Know the question | know the population | know the limit
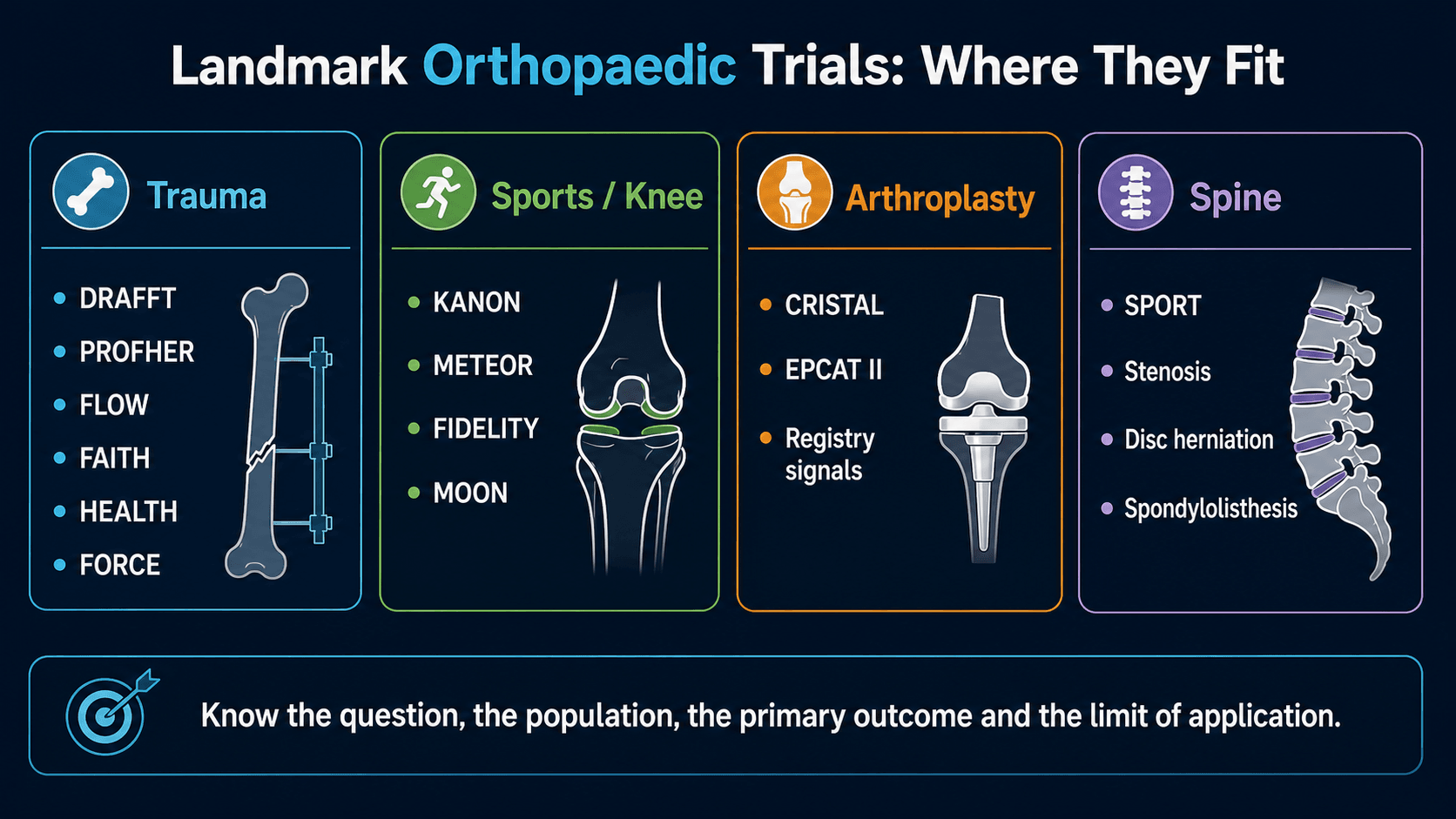
Landmark Trial Families
Critical Must-Knows
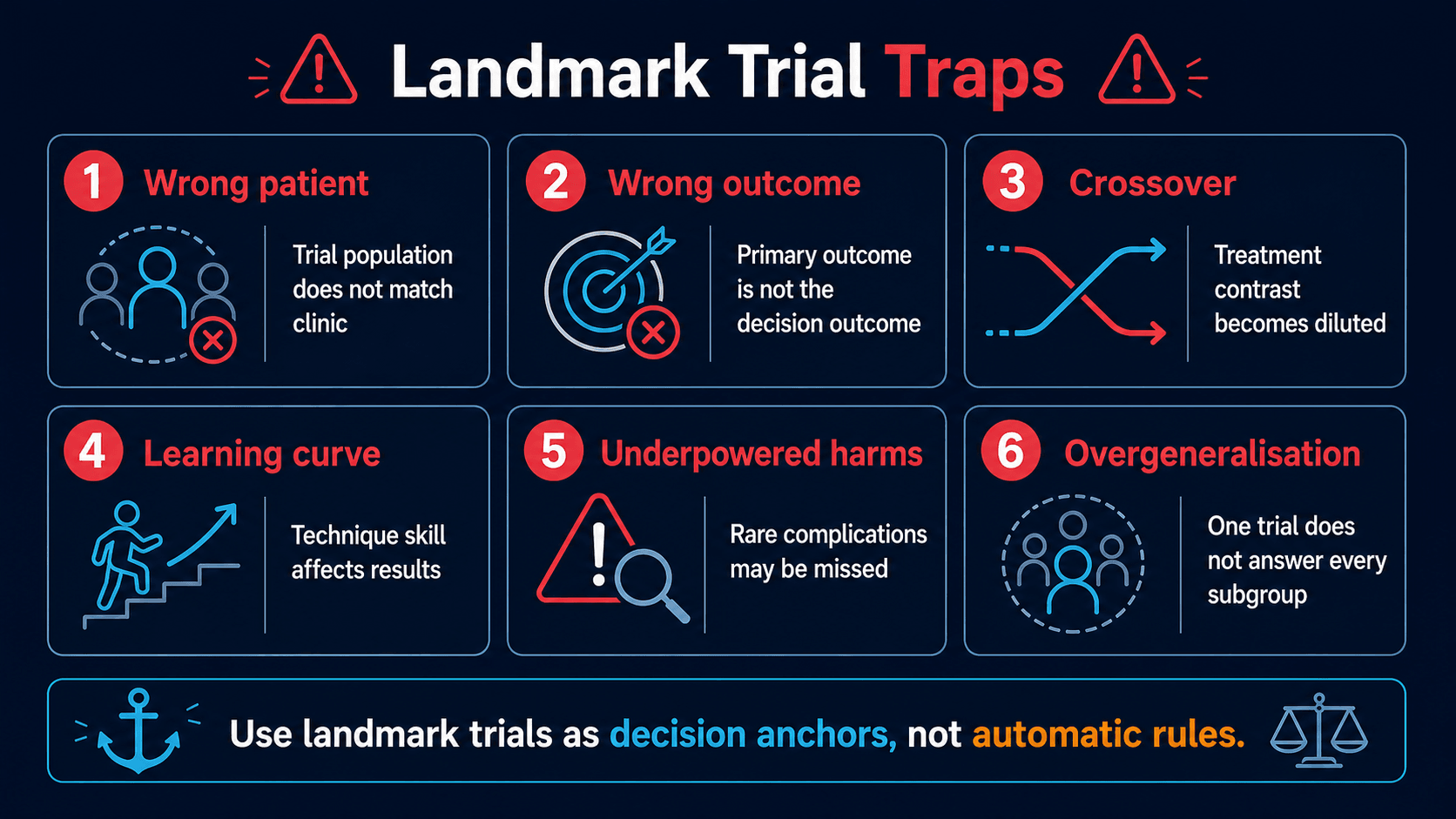
- A landmark trial is not an automatic rule. It is a strong decision anchor only when the patient, intervention, comparator and outcome match the case.
- Surgical trials often have crossover and incomplete blinding. Interpret intention-to-treat and as-treated results carefully.
- The primary outcome matters. A trial powered for function may not answer rare complications, implant survival or subgroup effects.
- Negative does not mean useless. Many trials show that routine surgery adds little for broad low-risk groups but may still help selected patients.
- Trial literacy changes management discussions. It improves consent, shared decision-making and avoidance of low-value surgery.
