Orthopedic Emergency | Multiligamentous Injury | Vascular Catastrophe
ANATOMIC CLASSIFICATION
Critical Must-Knows
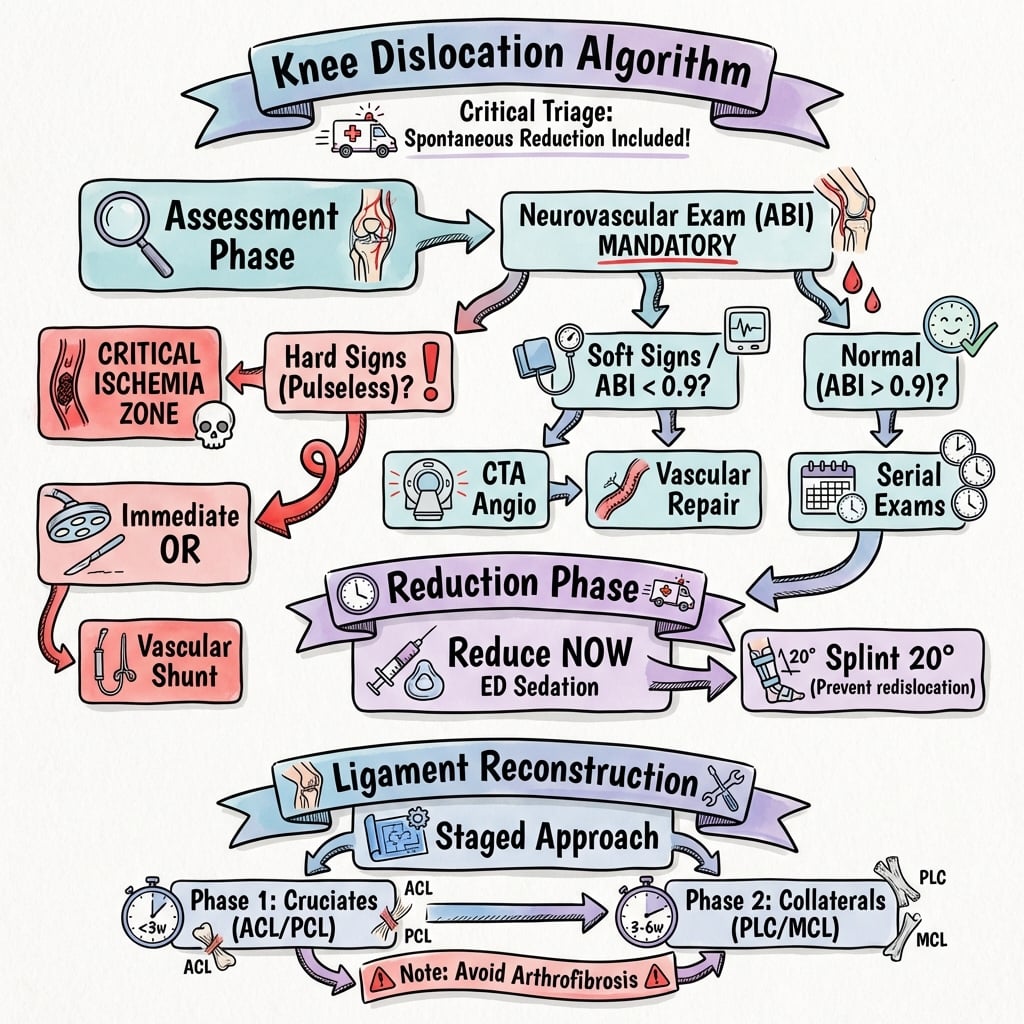
- VASCULAR EMERGENCY - Rule out popliteal artery injury in ALL cases with ABI and CTA
- Immediate reduction reduces vascular compromise - perform in ED under sedation
- Serial neurovascular exams - Document before and after reduction, every 2 hours
- Multiligamentous repair - Staged approach: ACL/PCL first, then collaterals at 3-6 weeks
- 20% missed initially - High suspicion if spontaneous reduction before arrival
Clinical Pearls
- "Popliteal artery injury occurs in 30-40% - Normal pulses do NOT exclude intimal tear
- "ABI less than 0.9 = Mandatory CTA - Sensitivity 95% for arterial injury
- "Peroneal nerve injury (25%) - Check foot dorsiflexion and eversion before/after reduction
- "Schenck Classification (KD I-V) grades injury severity based on ligaments torn
Clinical Imaging
Imaging Gallery




Critical Knee Dislocation Exam Points
Vascular Assessment Protocol
MANDATORY workup. Normal pulses do NOT exclude arterial injury. Intimal tears can present with normal distal pulses initially then thrombose at 6-24 hours. ABI less than 0.9 requires immediate CTA. Vascular surgery consult if any abnormality.
