Nightstick Fracture | Direct Blow | Nonoperative vs ORIF
TREATMENT DECISION
Critical Must-Knows
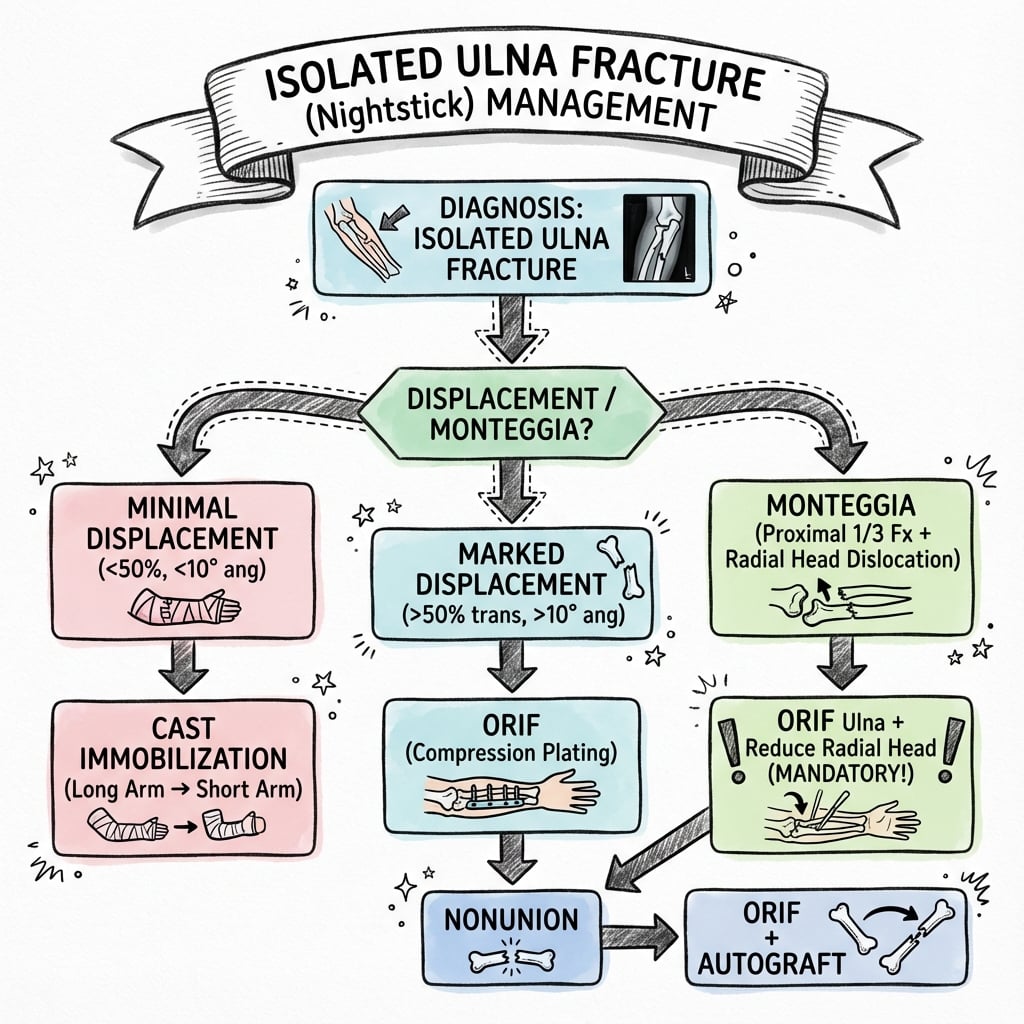
- Nightstick fracture = isolated ulna shaft from direct blow (defensive mechanism)
- EXCLUDE Monteggia (check radial head position on all views)
- Nonoperative threshold: less than 50% displacement, less than 10° angulation
- ORIF with 3.5mm DCP plate - 6+ cortices each side
- High union rate both operative and nonoperative
Clinical Pearls
- "ALWAYS check PRUJ - rule out Monteggia lesion
- "Functional bracing allows early motion
- "Plate fixation is gold standard for displaced
- "Refracture risk higher with plate removal
Critical Exam Concepts
Rule Out Monteggia
ALWAYS check radial head. An isolated ulna fracture is NOT Monteggia. Get proper views including elbow. A line through radial neck should bisect capitellum on ALL views (radiocapitellar line).
