Post-surgical stiffness | TKA & ACL | Cyclops lesion | MUA
- Arthrofibrosis is a diagnosis of exclusion - rule out infection, component malposition/oversizing, CRPS and poor rehab first
- Driven by aberrant myofibroblasts depositing type I collagen in a proinflammatory joint; TGF-beta is the best-established pathway
- Manipulation under anaesthesia (MUA) works best early - typically within 6-12 weeks of the index surgery, before scar matures
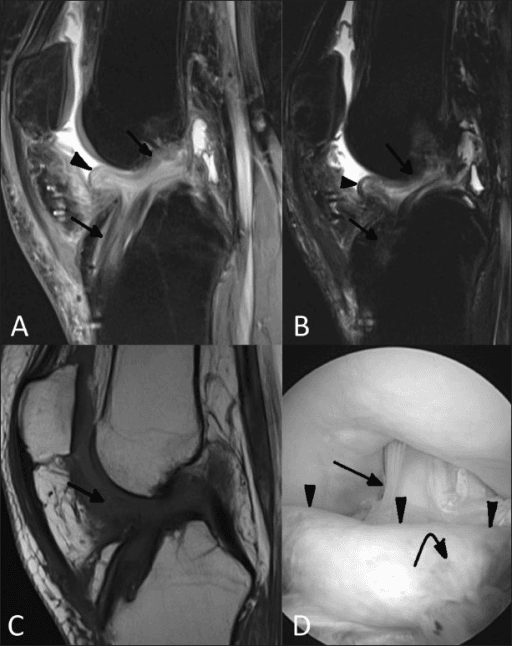
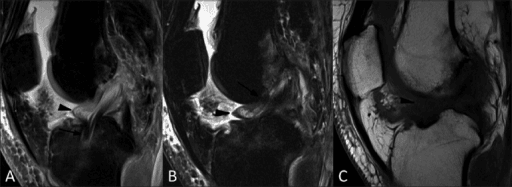
- Cyclops syndrome = fibrous nodule anterior to the ACL graft causing a painful, springy loss of terminal extension
- Prevention beats cure - good pain control, early range of motion, correct surgical technique and avoiding graft malposition
- “MUA after ~3 months is far less effective and risks fracture/extensor disruption
- “No biopsy and no biomarker confirms arthrofibrosis - it is clinical plus exclusion
- “Cyclops = LOSS OF EXTENSION; global arthrofibrosis = loss of flexion AND extension
- “Patella baja on lateral film suggests infrapatellar contracture - a poor-prognosis pattern
Never call stiffness 'arthrofibrosis' until you have excluded treatable causes. Infection, component malposition or oversizing, instability, CRPS and inadequate rehabilitation all mimic it and need different treatment.
Act on stiffness early. Manipulation under anaesthesia is most effective within roughly 6-12 weeks while the scar is immature. After 3 months it is less effective and the risk of periprosthetic fracture or extensor rupture rises.
Loss of EXTENSION after ACL reconstruction. A firm, sometimes audible/palpable block at terminal extension suggests a cyclops nodule anterior to the graft. Confirm on MRI; treat with arthroscopic excision.
Myofibroblast-driven type I collagen deposition in a proinflammatory joint, with TGF-beta as the best-established signalling pathway. No biomarker or biopsy confirms the diagnosis.
- Setting
- After TKA
- Motion Lost
- Flexion and extension
- First-line Treatment
- Therapy; MUA if early; release if late
- Setting
- After ACL reconstruction
- Motion Lost
- Terminal extension
- First-line Treatment
- Arthroscopic excision
- Setting
- After major knee surgery
- Motion Lost
- Flexion, patella baja
- First-line Treatment
- Aggressive therapy, release (poor prognosis)
- Setting
- Any (correctable cause)
- Motion Lost
- Variable
- First-line Treatment
- Treat the cause (infection/malposition)
STIFFExclude Before Diagnosing
Hook:A STIFF knee needs every other cause excluded before you blame scar.