Reduction Technique
Reduce immediately. Do NOT delay for imaging if neurovascular compromise present. Longitudinal traction with counter-traction. Reverse mechanism of injury. Reassess pulses post-reduction. Splint in 15-20 degrees flexion to prevent re-dislocation.
Schenck Classification
KD I-V system. KD I (one cruciate), KD II (both cruciates), KD III (M or L) (cruciate + collateral), KD IV (M or L) (both cruciates + collateral), KD V (fracture-dislocation). Higher grades = worse outcomes.
Surgical Timing
Staged repair approach. Acute: Reduce and splint, repair vascular/nerve injuries. Early (less than 3 weeks): ACL/PCL reconstruction. Delayed (3-6 weeks): Collateral ligament repair. Prevents arthrofibrosis with early total repair.
Quick Decision Guide
| Scenario | Vascular Status | Management | Key Pearl |
|---|---|---|---|
| Reduced dislocation, normal ABI (greater than 0.9) | Normal pulses, ABI 1.0 | Serial neurovascular exams, CTA if change | Intimal tears can thrombose at 6-24h |
| Reduced dislocation, ABI 0.7-0.9 | Diminished pulses | URGENT CTA + vascular surgery consult | 20% progress to thrombosis |
| Irreducible or pulseless limb | Absent pulses, cold foot | IMMEDIATE reduction + vascular surgery OR | 6-hour ischemia window - Amputation risk 86% |
PANICStructures at Risk in Knee Dislocation
| P | Popliteal artery 30-40% injury rate, intimal tears common |
| A | ACL and PCL Both cruciates torn in 80% of dislocations |
| N | Nerve (peroneal) 25-30% injury, check foot dorsiflexion |
| I | Intima (vessel) Can thrombose 6-24h post-injury despite normal pulses |
| C | Collaterals (MCL/LCL) Often torn with PLC - complete multiligament injury |
| P | Popliteal artery 30-40% injury rate, intimal tears common | I | Intima (vessel) Can thrombose 6-24h post-injury despite normal pulses |
| A | ACL and PCL Both cruciates torn in 80% of dislocations | C | Collaterals (MCL/LCL) Often torn with PLC - complete multiligament injury |
| N | Nerve (peroneal) 25-30% injury, check foot dorsiflexion |
Hook:Knee dislocation causes PANIC - Check Popliteal artery, ACL/PCL, Nerve, Intima, Collaterals!
CLIMBSchenck Classification (KD I-V)
| C | Cruciate alone KD I - Single cruciate injury (rare) |
| L | Ligaments both cruciates KD II - ACL + PCL torn |
| I | Including one collateral KD III - Cruciates + MCL or LCL |
| M | Medial AND lateral KD IV - Both cruciates + both collaterals |
| B | Bone fracture KD V - Fracture-dislocation (periarticular) |
| C | Cruciate alone KD I - Single cruciate injury (rare) | M | Medial AND lateral KD IV - Both cruciates + both collaterals |
| L | Ligaments both cruciates KD II - ACL + PCL torn | B | Bone fracture KD V - Fracture-dislocation (periarticular) |
| I | Including one collateral KD III - Cruciates + MCL or LCL |
Hook:CLIMB the knee dislocation severity ladder from KD I to KD V!
REDUCEAcute Management Priorities
| R | Recognize vascular injury Check ABI, pulses before and after reduction |
| E | Emergency reduction Immediate reduction if neurovascular compromise |
| D | Document neurovascular status Serial exams every 2 hours for 24 hours |
| U | Urgent CTA if abnormal ABI less than 0.9 = CTA + vascular surgery |
| C | Collateral assessment MRI to plan staged reconstruction |
| E | Early cruciate repair ACL/PCL within 3 weeks, collaterals 3-6 weeks |
| R | Recognize vascular injury Check ABI, pulses before and after reduction | D | Document neurovascular status Serial exams every 2 hours for 24 hours | C | Collateral assessment MRI to plan staged reconstruction |
| E | Emergency reduction Immediate reduction if neurovascular compromise | U | Urgent CTA if abnormal ABI less than 0.9 = CTA + vascular surgery | E | Early cruciate repair ACL/PCL within 3 weeks, collaterals 3-6 weeks |
Hook:REDUCE is the goal - systematic approach prevents complications!