Direct Blow History
Classic mechanism. Patient raises arm to defend against blow (assault, fall onto object). The subcutaneous position of the ulna makes it vulnerable. Ask about mechanism carefully.
Nonoperative Criteria
Strict criteria. Less than 50% displacement, less than 10° angulation in proximal 2/3 or less than 15° in distal 1/3. Middle/distal third location. Functional brace allows early motion.
ORIF Threshold
Greater than 50% displacement or significant angulation. Use 3.5mm DCP plate with 6+ cortices each side. Compression plating standard technique.
Isolated Ulna Fracture Quick Decision
| Displacement | Angulation | Location | Treatment |
|---|---|---|---|
| Less than 50% | Less than 10° | Middle/distal | Functional brace |
| 50% | 10-15° | Any | Borderline - consider ORIF |
| Greater than 50% | Greater than 15° | Proximal | ORIF recommended |
| Any | Any | Open fracture | ORIF + debridement |
NIGHTNightstick Fracture Features
| N | Not Monteggia Confirm radial head located |
| I | Isolated ulna Single bone injury |
| G | Guard position Defensive arm raised |
| H | Hit directly Direct blow mechanism |
| T | Treatment by displacement Brace or ORIF |
| N | Not Monteggia Confirm radial head located | H | Hit directly Direct blow mechanism |
| I | Isolated ulna Single bone injury | T | Treatment by displacement Brace or ORIF |
| G | Guard position Defensive arm raised |
Hook:NIGHT stick fracture from a NIGHT time assault!
PLATEORIF Indications
| P | Proximal third Higher union issues |
| L | Large displacement (greater than 50%) Unstable pattern |
| A | Angulation greater than 15° Malunion risk |
| T | Two bone involvement Not truly isolated |
| E | Expected compliance poor Brace won't work |
| P | Proximal third Higher union issues | T | Two bone involvement Not truly isolated |
| L | Large displacement (greater than 50%) Unstable pattern | E | Expected compliance poor Brace won't work |
| A | Angulation greater than 15° Malunion risk |
Hook:PLATE the ulna when criteria met!
SAFENonoperative Criteria
| S | Stable pattern Less than 50% displacement |
| A | Angulation minimal Less than 10-15 degrees |
| F | Functional brace compliant Patient can manage |
| E | Exclude Monteggia Radial head in joint |
| S | Stable pattern Less than 50% displacement | F | Functional brace compliant Patient can manage |
| A | Angulation minimal Less than 10-15 degrees | E | Exclude Monteggia Radial head in joint |
Hook:SAFE for functional bracing!
Overview and Epidemiology
Why 'Nightstick' Fracture?
Historical name. Called nightstick fracture because the mechanism is typically a direct blow to the raised forearm, as when defending against an assault with a nightstick (baton). The subcutaneous ulna border is vulnerable to direct impact.
Epidemiology
- 2-5% of forearm fractures
- Bimodal: young males (assault), elderly (falls)
- More common in males
- Middle to distal third most common
Mechanism
- Direct blow to subcutaneous ulna border
- Defensive arm position (guard)
- Fall onto hard edge
- Sports (hockey stick, bat)
Anatomy and Biomechanics
Ulna Shaft
Position: The posterior border is subcutaneous throughout its length, making it vulnerable to direct trauma.
Cross-section: Triangular proximally, becomes more rounded distally.
Interosseous membrane: Connects ulna to radius. Important for load transfer and forearm stability. Disruption creates longitudinal instability (Essex-Lopresti).
Classification
OTA/AO Classification
22-A1: Simple fracture of ulna only.
22-B1: Wedge fracture of ulna only.
22-C1: Complex fracture of ulna only.
The classification guides complexity but treatment is primarily based on displacement and angulation.
