection rates comparable to international centres of excellence. In limited-resource settings, delayed presentation with established myelopathy is common, monitoring may be unavailable, and emphasis shifts to timely decompression and watertight closure to limit CSF leak. Genetic testing and dedicated NF2/schwannomatosis multidisciplinary clinics are concentrated in tertiary referral networks; telemedicine and regional referral pathways help extend specialist input where local capacity is limited.
Controversies & Areas of Uncertainty
1. Laminectomy vs laminoplasty vs instrumented fusion. Whether laminoplasty or routine instrumentation reduces post-operative deformity remains unsettled. Most series reserve fusion for multilevel laminectomy (3 or more levels), the cervicothoracic/thoracolumbar junctions, pre-existing deformity, and paediatric patients in whom post-laminectomy kyphosis is far more common.
2. Nerve root sacrifice in nerve sheath tumors. Traditional teaching preserves the parent root; contemporary data (Vandenbulcke et al., 2023) suggest the involved root in foraminal/dumbbell tumors is frequently non-functional and can be sacrificed to achieve gross total resection with a low risk of clinically significant deficit. Intra-operative stimulation to confirm a non-eloquent root is the pragmatic compromise.
3. Extent of dural handling for meningioma. Simpson Grade I (dural excision and duraplasty) lowers recurrence versus Grade II (coagulation only) but raises the risk of CSF leak and cord injury when the dura is ventral. Many surgeons accept Grade II for ventral/ventrolateral thoracic meningiomas where aggressive dural resection is hazardous.
4. Role of radiosurgery. Stereotactic radiosurgery is increasingly used for residual/recurrent meningioma and schwannoma and for NF2 tumors, but long-term spinal cord tolerance data are limited; surgery remains first-line for symptomatic compressive lesions.
5. Surveillance versus treatment of small asymptomatic tumors. Incidental small IDEM tumors (especially in NF2) are often observed with serial MRI; growth rate and symptom development, rather than size alone, drive the decision to operate.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman presents with 6 months of progressive gait difficulty and band-like thoracic pain. MRI shows a T6-T7 intradural extramedullary mass that is isointense on T2, enhances homogeneously, and has a dural tail sign.”
“A 45-year-old man presents with right-sided neck pain and C6 radiculopathy. MRI shows a C5-C6 intradural extramedullary tumor that is T2 hyperintense with heterogeneous enhancement. There is foraminal extension with an extraspinal component.”
“A 28-year-old man presents with 18 months of low back pain and recent onset of urinary hesitancy. MRI shows a well-circumscribed L3-L4 intradural tumor arising from the filum terminale. It is T2 hyperintense with homogeneous enhancement.”
“A 32-year-old woman presents with progressive gait ataxia. MRI shows three intradural extramedullary tumors at C3, T6, and L2. She also reports hearing loss for 2 years.”
Schwannoma vs Meningioma
- Schwannoma: T2 BRIGHT, heterogeneous, cystic, foraminal extension
- Meningioma: T2 ISO/DARK, homogeneous, dural tail, thoracic
- Signal intensity ratio on T2 reliably differentiates
- Schwannoma = any level, Meningioma = 80% thoracic
Tumor Frequencies
- Schwannoma: 40% (most common)
- Meningioma: 25% (80% female)
- Neurofibroma: 15% (NF1 associated)
- Myxopapillary ependymoma: 10% (filum terminale)
Surgical Goals
- GTR is curative for most IDEM tumors
- Schwannoma: Nerve preservation often possible
- Meningioma: Simpson Grade II (GTR + dural excision)
- Ependymoma: EN BLOC essential (capsule violation = seeding)
Dumbbell Tumors
- 69% are schwannomas
- Eden Classification: I-III based on extension
- Combined approach may be needed
- Assess stability if facetectomy required
NF Association
- NF1: Neurofibromas, plexiform, cafe-au-lait, chr 17
- NF2: Schwannomas + meningiomas, bilateral VS, chr 22
- Multiple spinal tumors = screen for NF2
- NF2 requires multidisciplinary approach
Complications
- CSF leak most common (5-10%)
- Post-laminectomy kyphosis (consider fusion if 3+ levels)
- Recurrence: GTR less than 5-10%, STR 30-40%
- Neurological deficit rare with microsurgical technique
Evidence Base
T2 Signal Intensity Ratio Differentiates Schwannoma from Meningioma
- 20 schwannomas vs 20 meningiomas, pathology-proven IDEM tumors
- Tumor-to-fat T2 signal-intensity ratio significantly higher in schwannoma (p=0.002)
- Optimal SI-ratio cutoff 0.420 (sensitivity 80%, specificity 70-75%)
- Area under ROC curve 0.78 for both independent readers
Long-Term Outcome After Spinal Schwannoma Removal
- 187 surgically treated spinal schwannomas, median follow-up 12.9 years
- Life expectancy equivalent to the general population
- Late complications in 21%: arachnoiditis (6%), spinal deformity (6%), cystic myelopathy (2%)
- Residual local pain (46%) and radiating pain (43%) were the commonest late complaints
Spinal Meningiomas: Surgical Management and Outcome
- Single-institution series plus pooled review of 556 patients from six large series
- Spinal meningiomas can be completely resected in most cases
- Surgery associated with postoperative functional improvement
- Low recurrence rate after complete resection
Long-Term Outcome of Spinal Myxopapillary Ependymoma (Rare Cancer Network)
- 183 patients across MD Anderson and the Rare Cancer Network
- Estimated 10-year overall survival 92.4%; 10-year progression-free survival 61.2%
- Treatment failure in ~32%, predominantly local (27%) but distant spinal/brain relapse in 9-6%
- Extent of surgery and use of adjuvant radiotherapy were independent prognostic factors
Nerve Root Sacrifice for Foraminal/Dumbbell Nerve Sheath Tumors
- 26 foraminal/dumbbell benign nerve sheath tumors; involved root routinely sacrificed
- Gross total resection achieved in 84.6%
- Functional motor roots (C5-T1, L3-S1) involved in 14 cases
- Persistent new or worsened motor deficit in only 1/9 and 1/5 patients respectively at follow-up
References
- Takashima H, Takebayashi T, Yoshimoto M, et al. Differentiating spinal intradural-extramedullary schwannoma from meningioma using MRI T2 weighted images. Br J Radiol. 2018;91(1092):20180262. doi:10.1259/bjr.20180262. PMID 30052467.
- Seppala MT, Haltia MJ, Sankila RJ, et al. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg. 1995;83(4):621-6. doi:10.3171/jns.1995.83.4.0621. PMID 7674010.
- Gottfried ON, Gluf W, Quinones-Hinojosa A, et al. Spinal meningiomas: surgical management and outcome. Neurosurg Focus. 2003;14(6):e2. doi:10.3171/foc.2003.14.6.2. PMID 15669787.
- Weber DC, Wang Y, Miller R, et al. Long-term outcome of patients with spinal myxopapillary ependymoma: treatment results from the MD Anderson Cancer Center and institutions from the Rare Cancer Network. Neuro Oncol. 2015;17(4):588-95. doi:10.1093/neuonc/nou293. PMID 25301811.
- Vandenbulcke A, D'Onofrio GF, Capo G, et al. Sacrifice of involved nerve root during surgical resection of foraminal and/or dumbbell spinal neurinomas. Brain Sci. 2023;13(1):109. doi:10.3390/brainsci13010109. PMID 36672090.