Clinical Pearls
- "Open every trial discussion with the PICO and the primary outcome.
- "State what the trial changed and what it did not answer.
- "Be careful applying pragmatic trial results to excluded high-risk subgroups.
- "In fracture trials, distinguish radiographic success from patient-centred function and reoperation.
- "In arthroplasty prophylaxis trials, separate symptomatic VTE, bleeding, mortality and protocol context.
Do not quote a trial without stating the patient group
“PROFHER showed no difference” or “DRAFFT changed distal radius fixation” is incomplete. A useful answer states the population, comparator, outcome and limitation. The wrong extrapolation is often more dangerous than not knowing the acronym.
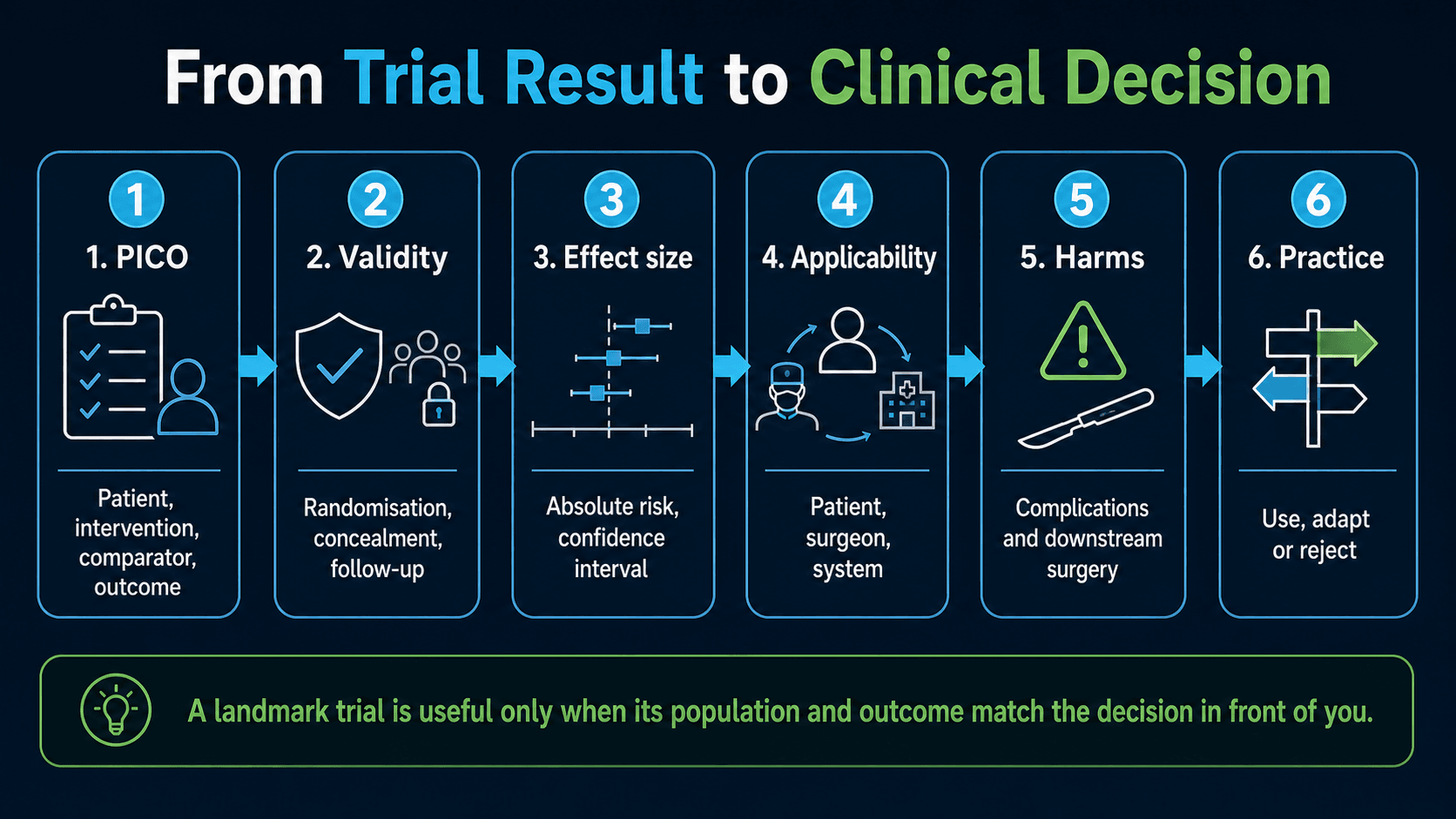
How to Use a Trial
PICOQuestion | SAFEValidity | CASTClinical use |
|---|---|---|
P Patient Age, injury, severity, setting and exclusions. | S Selection Who was included and excluded? | C Context Does the trial setting match yours? |
I Intervention Operation, implant, pathway or medication. | A Allocation Was randomisation protected? | A Absolute effect What is the real size of benefit or harm? |
C Comparator Non-operative care, another operation or placebo. | F Follow-up Was outcome capture complete? | S Subgroups Was this subgroup powered or exploratory? |
O Outcome Function, reoperation, complications, mortality or cost. | E Endpoint Was the primary outcome clinically meaningful? | T Tradeoff What are the risks, costs and downstream procedures? |
No PICO, no application. | A famous trial can still have limits. | Cast evidence onto the actual patient. |
Overview
Landmark trials are studies that changed, challenged or clarified common orthopaedic decisions. They are most useful when they are remembered as clinical questions rather than as acronyms.