Clinical Assessment
History
- Mechanism (direct blow vs fall)
- Assault or accident
- Location and timing of impact
- Previous forearm injury
- Hand dominance
Examination
- Inspect for deformity, swelling
- Palpate entire ulna and radius
- Check DRUJ and PRUJ
- Test forearm rotation
- Neurovascular exam
Must Exclude Monteggia
An isolated ulna fracture is NOT a Monteggia lesion. Always check the proximal radioulnar joint (PRUJ). The radiocapitellar line (line through radial shaft/neck) should bisect the capitellum on ALL views. If the radial head is dislocated, it is a Monteggia fracture-dislocation, not an isolated ulna fracture.
Differential Diagnosis
Distinguishing Isolated Ulnar Shaft Fracture from Mimics
| Diagnosis | Key Distinguishing Feature | Pitfall if Missed |
|---|---|---|
| Isolated ulnar shaft fracture | Single ulna fracture, radiocapitellar line intact, DRUJ congruent | — |
| Monteggia fracture-dislocation | Ulna fracture PLUS radial head dislocation (radiocapitellar line broken) | Missed radial head dislocation leads to chronic instability and poor function |
| Both-bone forearm fracture | Radius AND ulna both fractured | Treating as isolated underestimates instability |
| Galeazzi fracture | Radial shaft fracture with DRUJ disruption (not ulnar shaft) | Different injury; DRUJ must be reduced |
| Essex-Lopresti injury | Radial head fracture, IOM disruption, DRUJ instability (longitudinal) | Missed longitudinal forearm instability |
| Pathological fracture | Low-energy mechanism, lytic/sclerotic lesion on imaging | Fixing without addressing underlying lesion |
Investigations
Essential Views
Forearm AP and Lateral: Both bones, full length.
Include elbow: Essential to assess radiocapitellar alignment and exclude Monteggia.
Include wrist: Assess DRUJ for longitudinal instability.
Measurements: Displacement as percentage of bone width, angulation in degrees.
Management
Functional Bracing
Indications: Less than 50% displacement, less than 10° angulation (proximal/middle), less than 15° angulation (distal), intact radiocapitellar joint.
Protocol: Initial long-arm splint 1-2 weeks. Convert to functional brace. Allow elbow and wrist motion. Serial X-rays at 2, 4, 6 weeks.
Expected outcomes: Union in 8-12 weeks. Good functional results if criteria met.
Failure: If displacement increases or patient non-compliant, convert to ORIF.
Functional Bracing Rationale
Why functional bracing works: The interosseous membrane and surrounding soft tissues provide stability. Early motion prevents stiffness while allowing fracture healing through micromotion. The ulna is primarily a stabilizer (not weight-bearing like radius), so moderate displacement is tolerated.
Advantages
- Avoids surgery complications
- Lower infection risk
- Early joint motion
- Cost-effective
- No hardware removal needed
Requirements
- Patient compliance critical
- Regular follow-up essential
- Serial radiographs needed
- Accept some residual deformity
- Longer time to union
Plate Removal Consideration
Refracture after plate removal is a recognized complication (up to 20% in some series). Counsel patients about this risk. If removing plate, protect arm for 6-12 weeks after removal.
Surgical Technique
Posterior Approach to Ulna
Position: Supine with arm across chest, or lateral with arm on table.
Incision: Direct posterior over subcutaneous ulna border.
Internervous plane: Between ECU (posterior interosseous) and FCU (ulnar nerve). The ulna is subcutaneous - minimal dissection needed.
Key structure: Ulnar nerve is anterior and does not need to be identified for shaft fractures.
Complications
| Complication | Incidence | Management |
|---|---|---|
| Nonunion | 5-10% (nonoperative) | ORIF with bone graft |
| Malunion | Variable | Osteotomy if symptomatic |
| Refracture post plate removal | Up to 20% | Protect arm, consider leaving plate |
| Infection | 1-2% (operative) | Antibiotics, debridement |
| Hardware prominence | Common | Plate removal after union |
Postoperative Care
Rehabilitation Protocol
Splint or brace. Wound care. Finger and shoulder ROM.
Begin elbow and wrist ROM. Gentle forearm rotation. Sling for comfort.
Full ROM goal. Light strengthening. X-ray to confirm healing.
Progressive strengthening. Return to work based on healing. Sports at 4-6 months.
Outcomes and Prognosis
Outcome Factors
Favorable: Distal third, minimal displacement, good compliance, anatomic reduction.