EYESCyclops Lesion Features
Hook:The CYCLOPS has one EYE - and it blocks the knee from straightening.
TIPSDrivers of Fibrosis
Hook:TIPS for why scar forms - TGF-beta, Inflammation, Proliferation, Scar collagen.
Overview and Epidemiology
Arthrofibrosis is the formation of excessive scar tissue within and around the knee that mechanically restricts movement, causing stiffness, pain and functional loss. According to PubMed, a critical analysis review describes it after total knee arthroplasty (TKA) as new formation of excessive scar tissue producing limited range of motion, pain and functional deficits (Ramos et al., JBJS Reviews 2023; DOI).
It is best thought of as a spectrum:
- Diffuse (global) arthrofibrosis - pan-capsular scarring after arthroplasty or major trauma, losing both flexion and extension.
- Localised arthrofibrosis - most importantly the cyclops lesion after ACL reconstruction, a discrete anterior nodule that blocks extension.
- Infrapatellar contracture syndrome - dense scarring of the fat pad and patellar tendon, often with patella baja.
Why It Matters
A stiff knee is one of the most disabling outcomes after otherwise technically sound surgery. Patients cannot manage stairs, get out of chairs or walk normally, and revision for stiffness alone is notoriously unsatisfying.
Arthrofibrosis = pathological scar causing restricted motion AFTER excluding other causes of stiffness. It is a clinical diagnosis of exclusion, not a radiological or histological one.
Frequency
- After TKA, clinically significant stiffness requiring manipulation occurs in roughly 2-5% of knees in modern series.
- According to PubMed, a multimodal pain-management cohort reported manipulation rates falling from 4.75% to 2.24% with a multimodal protocol (Lavernia et al., J Arthroplasty 2008; DOI).
- After ACL reconstruction, cyclops lesions are seen in up to a quarter of second-look arthroscopies, but symptomatic cyclops syndrome is far less common - around 3-11% depending on the series.
Pathophysiology
Arthrofibrosis is fundamentally a dysregulated wound-healing response. Normal healing resolves; arthrofibrosis is healing that fails to switch off.
The Fibrotic Cascade
- Surgical/injury trigger - tissue damage and bleeding create a proinflammatory environment.
- Inflammation - cytokines recruit fibroblasts and activate them.
- Myofibroblast transformation - fibroblasts differentiate into contractile myofibroblasts.
- Excess matrix - myofibroblasts deposit large amounts of type I collagen.
- Contraction and maturation - the scar contracts and cross-links, mechanically tethering the joint.
According to PubMed, the pathophysiology is multifactorial and centres on aberrant activation and proliferation of myofibroblasts that primarily deposit type I collagen in response to a proinflammatory environment, with transforming growth factor-beta (TGF-beta) signalling the best-established pathway (Ramos et al., JBJS Reviews 2023; DOI).
TGF-beta drives the myofibroblast. It is the central, best-established profibrotic signal in knee arthrofibrosis. There is currently no validated biomarker and no diagnostic biopsy.
The Cyclops Lesion
The cyclops lesion is a localised variant. According to PubMed, second-look studies describe it as a fibroproliferative nodule arising from tibial-tunnel drilling debris, ACL stump remnants or broken graft fibres, sometimes from repeated graft impingement on the notch in terminal extension (Delince et al., Arthroscopy 1998; DOI). Its bluish, vascular arthroscopic appearance with surrounding reddish tissue ("eyes") gives it the name.
Contributory Factors
- Surgical - graft malposition or oversizing, notch impingement, retained drilling debris, overstuffed patellofemoral joint, haematoma.
- Patient - tendency to aggressive scarring, prior surgery, diabetes, lower pain threshold.
- Rehabilitation - inadequate pain control and delayed mobilisation allow scar to mature unopposed.
Classification
There is no single universally accepted classification. The most useful exam frameworks are by pattern and by whether a treatable cause is present.
