Lauge-Hansen Classification of Ankle Fractures
Never classify from the anteroposterior radiograph alone. The fibular fracture in SER stage II looks transverse on AP but is oblique on the lateral; missing the posterior malleolus or failing to recognise a high fibula (Maisonneuve) in pronation-external-rotation stage III changes both classification and fixation. Always restore the medial clear space and talar shift before deciding syndesmotic screws are unnecessary.
The Four Injury Patterns and Their Stages
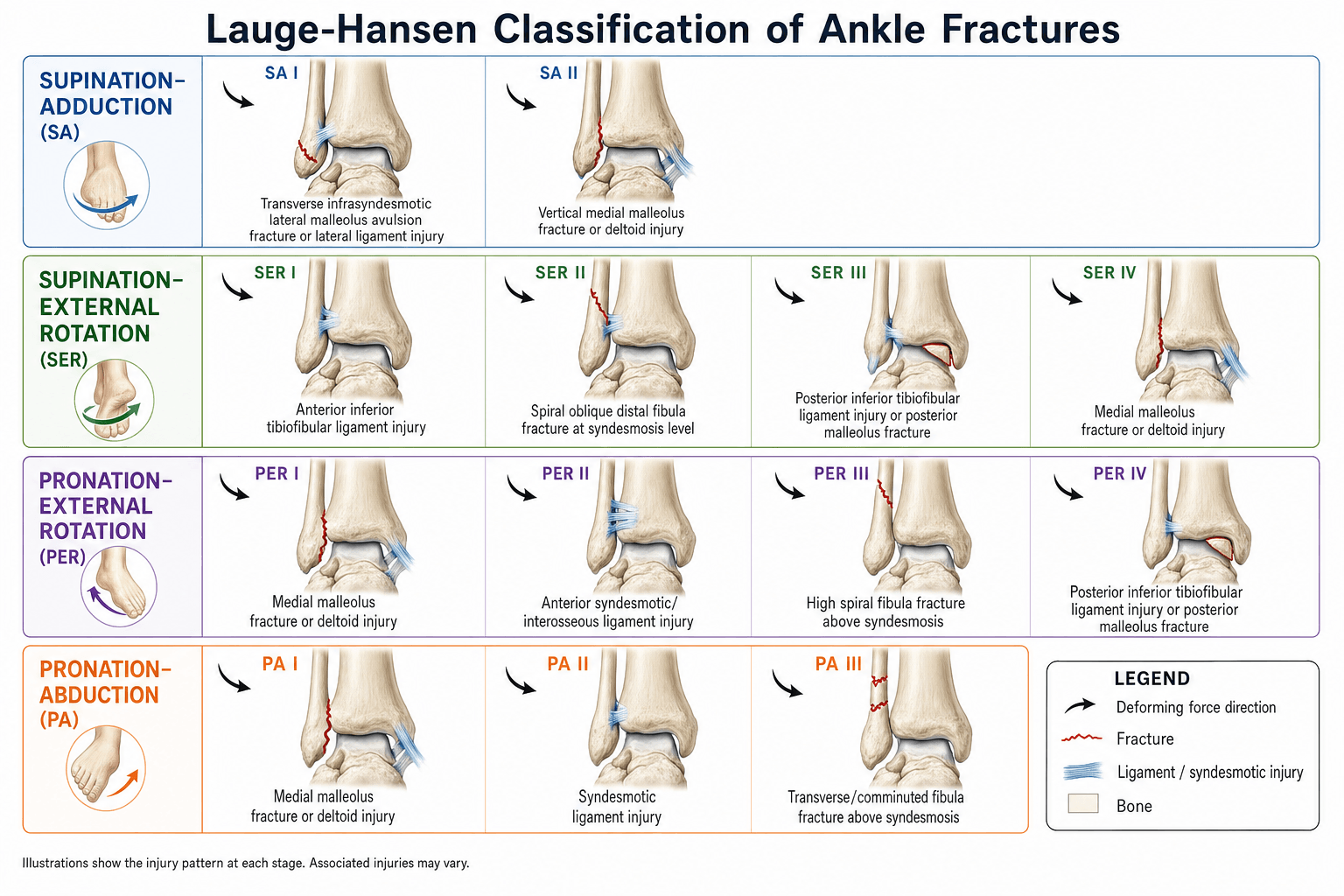
Lauge-Hansen describes four foot-position and force-direction combinations. Each pattern produces a predictable, staged sequence of soft-tissue then bony failure.