Unfavorable: Proximal third, comminution, delayed treatment, smoking.
Controversies and Areas of Uncertainty
The 50% / 10° Threshold
The classic nonoperative criteria (under 50% displacement, under 10° angulation) come from Sarmiento-era series. Newer data (Coulibaly 2015) link angulation of 8° or more and any secondary displacement to malunion, nonunion and failure to return to prior activity, suggesting the traditional limits may be too permissive for active patients.
Moderately Displaced Fractures
Fractures near the 50% threshold are genuinely contested. Ali (2019) reported 5 of 10 nonoperative cases failed, yet operative treatment adds surgical and hardware risk. No RCT resolves this; decisions are individualised by age, demand, compliance and follow-up reliability.
Routine Bone Grafting
Anderson's historical recommendation to graft minor comminution is no longer supported: Ring (2005) found bone grafting did not reduce nonunion in comminuted forearm fractures. Bridge plating with biological technique is now preferred.
Plate Removal
Whether to remove a subcutaneous, prominent ulnar plate is debated. Removal relieves symptoms but carries a refracture risk concentrated at the plate ends; many surgeons leave asymptomatic plates in situ and, if removing, protect the limb afterwards.
Evidence Base and Key Studies
Functional Bracing - Landmark Series (Sarmiento)
- 444 isolated ulnar shaft fractures braced; 287 (65%) followed up
- Union in 99% of fractures; mean shortening only 1.1 mm
- Mean final radial and dorsal angulation 5° each
- Good-to-excellent function in more than 96% (greatest pronation loss in proximal-third)
Compression Plating of Forearm Diaphysis (Anderson)
- 330 acute diaphyseal radius/ulna fractures plated; 137 isolated/combined ulna fractures
- Union rate 96.3% for the ulna and 97.9% for the radius
- Established ASIF compression plating as the standard for forearm diaphyseal fractures
- Iliac bone graft used for severely comminuted patterns (later questioned)
Bone Graft Not Required for Comminution (Ring)
- 41 comminuted both-bone forearm fractures plated with 3.5/4.5 mm DCP (6+ holes)
- Nonunion in 12% (5 patients)
- Bone grafting NOT associated with lower nonunion (OR 0.98, 95% CI 0.15-6.42)
- Open fracture, multiple injury, ipsilateral injury also not significant
Operative vs Nonoperative Nightstick Outcomes (Ali)
- 52 isolated ulnar shaft fractures; 42 ORIF (incl. 6 open) vs 10 nonoperative
- 5 of 10 nonoperative cases failed and required more follow-up visits
- ORIF gave satisfactory outcome with early non-load-bearing mobilisation
- Fractures with less than 50% displacement individualised by age, function, compliance
Displacement Drives Complications (Coulibaly)
- 70 isolated ulnar shaft fractures; 33 nonoperative vs 37 ORIF
- 14 nonunions and 17 malunions overall; nonoperative significantly associated with both
- Angulation of 8° or more linked to failure to return to prior activity level
- Secondary displacement greater than 2 mm contributed to malunion and nonunion
Refracture After Plate Removal (Lindgren)
- 349 surgically fixed forearm fractures; subsequent fracture rate 5-11%
- Plate refractures 10.9% vs flexible-nail 5.1%
- 90% of plate refractures occurred at the proximal or distal plate edge
- 90% of plate refractures required revision surgery
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Nightstick Fracture
"A 28-year-old man presents after an altercation where he raised his arm to defend himself. X-rays show an isolated mid-shaft ulna fracture with 30% displacement and 5 degrees of angulation. How would you manage this?"
Scenario 2: Displaced Fracture
"A 35-year-old woman falls onto a metal railing, striking her forearm. X-rays show an isolated ulna fracture with 75% displacement and 20 degrees of angulation. How would you treat this?"
Scenario 3: Proximal Third Fracture
"An isolated ulna fracture in the proximal third with 40% displacement. The radial head is confirmed located. How would your management differ from a mid-shaft fracture?"
Scenario 4: Open Fracture
"A 42-year-old motorcyclist presents with a Gustilo grade II open isolated ulna fracture. The radial head is confirmed located. How would you manage this injury?"