Overview and Epidemiology
Why This Topic Matters
Knee dislocation is an orthopedic emergency with potential for limb-threatening vascular injury. Despite being rare (0.02% of knee injuries), the consequences of missed diagnosis are catastrophic: amputation rates of 86% if ischemia exceeds 6 hours. The key challenge is that 20% of dislocations spontaneously reduce before arrival, making diagnosis difficult unless high clinical suspicion is maintained.
Mechanism of Injury
- High-energy trauma (60%): Motor vehicle collision, fall from height
- Low-energy in obese (40%): Simple fall, hyperextension
- Sports injuries: Dashboard injury, contact sports (football, rugby)
- Ultra-low velocity: Morbidly obese patients (BMI greater than 40)
Associated Injuries
- Popliteal artery injury: 30-40% (intimal tear most common)
- Peroneal nerve palsy: 25-30% (lateral dislocations highest risk)
- Compartment syndrome: 10-15% (especially after vascular repair)
- Meniscal tears: 50% (often peripheral detachment)
Anatomy
Ligamentous Anatomy
- ACL: Anteromedial and posterolateral bundles
- PCL: Anterolateral and posteromedial bundles
- MCL: Superficial (tibial attachment) and deep (meniscal)
- LCL: Fibular attachment, part of posterolateral corner
Posterolateral Corner (PLC)
- LCL: Primary lateral stabilizer
- Popliteus tendon: Dynamic posterolateral stabilizer
- Popliteofibular ligament: Resists external rotation
- Lateral capsule: Secondary restraint

Pathophysiology
Popliteal Artery Vulnerability
The popliteal artery is tethered proximally at the adductor hiatus and distally at the soleus arch, making it vulnerable to injury during knee dislocation. Intimal tears can occur WITHOUT complete disruption, presenting initially with normal pulses but thrombosing 6-24 hours later. This is why normal pulses do NOT exclude arterial injury.
Anatomic Constraints and Injury Patterns
| Structure | Anatomic Feature | Injury Mechanism | Clinical Significance |
|---|---|---|---|
| Popliteal artery | Tethered at adductor hiatus and soleus arch | Stretching during anterior dislocation | Intimal tear common, delayed thrombosis |
| Common peroneal nerve | Wraps around fibular neck | Traction injury in lateral/posterolateral dislocation | 25-30% injury rate, poor recovery |
| ACL and PCL | Intracapsular, minimal blood supply | Torn in 80% of dislocations | Both require reconstruction for stability |
Injury Mechanism and Cascade
Pathological sequence in knee dislocation:
- High-energy force - MVA, sports collision, fall from height
- Ligamentous failure - ACL/PCL rupture, capsular disruption
- Joint subluxation/dislocation - Tibiofemoral joint displaced
- Vascular tethering - Popliteal artery stretched over fixed points
- Intimal injury - Dissection, thrombosis, or complete transection
- Nerve traction - Peroneal nerve stretched around fibular head
- Spontaneous reduction - May occur, masking severity of injury
Classification Systems
Schenck Classification (Most Widely Used)
| Grade | Ligaments Injured | Frequency | Prognosis |
|---|---|---|---|
| KD I | Single cruciate (ACL or PCL) | 5-10% | Good with reconstruction |
| KD II | Both cruciates (ACL + PCL) | 15-20% | Moderate, requires both repairs |
| KD III-M | Cruciates + MCL | 25% | Fair, staged repair needed |
| KD III-L | Cruciates + LCL/PLC | 30% | Fair, PLC critical for rotatory stability |
| KD IV-M/L | All four major ligaments | 20% | Poor, high stiffness risk |
| KD V | Periarticular fracture + ligament | 10% | Variable, fracture healing affects timing |
Schenck Mnemonic
Think I - II - III - IV - V as increasing severity: I = one cruciate, II = two cruciates, III = three ligaments (add one collateral), IV = four ligaments (all), V = five problems (ligaments plus fracture).

Clinical Assessment
History
- Mechanism: High-energy trauma, dashboard injury, hyperextension
- Reduced in field: 20% spontaneously reduce - Ask if knee "popped out"
- Pain and swelling: Immediate hemarthrosis, inability to bear weight
- Paresthesias: Foot numbness suggests nerve or vascular injury
Examination
- Look: Gross deformity (if not reduced), swelling, ecchymosis
- Neurovascular: MANDATORY before and after reduction - ABI, pulses, peroneal nerve
- Stability testing: DO NOT stress test acutely - Risk re-dislocation
- Compartments: Palpate for tightness, especially post-vascular repair
The Spontaneously Reduced Dislocation
20% of knee dislocations reduce spontaneously before medical evaluation. High clinical suspicion is required if history suggests transient dislocation. Key clues: High-energy mechanism, severe instability on exam, inability to bear weight despite normal X-rays. Obtain MRI to assess multiligamentous injury.