- Stage I
- Transverse lateral malleolus or ATFL tear
- Stage II
- Vertical medial malleolus fracture
- Stage III
- —
- Stage IV
- —
- Stage I
- AITFL tear or avulsion
- Stage II
- Oblique fibula fracture at syndesmosis level
- Stage III
- PITFL tear or posterior malleolus
- Stage IV
- Deltoid tear or medial malleolus fracture
- Stage I
- Transverse medial malleolus or deltoid tear
- Stage II
- AITFL and syndesmosis disruption
- Stage III
- Short oblique fibula fracture above syndesmosis with lateral comminution
- Stage IV
- —
- Stage I
- Transverse medial malleolus or deltoid tear
- Stage II
- AITFL and syndesmosis disruption
- Stage III
- High oblique fibula fracture (Maisonneuve possible)
- Stage IV
- PITFL or posterior malleolus fracture
SA • SER • PA • PER (foot position + force)The four patterns
Hook:First word = foot position (Supination vs Pronation), second = deforming force (Adduction/Abduction/External rotation). Supination injures the lateral side first; pronation injures the medial side first.

Anterior • Oblique • Posterior • MedialSER stages — the commonest
Hook:SER runs Anterior → Oblique fibula → Posterior → Medial — it travels around the ankle from front to back to medial.
The fibular fracture level on the lateral radiograph is the key to staging. In SER the fracture begins at the syndesmosis and spirals proximally; in PER the fracture is higher and the medial injury precedes the fibular fracture. A high fibular fracture with medial tenderness always prompts a full-length tibia radiograph to exclude a Maisonneuve injury.

Clinical Application and Reduction Principles
The classification directly informs closed reduction technique and the structures that must be restored at surgery.
- Key Reduction Move
- Direct medial buttress plating of vertical malleolus
- Structures Requiring Fixation
- Medial malleolus (buttress plate)
- Syndesmosis Likely?
- Rare
- Key Reduction Move
- Internal rotation of foot after fibular reduction
- Structures Requiring Fixation
- Fibula (plate), posterior malleolus if large, medial if unstable
- Syndesmosis Likely?
- Yes if stage III or IV
- Key Reduction Move
- Abduction stress then fibular plating with possible syndesmotic screw
- Structures Requiring Fixation
- Medial malleolus, fibula (often with intercalary fragment)
- Syndesmosis Likely?
- Yes
- Key Reduction Move
- External rotation correction then syndesmotic reduction
- Structures Requiring Fixation
- Medial, high fibula (often intramedullary or plate), posterior if unstable
- Syndesmosis Likely?
- Yes — almost always
SER III–IV • PA III • PER III–IVWhen to stabilise the syndesmosis
Hook:Any pattern reaching stage III–IV has torn the tibiofibular ligaments → assess and usually stabilise the syndesmosis after the fibula and medial side are fixed.