A good landmark-trial discussion should answer:
- What patient population was studied?
- What was the intervention and comparator?
- What primary outcome was used?
- What was the practice signal?
- What are the limitations and excluded patients?
- How should the result affect consent and management?
The complete one-sentence trial answer
“This trial asked whether intervention X compared with Y improved outcome Z in patient group P; the main signal was this, but I would not apply it automatically to these excluded or higher-risk patients.”
Concepts and Core Principles
What Makes a Trial Practice-Changing?
| Domain | Question | Why It Matters |
|---|---|---|
| Clinical relevance | Does the trial answer a decision surgeons face often? | Common decisions such as distal radius fixation or proximal humerus surgery affect many patients. |
| Internal validity | Were randomisation, allocation, follow-up and outcome assessment credible? | A flawed trial can mislead even if large. |
| Effect size | Is the difference clinically meaningful, not just statistically significant? | Small differences may not justify operative risk. |
| Applicability | Do the inclusion criteria match the patient in front of you? | A trial may exclude severe displacement, open injury, frailty or revision cases. |
| Downstream consequences | Did the trial capture reoperation, complications, cost and later crossover? | Orthopaedic decisions often have delayed consequences. |
Classification of Landmark Trials
Trial Style
| Style | Strength | Limitation |
|---|---|---|
| Explanatory trial | Tests whether an intervention can work under controlled conditions. | May not represent everyday surgical practice. |
| Pragmatic trial | Tests whether a strategy works in real clinical settings. | Treatment heterogeneity and crossover can dilute the result. |
Trauma Trials
Trauma Trial Signals
| Trial | Clinical Question | Practice Signal |
|---|---|---|
| DRAFFT | For adult dorsally displaced distal radius fractures, how do K-wires and volar locking plates compare? | Plate fixation was challenged as routine treatment for broad displaced distal radius fracture groups; cost, reoperation and patient selection matter. |
| DRAFFT 2 | After manipulation of dorsally displaced distal radius fractures, is K-wire fixation better than moulded cast? | Moulded cast was a serious comparator after acceptable reduction; avoid automatic fixation when stability and patient factors permit casting. |
| PROFHER | For displaced proximal humerus fractures in adults, does surgery improve patient-reported outcomes over non-operative care? | Routine surgery for many displaced proximal humerus fractures was strongly challenged; selected fracture patterns and younger/high-demand patients still need individual assessment. |
| FLOW | In open fractures, what irrigation pressure and solution should be used? | Very high pressure lavage did not become the default; soap solution raised concern. Normal saline and sensible pressure remain common practice anchors. |
| FAITH | For femoral neck fracture fixation, do sliding hip screws and cancellous screws differ? | Implant choice must be matched to fracture biology, displacement and patient factors; fixation failure remains central. |
| HEALTH | For displaced femoral neck fracture in independently ambulatory older adults, THA or hemiarthroplasty? | THA gave modest functional advantages in selected patients but with tradeoffs including dislocation; selection is key. |
| FORCE | For paediatric distal radius torus fractures, bandage or rigid immobilisation? | Simple bandage and discharge strategy is reasonable for uncomplicated torus fractures, reducing overtreatment. |
Trauma trial limitation
Fracture trials usually answer a strategy question for a defined injury group. They do not remove the need to assess displacement, soft tissue, bone quality, open injury, neurovascular status, patient demand and ability to comply with follow-up.