Differential Diagnosis
The spontaneously reduced dislocation and the acutely swollen, unstable knee can be confused with lesser injuries. The distinction matters because only the true (occult) dislocation mandates the full vascular pathway.
Differential Diagnosis of the Acutely Unstable Knee
| Diagnosis | Discriminating Features | Vascular/Nerve Risk | Key Investigation |
|---|---|---|---|
| Knee dislocation (incl. spontaneously reduced) | Multidirectional gross instability, 2 or more ligaments torn, high-energy or ultra-low-velocity in obese | High - popliteal artery and peroneal nerve at risk | ABI plus serial exam; MRI for ligament pattern |
| Isolated ACL rupture | Single-plane anterior laxity, positive Lachman, intact PCL and collaterals | Negligible | MRI; vascular workup not required |
| Patellar dislocation | Patella displaced (usually lateral), tibiofemoral joint congruent, apprehension sign | Negligible | Skyline/axial radiograph; MRI for MPFL |
| Tibial plateau fracture-dislocation (Schenck KD-V) | Bony deformity plus instability, articular step-off on imaging | High - treat as a dislocation | CT for fracture; ABI plus CTA |
| Proximal tibiofibular joint dislocation | Lateral fibular head prominence, peroneal symptoms, tibiofemoral joint reduced | Peroneal nerve at risk; artery usually spared | AP/oblique radiograph, comparison views |
Vascular Assessment Protocol (MANDATORY)
| Test | Normal Value | Abnormal Finding | Action Required |
|---|---|---|---|
| Ankle-Brachial Index (ABI) | Greater than 0.9 | Less than 0.9 | IMMEDIATE CTA + vascular surgery consult |
| Pedal pulses | 2+ bilateral | Diminished or absent | Urgent CTA (do NOT rely on pulses alone) |
| Capillary refill | Less than 2 seconds | Greater than 3 seconds | Immediate reduction, reassess post-reduction |
| Serial exams | Stable over 24 hours | Deterioration at any point | Urgent CTA - Delayed thrombosis |

Investigations
Imaging Protocol
Before reduction: Document dislocation direction, identify fractures (KD V). After reduction: Confirm concentric reduction, assess for occult fractures (tibial plateau, femoral condyle). Stress views should NOT be performed acutely.
MANDATORY in all cases. ABI less than 0.9 has 95% sensitivity for arterial injury. Perform before and after reduction, then serially every 2 hours for 24 hours. Normal ABI does NOT exclude intimal tear.
Gold standard for arterial injury. Sensitivity 95%, specificity 99% for popliteal artery injury. Detects intimal tears, pseudoaneurysms, complete disruption. URGENT vascular surgery consult if any abnormality.
Once vascular status secure. Typically performed at 5-7 days post-injury to assess ligament injury pattern and plan staged reconstruction. T2-weighted sequences show all ligament tears, meniscal injuries, and chondral damage.
Do NOT Delay Reduction for Imaging
If obvious dislocation with neurovascular compromise, reduce IMMEDIATELY in the emergency department under procedural sedation. Do NOT wait for X-rays or CT. Reduction improves vascular flow and reduces compartment pressure. Image AFTER reduction to confirm concentric alignment.
Management Algorithm
Acute Management (First 6 Hours)
Goal: Restore vascular flow, prevent limb loss, document injuries.
ED Protocol
- Identify knee dislocation (obvious or history of reduction)
- Document neurovascular status (ABI, pulses, peroneal nerve)
- Obtain AP/lateral X-rays if time permits
- Procedural sedation (propofol or ketamine)
- Longitudinal traction with counter-traction at thigh
- Reverse mechanism of injury (flex for anterior, extend for posterior)
- Reassess neurovascular status post-reduction
- Repeat ABI and pulses (document improvement or deterioration)
- Confirm concentric reduction on X-ray
- Splint knee in 15-20 degrees flexion (prevents re-dislocation)
- Vascular surgery consult if ABI less than 0.9
- Neurovascular checks every 2 hours for 24 hours
- Watch for compartment syndrome (especially post-vascular repair)
- MRI at 5-7 days to plan ligament reconstruction
Reduction Technique Pearl
For anterior dislocation (most common): Apply longitudinal traction to tibia while assistant provides counter-traction at thigh. Gently extend knee while applying posterior pressure to proximal tibia. For posterior dislocation: Flex hip to 90 degrees, apply traction, then extend knee while lifting tibia anteriorly.