By Pattern
- Key Feature
- Pan-capsular scar
- Motion Affected
- Flexion + extension
- Prognosis
- Variable
- Key Feature
- Anterior graft nodule
- Motion Affected
- Extension
- Prognosis
- Good after excision
- Key Feature
- Patella baja, fat pad scar
- Motion Affected
- Flexion mainly
- Prognosis
- Poor
- Key Feature
- Posterior contracture
- Motion Affected
- Extension
- Prognosis
- Variable
Primary vs Secondary
- Primary (idiopathic) arthrofibrosis - an exaggerated fibrotic response with no identifiable mechanical cause.
- Secondary arthrofibrosis - stiffness driven by a correctable problem (malpositioned/oversized component, instability, infection, CRPS, poor rehab). Identifying secondary causes is the single most important step because they change management completely.
Examiners want to hear you separate primary scar from secondary stiffness. Always say: "First I would exclude a treatable cause before labelling this primary arthrofibrosis."
Clinical Presentation
History
- Persistent stiffness despite a technically satisfactory operation and appropriate rehabilitation.
- Pain - often disproportionate, worse at the extremes of motion.
- Functional loss - difficulty with stairs, sit-to-stand, kneeling.
- Cyclops syndrome - after ACL reconstruction, a painful loss of full extension, sometimes with an audible or palpable clunk near terminal extension.
Examination
Document active and passive flexion and extension, and compare to the other side. Global arthrofibrosis loses both; cyclops loses terminal extension with a springy, sometimes clunking end-feel.
A warm, hot or persistently swollen knee should raise suspicion of infection or active inflammation rather than mature scar.
Assess ligamentous stability - instability mimics and aggravates stiffness, and an unstable knee will not respond to manipulation.
Check patellar height and tracking. Patella baja suggests infrapatellar contracture, a poor-prognosis pattern.
A hot, swollen, painful knee with raised inflammatory markers may be infected. Never manipulate or release a knee until infection has been excluded - manipulating a septic joint is dangerous and worsens outcomes.
Investigations
Investigations serve mainly to exclude other causes - there is no test that proves arthrofibrosis.
Bloods
- CRP, ESR, white cell count - screen for periprosthetic or septic joint infection.
- Consider joint aspiration for cell count, differential and culture if infection is suspected.
Imaging
Plain films assess component position and size, alignment, patellar height (baja) and loosening. Overstuffing of the patellofemoral joint and malrotation are key technical mimics to identify.
According to PubMed, in the TKA setting the review is explicit that imaging helps rule out specific causes of stiffness, biopsy is not indicated and no biomarkers of arthrofibrosis exist (Ramos et al., JBJS Reviews 2023; DOI).
A focal nodule anterior to the ACL graft that is low-to-intermediate signal, in a patient with loss of extension, is the radiological signature of a symptomatic cyclops lesion.
Management
Management is staged and escalating: optimise rehabilitation, then manipulation, then surgical release - and always treat any secondary cause first.
Step 1 - Prevention and Rehabilitation
- Multimodal analgesia and early aggressive physiotherapy to keep the knee moving while scar is immature.
- Address swelling, encourage extension as well as flexion, and set range-of-motion milestones.
According to PubMed, a multimodal pain-management protocol reduced the manipulation rate after TKA from 4.75% to 2.24%, supporting good analgesia as primary prevention (Lavernia et al., J Arthroplasty 2008; DOI). Adjuncts at the index operation have also been explored - according to PubMed, autologous platelet gel and fibrin sealant improved early range of motion and reduced the incidence of arthrofibrosis and forced manipulation in one controlled study (Everts et al., Knee Surg Sports Traumatol Arthrosc 2007; DOI).
Step 2 - Manipulation Under Anaesthesia (MUA)
- Indicated for diffuse stiffness that fails to progress with therapy, ideally early (within ~6-12 weeks).
- Performed gently under full muscle relaxation with the hand close to the joint to minimise lever-arm forces.