Sports and Knee Trials
Sports and Knee Trial Signals
| Trial | Clinical Question | Practice Signal |
|---|---|---|
| KANON | Early ACL reconstruction versus structured rehabilitation with optional delayed reconstruction. | Not every ACL rupture requires immediate reconstruction; instability episodes, goals, pivoting sport and meniscal risk guide individual decisions. |
| METEOR | Arthroscopic partial meniscectomy versus physical therapy in meniscal tear with osteoarthritis. | Physical therapy is a strong first-line option for many degenerative meniscal tears with OA; crossover matters. |
| FIDELITY | Arthroscopic partial meniscectomy versus sham surgery for degenerative meniscal tear. | Routine arthroscopic partial meniscectomy for degenerative meniscal symptoms without clear mechanical indication was strongly challenged. |
| MOON | Prospective ACL cohort evidence on outcomes, graft choice and predictors. | Useful for prognosis and counselling, but not a single randomised treatment rule. |
Degenerative meniscus discussion
The central counselling point is not “arthroscopy never works.” It is that high-quality evidence has narrowed the indication: degenerative meniscal symptoms with osteoarthritis usually need education, rehabilitation and non-operative care before considering arthroscopy, unless there is a specific mechanical problem or atypical scenario.
Arthroplasty Trials
Arthroplasty Trial Signals
| Trial | Clinical Question | Practice Signal |
|---|---|---|
| CRISTAL | Aspirin versus enoxaparin for symptomatic VTE prevention after hip or knee arthroplasty. | Enoxaparin performed better for symptomatic VTE in the trial context; prophylaxis choice must account for local protocol, bleeding risk and patient risk. |
| EPCAT II | After initial rivaroxaban, can aspirin continue extended prophylaxis after hip or knee arthroplasty? | Aspirin can be part of selected sequential prophylaxis pathways; do not confuse this with aspirin-only from day zero for all patients. |
| Registry signals | Which implants, bearings or fixation strategies survive in real-world use? | Registry findings are powerful for implant surveillance but remain observational and confounded. |
Spine Trials
Spine Trial Signals
| Trial | Clinical Question | Practice Signal |
|---|---|---|
| SPORT disc herniation | Surgery versus non-operative care for lumbar disc herniation. | Surgery can provide faster symptom relief for selected patients; long-term interpretation is affected by crossover. |
| SPORT spinal stenosis | Decompression strategy versus non-operative care for symptomatic lumbar stenosis. | Supports benefit of surgery in selected symptomatic stenosis, but patient selection and expectations matter. |
| SPORT degenerative spondylolisthesis | Surgery versus non-operative care for degenerative spondylolisthesis with stenosis. | Supports surgery for selected symptomatic patients, but treatment choice depends on instability, deformity and patient risk. |
Spine trial interpretation
Spine trials are highly affected by crossover, symptom severity, imaging-symptom correlation and patient preference. Quote the signal, then explain how patient selection changes the decision.
Clinical Relevance and Application
How to State a Landmark Trial in Practice
| Step | Good Answer | Weak Answer |
|---|---|---|
| Name the question | PROFHER studied surgery versus non-operative care for displaced proximal humerus fractures in adults. | PROFHER says no surgery. |
| Name the outcome | The key outcome was patient-reported function, not perfect radiographic anatomy. | The X-ray looks better after surgery. |
| Name the limitation | I would still individualise younger patients, fracture-dislocations, head-splitting injuries and clear surgical indications. | The trial applies to every proximal humerus fracture. |
| Translate to management | This evidence supports shared decision-making and avoids routine surgery in broad low-risk groups. | I quote the acronym and stop. |
Controversies and Areas of Uncertainty
Landmark trials answer a defined question, but several remain genuinely contested. Stating the controversy honestly is a marker of a strong candidate.