Surgical Technique
Cruciate Ligament Reconstruction
Surgical Steps (ACL + PCL)
Supine on standard operating table. Lateral post at thigh. Foot of bed dropped for knee flexion. Tourniquet thigh (usually NOT inflated due to vascular concerns). Prepare for arthroscopy and open if needed.
Standard portals (anterolateral, anteromedial). Assess cruciate tears, meniscal injuries, chondral damage. Document with photos. Perform limited debridement of cruciate remnants (preserve tibial footprint).
Bone-patellar tendon-bone (BTB) autograft preferred for ACL (bone blocks aid fixation). Achilles allograft often used for PCL (larger diameter, less donor morbidity). Prepare grafts on back table with whipstitch sutures.
ACL: Femoral tunnel at 10:30 (right knee) or 1:30 (left knee), tibial tunnel at ACL footprint. PCL: Femoral tunnel at 2:00 (right) or 10:00 (left), tibial tunnel via posteromedial portal. Ensure tunnels avoid convergence.
ACL first: Pass graft, fix femur (interference screw or button), tension at 20 degrees flexion, fix tibia. PCL second: Pass via posteromedial portal, fix femur, tension at 90 degrees flexion (posterior drawer reduced), fix tibia.
Check stability: Lachman (ACL), posterior drawer (PCL). Assess ROM (should achieve 0-130 degrees). Document with fluoroscopy. Ensure no graft impingement. Close portals, apply hinged knee brace locked 0-90 degrees.
Avoid Convergence of Tunnels
When reconstructing both ACL and PCL, femoral tunnels can converge (ACL at 10:30/1:30, PCL at 2:00/10:00). Use 3D planning on CT or intraoperative fluoroscopy to ensure adequate bone bridge. If concern, stage PCL reconstruction 6 weeks later.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Limb loss (amputation) | 5-10% overall, 86% if ischemia greater than 6h | Delayed vascular repair, compartment syndrome | Prevention: Immediate reduction and vascular surgery consult |
| Arthrofibrosis (stiffness) | 20-50% (50% if early total repair) | Early total ligament repair, inadequate ROM | Prevention: Staged repair. Treatment: Manipulation or arthroscopic lysis |
| Persistent instability | 15-30% | Missed PLC injury, graft failure | Revision reconstruction with attention to PLC |
| Permanent peroneal nerve palsy | 10-20% (25-30% have initial injury) | Traction injury, compartment syndrome | Ankle-foot orthosis, tendon transfer if no recovery at 12 months |
| Deep vein thrombosis | 10-15% | Vascular repair, immobilization | Prophylactic anticoagulation, early mobilization |
Compartment Syndrome Post-Vascular Repair
Compartment syndrome occurs in 10-15% of patients after popliteal artery repair due to reperfusion injury. Maintain HIGH clinical suspicion. Perform 4-compartment fasciotomy liberally if any concern (pain out of proportion, tense compartments). Delayed fasciotomy (greater than 6-8 hours) leads to permanent muscle and nerve damage.
Postoperative Care and Rehabilitation
ACL/PCL Reconstruction Protocol
- Hinged knee brace locked 0-90 degrees
- Weight-bearing as tolerated with crutches
- ROM exercises: Passive extension to 0 degrees, flexion to 90 degrees
- Quad sets, ankle pumps, SLR (avoid hamstring contraction)
- Unlock brace, progress ROM to 0-120 degrees
- Weight-bearing as tolerated, wean crutches by week 4
- Closed-chain exercises (wall sits, mini squats)
- Avoid open-chain hamstring exercises (protect PCL)
- Full ROM expected (0-130 degrees)
- Progress strengthening (leg press, step-ups)
- Proprioception and balance training
- Stationary bike, swimming (no breaststroke)
- Jogging at 4-6 months if quad strength greater than 70%
- Sport-specific training at 6-9 months
- Return to sport at 12 months (MINIMUM)
- Functional testing before clearance
Outcomes and Prognosis
| Treatment Approach | Stability Outcome | ROM Outcome | Notes |
|---|---|---|---|
| Staged reconstruction (cruciates early, collaterals delayed) | Good stability 70-80% | Stiffness 20%, full ROM 60% | Current gold standard approach |
| Early total repair (all ligaments at once) | Good stability 60-70% | Stiffness 50%, full ROM 30% | Historical approach, high stiffness rate |
| Delayed reconstruction (greater than 3 months) | Variable stability 50-70% | Better ROM (low stiffness) | Scar tissue makes reconstruction difficult |
Predictors of Poor Outcome
Poor outcomes are associated with: (1) Vascular injury requiring repair (higher complication rate), (2) KD IV or KD V injuries (all ligaments torn), (3) Peroneal nerve palsy (10-20% permanent), (4) Delayed reconstruction (greater than 6 months), and (5) High-energy mechanism (polytrauma, associated injuries).