Reading the mortise: the measurements that define instability
Deciding "is the syndesmosis/deltoid intact?" rests on three reproducible measurements on a true mortise view (taken ~1 cm above the plafond), so know the normal values:
- Normal
- less than ~6 mm (AP and mortise)
- Suggests disruption
- greater than ~6 mm
- Note
- The MOST reliable sign of syndesmotic disruption (least affected by rotation)
- Normal
- greater than ~6 mm (AP) / greater than ~1 mm (mortise)
- Suggests disruption
- reduced or absent
- Note
- Lost overlap suggests syndesmotic widening (rotation-dependent)
- Normal
- less than ~4 mm, and ≤ the superior clear space
- Suggests disruption
- greater than ~4-5 mm
- Note
- Widening = deltoid/medial malleolus failure (talar shift)
The tibiofibular clear space is the single most reliable plain-film indicator of syndesmotic disruption because, unlike the overlap, it changes little with limb rotation. A normal-looking static mortise does not exclude instability, so an external-rotation stress or gravity-stress view (or intra-operative hook test) is used when a Weber B / SER injury is "stable-looking" but the deltoid is in question.
After anatomic fibular reduction and medial repair, test syndesmotic stability with the hook test or external rotation stress under fluoroscopy. Persistent widening greater than 2 millimetres on the mortise view after fixation indicates the need for a syndesmotic screw or suture-button construct.
Knowing the Haraguchi morphology is only useful if you know what to do with it:
- Traditional rule: fix the posterior malleolus when it involves more than about 25-33% of the articular surface on the lateral radiograph (large fragments leave the talus prone to posterior subluxation and articular incongruity).
- Modern shift: the decision is increasingly driven by fragment morphology, articular step-off and the contribution to SYNDESMOTIC stability rather than size alone — because the posterior fragment carries the posterior-inferior tibiofibular ligament (PITFL) and reconstitutes the posterior incisura, so fixing even a smaller posterolateral fragment can restore syndesmotic stability and may obviate a separate syndesmotic screw.
- Approach by Haraguchi type: a posterolateral-oblique (type I) fragment is reached through a posterolateral approach; a medial-extension (type II) fragment that runs into the medial malleolus may need a posteromedial approach — which is exactly why preoperative CT (not plain films) plans the fixation.
The single most important determinant of outcome in a syndesmotic injury is ANATOMIC reduction — and malreduction is the commonest avoidable error, present in a substantial proportion of fixations and under-detected on intra-operative fluoroscopy (a postoperative or intra-operative CT, ideally compared with the uninjured side, is far more sensitive).
- Screw fixation: a rigid 3.5/4.5 mm screw through 3 or 4 cortices, placed roughly 2-4 cm above the plafond and angled about 30° from posterolateral to anteromedial, with the ankle held in neutral dorsiflexion (not plantarflexion) to avoid over-tightening/over-compression; routine elective removal and the timing of weight-bearing remain debated.
- Suture-button (dynamic) fixation: allows physiological micromotion and is associated with lower malreduction and hardware-removal/reoperation rates and at least comparable functional outcomes — increasingly preferred.
- Whatever the construct, confirm the reduction, not just the stability — a stable but malreduced syndesmosis still does badly.
Limitations and Modern Context
- The original description was based on cadaveric sectioning and does not account for combined or atypical mechanisms seen in high-energy trauma.
- Inter-observer reliability is only moderate for exact stage assignment once the medial injury is reached; the fibular fracture pattern on the lateral view is the most reproducible element.
- CT is now routine for assessing the posterior malleolus and syndesmosis and frequently refines the operative plan (fragment size, morphology and approach) beyond what plain-film staging predicts.
- Modern locking plates and minimally invasive techniques have reduced the need for perfect anatomic reduction of every fragment, yet the ligament sequence still dictates which structures must be addressed.
- The classification remains valuable for teaching reduction logic even though fixation decisions increasingly incorporate CT and intra-operative stress examination.
- Danis-Weber is the everyday companion classification. Weber grades the fibular fracture purely by its level relative to the syndesmosis — A below (≈ SA, syndesmosis intact), B at the level (≈ SER, variable syndesmosis), C above (≈ PA/PER, syndesmosis disrupted, higher fibula = more unstable). Weber is simpler and quicker for communication and broadly maps to syndesmotic risk, whereas Lauge-Hansen adds the mechanism and the ligament sequence; many surgeons quote both. The AO/OTA system further subdivides Weber. Stability — not the label alone — drives the decision to operate (a Weber B / SER injury is the classic "is the deltoid intact?" stability question, answered by the medial clear space and stress views).