MCQ Practice Points
Displacement Threshold
Q: What is the displacement threshold for nonoperative treatment of isolated ulna fractures? A: Less than 50% of bone width. Beyond this, ORIF is recommended.
Angulation Threshold
Q: What angulation is acceptable for nonoperative treatment? A: Less than 10 degrees in proximal/middle third, up to 15 degrees in distal third.
Monteggia Exclusion
Q: What must be confirmed before diagnosing an isolated ulna fracture? A: Radial head is located. Check radiocapitellar line on all views to exclude Monteggia lesion.
Plate Fixation
Q: What is the minimum fixation required for ulna shaft ORIF? A: 6 cortices (3 screws) on each side of the fracture with a 3.5mm DCP or LCP.
Refracture Risk
Q: What is a significant risk after plate removal from the ulna? A: Refracture (up to 20%). Recommend waiting 18-24 months before removal if indicated.
Nightstick Mechanism
Q: What is the mechanism of a nightstick fracture? A: Direct blow to the subcutaneous ulna border, typically when arm is raised in defense.
Guidelines, Registries & Global Practice
Global Epidemiology
- Isolated ulnar shaft fractures are uncommon (a small fraction of forearm fractures) and remain under-studied
- Bimodal: young men (assault, the classic "nightstick" mechanism) and older adults (low-energy falls)
- High-energy mechanism predominated (85.7%) in one Level I trauma-centre series of 70 cases (Coulibaly 2015)
- Mechanism varies by region: interpersonal violence in urban trauma centres, falls in ageing populations, sport elsewhere
Registry & Evidence Gap
- No dedicated arthroplasty-style registry exists for diaphyseal forearm fractures
- Evidence base is small retrospective series and case-control studies, not RCTs
- No high-level consensus on the exact operative threshold for moderately displaced fractures
- This makes individualised, shared decision-making essential
Society Guidance & Practice Comparison
| Body / Region | Position on Isolated Ulnar Shaft Fractures |
|---|---|
| AO Foundation / OTA | Classify as 2U2 (ulna diaphysis); plate compression for simple, bridge plating for comminuted; minimum 6 cortices each side |
| AAOS (US) / UK BOA practice | Nonoperative bracing for minimally displaced (under 50% displacement, under 10° angulation, radial head reduced); ORIF for displaced or proximal-third |
| EFORT / European literature | Lower angulation tolerance suggested (8° or more linked to worse function); favour fixation when displacement near threshold |
| Consistent global principle | Exclude Monteggia in every case (radiocapitellar line on dedicated elbow views) before labelling 'isolated' |
High-Resource Settings
- Prefabricated functional braces readily available for nonoperative pathway
- Locking plates (LCP) stocked for osteoporotic bone
- Early supervised hand therapy and serial imaging routine
- Day-case ORIF feasible with image intensifier
Limited-Resource Settings
- Custom moulded casts/braces substitute for prefabricated braces
- Standard (non-locking) DCP plating remains effective and lower cost
- Reliable follow-up for serial radiographs may favour definitive fixation when displacement is borderline
- Implant removal may be deferred indefinitely to conserve theatre resources and avoid refracture risk
Non-Accidental Injury
Safeguarding remains global. In a child or in any patient where the history does not match the injury, an isolated ulnar fracture should prompt consideration of non-accidental injury and appropriate safeguarding pathways, irrespective of healthcare system.
ISOLATED ULNA FRACTURES
Clinical summary
Key Features
- •Nightstick = direct blow mechanism
- •Must exclude Monteggia (check PRUJ)
- •Subcutaneous position vulnerable
- •Middle/distal third most common
Nonoperative Criteria
- •Less than 50% displacement
- •Less than 10° angulation prox/mid
- •Less than 15° angulation distal
- •Radial head located
ORIF Indications
- •Greater than 50% displacement
- •Greater than 15° angulation
- •Proximal third (lower threshold)
- •Open fractures
Operative Technique
- •Posterior approach to ulna
- •3.5mm DCP or LCP
- •6+ cortices each side
- •Lag screw if oblique
Outcomes
- •95%+ union rate (ORIF)
- •90% union rate (nonoperative)
- •Refracture risk with plate removal
- •Prox third higher complications