Live Debates Behind the Trials
| Area | The Tension | How to Frame It |
|---|---|---|
| Proximal humerus surgery | PROFHER challenged routine surgery, but it excluded fracture-dislocations and head-split patterns and enrolled mostly older patients. | The signal is against routine surgery for typical displaced fractures, not against surgery for clearly operative patterns or high-demand young patients. |
| VTE prophylaxis after arthroplasty | CRISTAL favoured enoxaparin while EPCAT II found extended aspirin acceptable after initial rivaroxaban; guidelines diverge. | Separate aspirin-from-day-zero from sequential aspirin, and stratify by individual VTE and bleeding risk. |
| Degenerative meniscectomy | FIDELITY and METEOR challenge routine arthroscopy, yet some patients with true mechanical symptoms still improve. | Reserve arthroscopy for genuine mechanical locking or a repairable tear after a proper rehabilitation trial. |
| Spine surgery selection | SPORT crossover blurs the randomised comparison, leaving the as-treated benefit open to interpretation. | Treat SPORT as support for shared decision-making in well-selected symptomatic patients, not proof for either extreme. |
| Pragmatic versus explanatory results | Pragmatic trials reflect real practice but heterogeneity and crossover can mask a real effect in a subgroup. | A negative pragmatic trial narrows but rarely abolishes an indication; look for prespecified subgroups. |
Differentiating Common Trial Confusions
Candidates frequently conflate trials with superficially similar questions. Keeping them distinct is high-yield.
Do Not Confuse These Trials
| Often Confused | Trial A | Trial B |
|---|---|---|
| Distal radius | DRAFFT: K-wires versus volar plate after a decision to fix. | DRAFFT 2: moulded cast versus K-wires after manipulation. |
| Meniscus | METEOR: meniscectomy versus physiotherapy WITH osteoarthritis. | FIDELITY: meniscectomy versus sham WITHOUT osteoarthritis. |
| Hip fracture implant choice | FAITH: sliding hip screw versus cancellous screws (fixation). | HEALTH: total hip arthroplasty versus hemiarthroplasty (replacement). |
| Arthroplasty VTE prophylaxis | CRISTAL: aspirin versus enoxaparin from the start. | EPCAT II: extended aspirin versus rivaroxaban after 5 days of rivaroxaban. |
Guidelines, Registries and Global Practice
Landmark trials are interpreted differently by major societies and are continuously cross-checked against arthroplasty registry data. Knowing where guidance converges and diverges is a global-exam expectation.
Side-by-Side Society Positions
| Question | Guidance Convergence | Where Practice Diverges |
|---|---|---|
| Proximal humerus fractures | AAOS and BOA / BOAST broadly support non-operative care for many displaced fractures, echoing PROFHER. | Thresholds for surgery in younger, high-demand patients and fracture-dislocations vary by region and surgeon. |
| Open fracture irrigation | BOA / BAPRAS open fracture standards and AO principles favour normal saline at low pressure and timely debridement, consistent with FLOW. | Antibiotic regimens and debridement timing targets differ between health systems. |
| VTE prophylaxis after arthroplasty | AAOS, NICE and ISTH all endorse routine pharmacological prophylaxis with individual risk assessment. | Aspirin monotherapy is more accepted in some North American pathways than in several European protocols after CRISTAL. |
| Degenerative meniscal tears | ESSKA and AAOS appropriate-use guidance discourage routine arthroscopy without mechanical symptoms. | Access to structured physiotherapy varies widely, shifting real-world thresholds for surgery. |
Why registries complement trials
Arthroplasty registries (NJR for England and Wales, AOANJRR in Australia, the Swedish and Norwegian registries, AJRR in the US, NZJR in New Zealand) capture implant survivorship, revision rates and rare complications across millions of procedures that no single randomised trial can power for. They are essential for the HEALTH-type question of dislocation and revision after hip-fracture arthroplasty.
High versus limited-resource practice
Trial conclusions assume access to physiotherapy, theatre time, implants and follow-up imaging. In limited-resource settings, a casting strategy (DRAFFT 2, FORCE) or non-operative pathway (PROFHER) may be even more attractive, while reliable structured rehabilitation (METEOR, KANON) can be the rate-limiting step rather than the operation.
Evidence Base
DRAFFT distal radius fixation
- DRAFFT randomised adults with a dorsally displaced distal radius fracture to K-wires versus volar locking plate and found no clinically relevant difference in the Patient-Rated Wrist Evaluation at 12 months.