Evidence Base and Key Trials
How to Read This Evidence
There is NO randomised controlled trial in knee dislocation - the injury is too rare and heterogeneous. The literature is dominated by systematic reviews, meta-analyses, and single-surgeon case series (Level III-IV). Every quoted figure below has been verified against the primary source; be cautious of the often-repeated "30-40% vascular injury" and "86% amputation" figures, which come from older selected series - pooled modern data give lower, more accurate numbers.
Decision Making in the Multiligament-Injured Knee: Evidence-Based Systematic Review
- Systematic review (Levels I-IV) of operative vs nonoperative, repair vs reconstruction, and early vs late surgery
- Surgery outperformed nonoperative care: good/excellent IKDC 58% vs 20%, return to full sport 29% vs 10%
- Posterolateral corner REPAIR failed more often than reconstruction (37% vs 9%)
- Early surgery (within 3 weeks) gave higher Lysholm (90 vs 82) and IKDC scores than delayed surgery
Vascular Injuries in Knee Dislocations: Role of Physical Examination in Determining Need for Arteriography
- Prospective cohort: 126 patients (134 knees) with acute multiligament knee injury at a Level-1 trauma centre
- Flow-limiting popliteal artery injury in 9 patients (7% prevalence) - lower than older quoted figures
- Serial physical examination had a single false positive and no missed injury (selective, not routine, arteriography)
- All 9 vascular injuries occurred in KD-III, KD-IV or KD-V; KD-IV warrants serial exams for at least 48 hours
The Role of Arteriography in Assessing Popliteal Artery Injury in Knee Dislocations
- Retrospective review of 55 patients (57 knees) with traumatic knee dislocation over 7 years
- Vascular exam (foot pulses plus ABI of 0.80 or greater) normal in 32 knees, abnormal in 25
- NO knee with a normal vascular examination had an injury requiring treatment
- Of 25 abnormal exams, 12 had vascular injury on angiography and 7 needed reverse saphenous vein grafting
Vascular and Nerve Injury After Knee Dislocation: A Systematic Review
- Meta-analysis of 862 knee dislocations - the largest pooled vascular/nerve dataset
- Weighted vascular injury frequency 18% and nerve injury 25% (lower than classic 30-40% teaching)
- 80% of vascular injuries were repaired; 12% of vascular injuries ended in amputation
- Highest vascular prevalence in KD-IIIL (ACL/PCL/lateral, 32%) and in posterior dislocations (25%)
Incidence of Concurrent Peroneal Nerve Injury in Multiligament Knee Injuries and Outcomes
- Retrospective cohort of 357 surgically treated multiligament knee injuries (mean follow-up 35 months)
- Concurrent peroneal nerve injury in 68 patients (19%)
- Nerve-injured patients had significantly lower final ROM (121 vs 127 degrees) and trended to lower return to work
- Pain (VAS), Lysholm and IKDC scores did NOT differ significantly with or without nerve injury
Arthroscopically Assisted Combined ACL/PCL Reconstruction in the Multiple Ligament Injured Knee: 2- to 10-Year Follow-up
- Case series of 35 combined ACL/PCL reconstructions (19 acute, 16 chronic) followed 2-10 years
- Significant improvement in Lysholm (mean 91), Tegner and HSS scores and in KT-1000 side-to-side laxity
- Normal Lachman/pivot-shift in 33 of 35 (94%); restored posterolateral stability less reliable
- Conclusion: reconstructed knees are functionally stable but NOT normal
Outcomes After Multiligament Knee Injury Worsen Over Time: Systematic Review and Meta-Analysis
- Meta-analysis of 79 studies and 3571 surgically treated multiligament knee injuries (mean age 35.6 years)
- Mean Lysholm 86 and IKDC 81 at 2 years, retaining roughly 80-85% of knee function
- Knee function DETERIORATES yearly (IKDC about -2.0 points/year), not a stable plateau
- PCL-based injuries had significantly worse IKDC (75 vs 84) and Lysholm (84 vs 91) than non-PCL injuries
Knee Dislocations in the Morbidly Obese Patient (Ultra-Low-Velocity Dislocation)
- Review of the increasingly common ultra-low-velocity knee dislocation in obese, morbidly obese and super-obese patients
- These injuries occur during everyday activities yet can be as severe or worse than high-velocity dislocations
- Frequently associated with neurovascular injury - early reduction and vascular assessment are critical to avoid amputation
- Limb size usually mandates external fixation to maintain reduction; reconstruction still improves outcomes
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Knee Dislocation in ED
"A 35-year-old male presents to ED after motor vehicle collision. Paramedics report his knee was dislocated and they reduced it in the field. On arrival, knee is swollen but reduced. Pedal pulses are present but diminished. What is your assessment and management?"