MUA is most effective early while scar is immature. Performed late (after ~3 months) it is less effective and carries a real risk of periprosthetic fracture, patellar tendon avulsion or wound dehiscence. Manipulate gently, with the hand high on the tibia.
Step 3 - Arthroscopic Management
- Cyclops lesion - arthroscopic excision of the nodule (with notchplasty if there is impingement) reliably restores extension.
- Diffuse arthrofibrosis - arthroscopic lysis of adhesions and selective release, often combined with a gentle manipulation at the same sitting.
Step 4 - Open Surgery / Revision
- Open release / quadricepsplasty for severe or recurrent diffuse scar resistant to arthroscopic treatment.
- Revision arthroplasty is reserved for stiffness due to component malposition or oversizing - and according to PubMed is typically a last resort when scar alone is the problem (Ramos et al., JBJS Reviews 2023; DOI).
If stiffness is due to a malpositioned or oversized component, no amount of manipulation or release will help - the implant must be revised. Diagnose this before operating for "arthrofibrosis".
Reassurance on Arthroscopy After TKA
According to PubMed, knee arthroscopy after ipsilateral TKA (commonly for patellar clunk/synovial hyperplasia or arthrofibrosis) was not associated with an elevated risk of periprosthetic joint infection in a registry-matched study, so arthroscopic treatment of post-TKA stiffness is a reasonable option (Wahlig et al., J Arthroplasty 2024; DOI).
Quadricepsplasty (Judet and Thompson)
Management Step 4 lists "open release / quadricepsplasty" and Viva 3 asks "what is the role of quadricepsplasty?" — here is the procedure those references rely on. Quadricepsplasty is the surgical lengthening/release of a scarred, contracted extensor mechanism that mechanically blocks flexion (typically dense extra-articular quadriceps scarring after a distal femoral fracture, prolonged immobilisation, or recalcitrant arthrofibrosis that has failed arthroscopic lysis).
- Thompson quadricepsplasty (1944) — a single-stage proximal release: through a midline/lateral approach, free the intra-articular adhesions and the patella, then release the scarred vastus intermedius and rectus from the femur, dividing the patellar retinacula as needed and checking flexion intra-operatively. Simpler, but splitting the vasti risks devascularising/denervating them and leaving an extension lag.
- Judet quadricepsplasty (1959) — a more extensive, sequential release performed step-by-step and tested at each stage: (1) release intra-articular and peripatellar adhesions and mobilise the patella; (2) release the vastus lateralis and the lateral intermuscular septum; (3) free the vastus intermedius off the femur; (4) only if flexion is still inadequate, release the rectus femoris origin. Flexion is checked after each step and the release stopped once adequate flexion (around 90 to 120 degrees) is reached, which preserves extensor continuity, strength and blood supply better than a single proximal release.
Key principles: protect the extensor mechanism's continuity and vascularity, achieve the gain on the table, and begin immediate continuous passive motion and aggressive supervised rehabilitation to hold it. Complications include an extension lag (quadriceps weakness), wound/skin problems, patellar fracture and recurrence. (A frank extensor-mechanism rupture is a different problem — see the extensor-mechanism-ruptures topic.)
Q: How does the Judet quadricepsplasty differ from the Thompson, and why does it matter? A: The Thompson is a single proximal release; the Judet is a sequential distal-to-proximal release, tested at each step and halted once adequate flexion is reached. The Judet approach better preserves active extension (less extension lag) at the cost of a larger dissection. Immediate aggressive rehabilitation is essential after either.
Infrapatellar Contracture Syndrome (Paulos)
The classification and Viva 3 flag infrapatellar contracture syndrome (ICS) and patella baja as the poor-prognosis pattern — here is the entity in full. ICS is an aggressive, exaggerated fibrotic response centred on the anterior compartment (infrapatellar fat pad, peripatellar retinaculum and patellar tendon) that "captures" the patella and progressively shortens the extensor mechanism, producing patella baja (infera).