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 35-year-old footballer presents after an inversion injury. The mortise radiograph shows an oblique fibular fracture at the level of the syndesmosis with 3 millimetres of medial clear-space widening. What is the Lauge-Hansen stage and what fixation is required?”
“A 42-year-old pedestrian is struck by a car. The AP radiograph shows a transverse medial malleolus fracture and a high fibular fracture 12 centimetres above the joint. What is the Lauge-Hansen classification, and what additional imaging and fixation decisions follow?”
The four patterns and hallmark features
- SA: vertical medial malleolus after transverse lateral ligament or bone injury
- SER (commonest): anterior ligament, spiral fibula, posterior ligament, medial injury
- PA: medial transverse first, then syndesmosis, then high fibula with lateral comminution
- PER: medial first, syndesmosis, very high fibula (Maisonneuve), posterior injury
Key radiographic signs
- Oblique fibula at syndesmosis level on lateral view equals SER stage II or higher
- Medial clear-space widening greater than 4 millimetres indicates deltoid or medial malleolus failure
- High fibular fracture demands full-length tibia radiograph
- Posterior malleolus fragment on lateral view indicates stage III or IV
Fixation implications
- SER and PER stage III–IV almost always need syndesmotic stabilisation after fibular plating
- SA stage II vertical medial malleolus requires buttress plate, not simple screws
- PA stage III often needs syndesmotic screw plus attention to intercalary fibular fragment
- Test syndesmosis after every fibular reduction — do not rely on classification alone
Evidence Base
All four citations were verified against PubMed. The system rests on Lauge-Hansen's 1950 cadaveric work (the mechanistic framework) and Yde's 488-fracture clinical series (confirming SER as the dominant pattern, ~57%, and noting that stage II of the pronation patterns is not fully explained by the original scheme). The crucial caveat is Nielsen's reproducibility study: four observers agreed completely on only 51 of 118 fractures — so the exact stage is only moderately reproducible and should be corroborated with the lateral film and intra-operative stress, not asserted from the AP view alone. Haraguchi's CT study is the modern refinement, showing the posterior malleolar fragment is highly variable (posterolateral-oblique 67%, medial-extension 19%, small-shell 14%) and justifying preoperative CT. Net: Lauge-Hansen is an outstanding teaching framework for reduction logic, but operative decisions increasingly rest on CT and stress testing.
Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations
- Original cadaveric study defining the four foot-position and force combinations
- Demonstrated the staged, sequential failure of specific ligaments before bone
- Established that the fibular fracture pattern reflects the mechanism and stage
The Lauge Hansen classification of malleolar fractures
- Series of 488 malleolar fractures classified by Lauge-Hansen type, partly based on operative findings
- Supination-eversion (SER) was the commonest pattern (57.4%); supination ~20.1% and pronation/pronation-eversion ~20.1%
- The classification gives an exact description useful for operative treatment, though stage II of the pronation patterns is not fully explained by Lauge-Hansen
Lauge-Hansen classification of malleolar fractures. An assessment of the reproducibility in 118 cases
- Four observers classified 118 malleolar-fracture radiographs by the Lauge-Hansen system
- Large interobserver variation — only 51 of 118 (43%) were classified identically by all four observers
- Intraobserver agreement was 64-82%; the authors concluded the system is difficult to apply reproducibly
Pathoanatomy of posterior malleolar fractures of the ankle
- CT study of 57 posterior malleolar fractures, categorised into three types by the fracture-line location
- Posterolateral-oblique type 67%, medial-extension type 19% (can extend into the medial malleolus), and small-shell type 14%
- Fracture configurations were highly variable, so preoperative CT is justified to plan the surgical approach