Scenario 2: Surgical Planning for Multiligamentous Injury
"The patient from Scenario 1 has secure vascular status (ABI 1.0). MRI at 7 days shows complete ACL, PCL, MCL, and posterolateral corner (PLC) tears (Schenck KD IV-M/L). Walk me through your surgical plan."
Scenario 3: Delayed Vascular Thrombosis
"The patient from Scenario 1 was admitted for observation. Initial ABI was 1.0. At 18 hours post-injury, nurse reports foot is cooler and pedal pulses are diminished. What is your management?"
MCQ Practice Points
Vascular Injury Question
Q: What percentage of knee dislocations have associated popliteal artery injury? A: 30-40% - This high rate is why ABI measurement is MANDATORY in all knee dislocations. Normal pulses do NOT exclude intimal tear, which can thrombose 6-24 hours later.
Classification Question
Q: A knee dislocation with complete ACL, PCL, MCL, and PLC tears is classified as: A: Schenck KD IV - All four major ligament complexes torn. KD I (one cruciate), KD II (both cruciates), KD III (cruciate + one collateral), KD IV (all ligaments), KD V (fracture-dislocation).
Treatment Question
Q: What is the advantage of staged ligament reconstruction over early total repair? A: Reduced arthrofibrosis rate (20% vs 50%) - Staged approach reconstructs cruciates early (2-3 weeks) then collaterals delayed (3-6 weeks). Early total repair has 50% stiffness rate with similar stability outcomes.
Complication Question
Q: What is the amputation rate if warm ischemia time exceeds 6 hours in knee dislocation with popliteal artery injury? A: 86% - This is why immediate reduction and vascular repair are critical. Time is limb in this injury.
Nerve Injury Question
Q: Common peroneal nerve injury occurs in what percentage of knee dislocations, and which dislocation direction has the highest risk? A: 25-30% overall, highest in lateral and posterolateral dislocations - Nerve wraps around fibular neck and is stretched during lateral displacement. Complete palsy has only 10-20% recovery rate.
Controversies and Areas of Uncertainty
True Rate of Vascular Injury
Classic teaching quotes 30-40% popliteal artery injury and 86% amputation if ischaemia exceeds 6 hours - figures from older, selected single-centre series. The largest pooled meta-analysis (Medina 2014, 862 patients) found 18% vascular injury and 12% amputation among those injured. Know both: examiners often expect the classic numbers, but the modern, more accurate figures are lower.
Routine vs Selective Angiography
Historic practice was routine arteriography in every dislocation. Prospective work (Stannard 2004; Klineberg 2004) showed a normal vascular exam plus ABI reliably excludes a limb-threatening injury, supporting a SELECTIVE pathway. CT angiography has now largely replaced catheter arteriography where available.
Repair vs Reconstruction of PLC
Acute primary repair of the posterolateral corner is attractive (single early operation) but fails far more often than reconstruction (37% vs 9% in Levy 2009). Most contemporary surgeons reconstruct, or augment repair, rather than repair alone - especially for the lateral side.
Timing and Single vs Staged Surgery
Early surgery (within 3 weeks) gives better functional scores than delayed surgery, but single-stage all-ligament reconstruction must be balanced against arthrofibrosis risk. There is no randomised evidence; decisions remain individualised by soft-tissue condition, vascular status and surgeon experience.
Peroneal Nerve - Explore or Observe?