- K-wires cost substantially less, so plate fixation was not justified as routine for this broad group.
- DRAFFT 2 (PMID 35152940) then showed moulded cast was equivalent to K-wires after acceptable manipulation, further discouraging routine surgery.
PROFHER proximal humerus
- 250 adults with a displaced proximal humerus fracture involving the surgical neck, randomised to surgery versus non-operative care.
- No difference in the Oxford Shoulder Score over two years, so surgery showed no patient-reported advantage in this population.
- The trial strongly challenged routine fixation for broad adult displaced proximal humerus fracture groups; the HTA report (PMID 25822598) confirmed surgery was also more costly.
FLOW open fracture irrigation
- 2447 patients with an open extremity fracture across 41 centres, randomised to high, low or very low irrigation pressure and to castile soap or normal saline.
- Reoperation within 12 months was similar across all three pressures (about 13 percent each), so very low pressure is an acceptable low-cost option.
- Soap produced more reoperations than saline (hazard ratio 1.32, 95 percent CI 1.06 to 1.66, P equals 0.01), favouring normal saline.
HEALTH femoral neck fracture
- 1495 independently ambulatory adults aged 50 or older with a displaced femoral neck fracture, randomised to total hip arthroplasty versus hemiarthroplasty.
- No significant difference in the primary outcome of secondary hip procedures within 24 months.
- THA gave small advantages in function and quality of life but a numerically higher dislocation rate, so patient selection remains central.
FAITH femoral neck fixation
- 1108 patients aged 50 or older with a low-energy hip fracture requiring fixation, randomised to a sliding hip screw versus multiple cancellous screws.
- No difference in 24-month reoperation (20 percent sliding hip screw versus 22 percent cancellous screws, hazard ratio 0.83, 95 percent CI 0.63 to 1.09).
- Avascular necrosis was more common with the sliding hip screw (9 versus 5 percent), but smokers and those with displaced or basicervical fractures may do better with it.
FORCE paediatric torus fracture
- 965 children aged 4 to 15 with a distal radius torus (buckle) fracture across 23 UK hospitals, randomised to the offer of a soft bandage and immediate discharge versus rigid immobilisation and follow-up.
- Pain at 3 days was equivalent (3.21 versus 3.14 on the Wong-Baker FACES scale, within the prespecified margin of 1.0).
- No difference in pain or function over 6 weeks, supporting a bandage-and-discharge strategy that reduces overtreatment.
Clinical Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Applying PROFHER
"An older adult presents with a displaced proximal humerus fracture. The radiograph is shown and the examiner asks whether PROFHER means surgery should never be offered."
Degenerative meniscal tear
"A patient with degenerative meniscal symptoms and osteoarthritis asks whether arthroscopy will fix the problem."
Arthroplasty prophylaxis
"A colleague says EPCAT II and CRISTAL prove aspirin is either always safe or never safe after arthroplasty."
Hip fracture implant choice
"An examiner asks how FAITH and HEALTH guide your management of an intracapsular femoral neck fracture in an older adult."
Landmark Trials: Key Takeaways
Clinical summary
How to quote
- •State patient group.
- •State intervention and comparator.
- •State primary outcome.
- •State practice signal and limitation.
Trauma
- •DRAFFT: distal radius fixation choices.
- •PROFHER: proximal humerus surgery challenged.
- •FLOW: open fracture irrigation evidence.
- •HEALTH: THA versus hemiarthroplasty tradeoffs.
- •FORCE: simple care for torus fracture.
Sports/Knee
- •KANON: ACL rehab-first strategy for selected patients.
- •METEOR: physical therapy strong for meniscus with OA.
- •FIDELITY: degenerative meniscectomy challenged by sham trial.
- •MOON: ACL cohort for prognosis and counselling.
Arthroplasty/Spine
- •CRISTAL and EPCAT II answer different prophylaxis questions.
- •SPORT supports selected spine surgery but crossover matters.
- •Registry signals are useful but observational.
Common errors
- •Overgeneralising.
- •Ignoring exclusions.
- •Forgetting the primary outcome.
- •Treating non-inferiority like superiority.
- •Using a trial as an automatic rule.