- Pathognomonic sign: markedly reduced patellar mobility in both the mediolateral and superoinferior directions (patellar entrapment / "shelf sign"), with painful restriction of flexion and extension and a developing low-riding patella.
- Paulos three stages:
- Prodromal (roughly 2 to 8 weeks): painful, decreasing motion, quadriceps shutdown and early loss of patellar mobility. This is the window to intervene with anti-inflammatory measures and gentle, controlled therapy — aggressive manipulation or surgery here inflames the process and makes it worse.
- Active (roughly 6 to 20 weeks): florid scarring, marked global restriction, skin changes and developing patella baja.
- Residual / burnt-out (after several months): inflammation settles but a fixed contracture, established patella infera and secondary patellofemoral arthrosis remain.
- Management is stage-dependent: early disease is calmed (anti-inflammatories, controlled motion, not forceful MUA); the residual stage is treated surgically with anterior-interval / medial and lateral retinacular release and fat-pad debridement, with quadricepsplasty for the contracted extensor mechanism — but outcomes are guarded once patella infera and arthrosis are established. The detailed measurement of patellar height (Insall-Salvati, Caton-Deschamps, Blackburne-Peel) is developed in the patellar-height-abnormalities topic.
Q: Why must infrapatellar contracture syndrome be recognised early rather than treated like ordinary stiffness? A: Because in the prodromal/active inflammatory stages, forceful manipulation or release makes it worse — the correct early treatment is anti-inflammatory measures and gentle controlled motion. The pathognomonic clue is global loss of patellar mobility with developing patella baja; once patella infera is fixed (residual stage) the prognosis is poor.
Complications
Scar can re-form, especially after late or repeated intervention. Aggressive post-procedure physiotherapy is essential to hold the gains made.
Forceful or late manipulation can cause periprosthetic fracture, patellar tendon avulsion, wound dehiscence and haemarthrosis.
Some patients have ongoing pain out of proportion; complex regional pain syndrome both mimics and complicates arthrofibrosis.
A stiff knee impairs stairs, transfers and gait, and patient satisfaction after revision for stiffness alone is often modest.
Guidelines, Registries & Global Practice
Global Epidemiology
- Clinically significant stiffness needing manipulation after TKA occurs in roughly 1.5-5% of knees worldwide; younger, obese and smoking patients are over-represented.
- Cyclops lesions appear in up to ~27% of second-look arthroscopies after ACL reconstruction, but symptomatic cyclops syndrome affects only ~3-11%.
- A narrow intercondylar notch and graft malposition are recognised anatomical/technical risk factors for cyclops formation.
Side-by-Side Guidance
- Stance
- Prevention and staged escalation
- Emphasis
- Early ROM, multimodal analgesia, MUA before scar matures
- Stance
- Optimise rehab pathways
- Emphasis
- Pain control and physiotherapy to prevent stiffness after TKA/ACL
- Stance
- ACL focus
- Emphasis
- Correct graft placement and debris removal to prevent cyclops; arthroscopic excision when symptomatic
- Stance
- Exclude treatable cause first
- Emphasis
- Never label stiffness arthrofibrosis until infection/malposition excluded
Registry and Outcome Data
- Arthroplasty registries (NJR, AJRR, AOANJRR) capture manipulation and reoperation for stiffness as quality indicators, consistently showing higher rates in younger TKA recipients.
- Registry and cohort data confirm stiffness is a leading non-infective reason for early reoperation after TKA.
High- vs Limited-Resource Practice
Multimodal analgesia, rotational CT, MRI for cyclops, and arthroscopic lysis/excision are routinely available, enabling early diagnosis and staged, joint-preserving treatment.
Where MRI and arthroscopy are scarce, diagnosis is clinical and treatment leans on physiotherapy and manipulation. Late presentation with mature scar worsens outcomes, underscoring the value of prevention through good early rehabilitation.