Whether to explore, neurolyse, graft or simply observe a complete peroneal palsy remains unresolved. There is no high-level evidence that acute exploration improves recovery, and many palsies are managed expectantly with an ankle-foot orthosis, reserving tendon transfer (posterior tibial tendon) for those without recovery by 12 months. Counsel that complete palsies recover poorly.
Guidelines, Registries & Global Practice
Global Epidemiology
Knee dislocation accounts for under 0.02% of orthopaedic injuries, but true incidence is under-reported because up to 50% reduce spontaneously before assessment. The epidemiological pattern is shifting worldwide from young high-energy trauma (road traffic, falls from height) toward ultra-low-velocity dislocations in obese and morbidly obese patients during everyday activity - a trend tracking rising global obesity. There is no dedicated international knee-dislocation registry; evidence comes from trauma-centre series and systematic reviews.
Side-by-Side Guidance and Consensus (Global)
| Body / Source | Vascular Assessment | Surgical Stance | Distinctive Point |
|---|---|---|---|
| AAOS / US trauma practice | Selective angiography driven by ABI and serial exam; ABI under 0.9 triggers CTA | Operative reconstruction favoured; reconstruct PLC | Drove the move away from routine arteriography |
| BOA / BOAST (UK) major trauma standards | Immediate neurovascular assessment, documented serial exams, urgent vascular input | Manage in or refer to a unit with combined vascular and ligament expertise | Embeds dislocation in major-trauma network pathways |
| AO Foundation / fracture-dislocation (KD-V) | Reduce and stabilise first; spanning external fixator if unstable or vascular repair done | Restore bony anatomy, then staged ligament surgery | External fixation for the unstable or large (obese) limb |
| EFORT / European consensus reviews | Selective imaging plus 24-48h observation, longer vigilance for KD-IV | Early reconstruction within 3 weeks where soft tissues allow | Emphasises staged approach to limit arthrofibrosis |
High-Resource Settings
- CT angiography and MRI readily available; selective (exam/ABI-driven) vascular pathway is standard
- On-site vascular surgery enables revascularisation within the ischaemia window
- Staged arthroscopic reconstruction with allograft/autograft and hinged bracing
- 24-48h inpatient neurovascular observation routine
Limited-Resource Settings
- Reliance on clinical exam and ABI where CTA is unavailable; low threshold to transfer
- Prompt closed reduction and a spanning external fixator stabilises the limb for transfer
- Delays to vascular care raise amputation risk - early recognition is the key modifiable factor
- Definitive ligament reconstruction may be deferred or unavailable; functional bracing used
The One Thing That Must Never Be Missed
Across every guideline and resource setting, the non-negotiable standard is a documented neurovascular assessment (pulses, ABI, peroneal nerve) before and after reduction with serial re-examination. A knee dislocation discharged on "normal pulses" alone, without ABI or an observation period, can return with a cold, pulseless limb and delayed thrombosis - the single most catastrophic and avoidable outcome of this injury.
KNEE DISLOCATION
Clinical summary
Key Anatomy
- •Popliteal artery = Tethered at adductor hiatus and soleus arch (vulnerable to injury)
- •Common peroneal nerve = Wraps around fibular neck (25-30% injury rate)
- •ACL + PCL = Both torn in 80% of dislocations
- •PLC (LCL, popliteus, popliteofibular) = Critical for rotatory stability
Classification
- •Schenck KD I = Single cruciate (rare)
- •Schenck KD II = Both cruciates
- •Schenck KD III-M/L = Cruciates + one collateral
- •Schenck KD IV-M/L = All four ligaments
- •Schenck KD V = Fracture-dislocation
Treatment Algorithm
- •ED: Immediate reduction, ABI measurement, CTA if ABI less than 0.9
- •Vascular injury: URGENT repair within 6 hours (amputation rate 86% if delayed)
- •Staged repair: Cruciates at 2-3 weeks, collaterals at 3-6 weeks
- •Serial exams: Every 2 hours for 24 hours (detect delayed thrombosis)
Surgical Pearls
- •Staged approach reduces stiffness from 50% to 20%
- •ACL/PCL tunnels: Avoid convergence (use fluoroscopy)
- •PLC reconstruction: Protect common peroneal nerve throughout
- •Collateral healing: Lock brace in extension 6 weeks
Complications
- •Amputation: 5-10% overall, 86% if ischemia greater than 6h
- •Arthrofibrosis: 50% if early total repair, 20% if staged
- •Peroneal palsy: 25-30% initial injury, 10-20% permanent
- •Persistent instability: 20-30% (often missed PLC)