MCQ Practice Points
Q: How is arthrofibrosis diagnosed? A: Clinically and by exclusion. There is no confirmatory biopsy and no biomarker - rule out infection, malposition, instability and CRPS first.
Q: What is the best-established profibrotic pathway? A: TGF-beta signalling, driving myofibroblast activation and type I collagen deposition.
Q: When is manipulation under anaesthesia most effective after TKA? A: Early - within roughly 6 to 12 weeks, before scar matures. Late MUA is less effective and riskier.
Q: What motion does a cyclops lesion typically block? A: Terminal extension. It is a fibrous nodule anterior to the ACL graft, treated by arthroscopic excision.
Q: Which patients are at higher risk of needing MUA after TKA? A: Younger (under 60), obese and smokers. Younger age is a particularly strong independent risk factor.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman is 10 weeks after a primary TKA. She has poor range of motion (5 to 75 degrees) despite physiotherapy and is in pain. How do you assess and manage her?”
“A 24-year-old man is 4 months after hamstring ACL reconstruction. He cannot fully straighten the knee, has anterior pain and a palpable clunk near terminal extension. What is your diagnosis and management?”
“A 45-year-old man has had two prior knee operations and now has severe stiffness with patella baja on the lateral radiograph. Manipulation has already failed once. How do you proceed?”
Key Concepts
- Pathological scar restricting knee motion
- Diagnosis of exclusion - no biopsy, no biomarker
- Myofibroblast + type I collagen; TGF-beta key pathway
- Spectrum: diffuse (TKA) to localised (cyclops)
Exclude First
- Infection (CRP/ESR/aspirate)
- Component malposition or oversizing
- Instability
- CRPS and inadequate rehabilitation
Cyclops Lesion
- After ACL reconstruction
- Loss of terminal EXTENSION + clunk
- Fibrous nodule anterior to graft on MRI
- Arthroscopic excision (+ notchplasty)
Management Ladder
- Prevention: analgesia + early ROM
- MUA: best within 6-12 weeks
- Arthroscopic lysis of adhesions
- Open release / revision (last resort)
Risk Factors
- Younger age (under 60) - strong
- Obesity, smoking
- Multiple prior surgeries
- Narrow notch (cyclops)
Evidence and Key Studies
Arthrofibrosis After TKA: Critical Analysis Review
- Arthrofibrosis is a clinical diagnosis of exclusion
- No biopsy and no biomarker confirms it
- Myofibroblasts deposit type I collagen; TGF-beta is the key pathway
- Revision arthroplasty is reserved as a last resort
Multimodal Pain Management and Arthrofibrosis
- Manipulation rate fell from 4.75% to 2.24% with multimodal analgesia
- Better early pain control allows earlier mobilisation
- Supports prevention over later intervention
- Recommends multimodal protocols for TKA
Risk Factors for Manipulation After TKA
- Overall MUA rate after TKA was 1.51%
- Younger age (under 60) is a strong risk factor (RR 3.46)
- Obesity and nicotine dependence increase risk
- Diabetes and depression were not significant risk factors
Multifactorial Etiopathogenesis of the Cyclops Lesion
- Cyclops is a fibroproliferative nodule, multifactorial in origin
- Drilling debris and stump remnants are key sources
- Graft malposition causing notch impingement contributes
- Arthroscopic resection (plus notchplasty) restores extension
Cyclops Syndrome After Double-Bundle ACL Reconstruction
- Symptomatic cyclops syndrome occurred in 3.61%
- More common with quadriceps than hamstring graft
- Mean extension loss ~6 degrees with early quad dysfunction
- Arthroscopic debridement restored motion in most
Intercondylar Notch Size and Cyclops Formation
- Cyclops lesions in 27.3% but symptomatic in only 10.9%
- Smaller intercondylar notch predisposes to cyclops formation
- Higher tunnel-to-notch ratio in the cyclops group
- Most cyclops lesions are asymptomatic incidental findings