Compartments of the Leg
Compartment syndrome is a clinical emergency, but its treatment is anatomical: every one of the four compartments must be opened. Knowing the contents lets you confirm decompression (e.g. you can see tibialis posterior in the deep posterior compartment) and protect the structures at the incisions.
The deep peroneal nerve (anterior) and first web space sensation are early in anterior ACS. At the posteromedial incision protect the saphenous vein and nerve; the deep posterior compartment is the one most often left inadequately released.
Overview
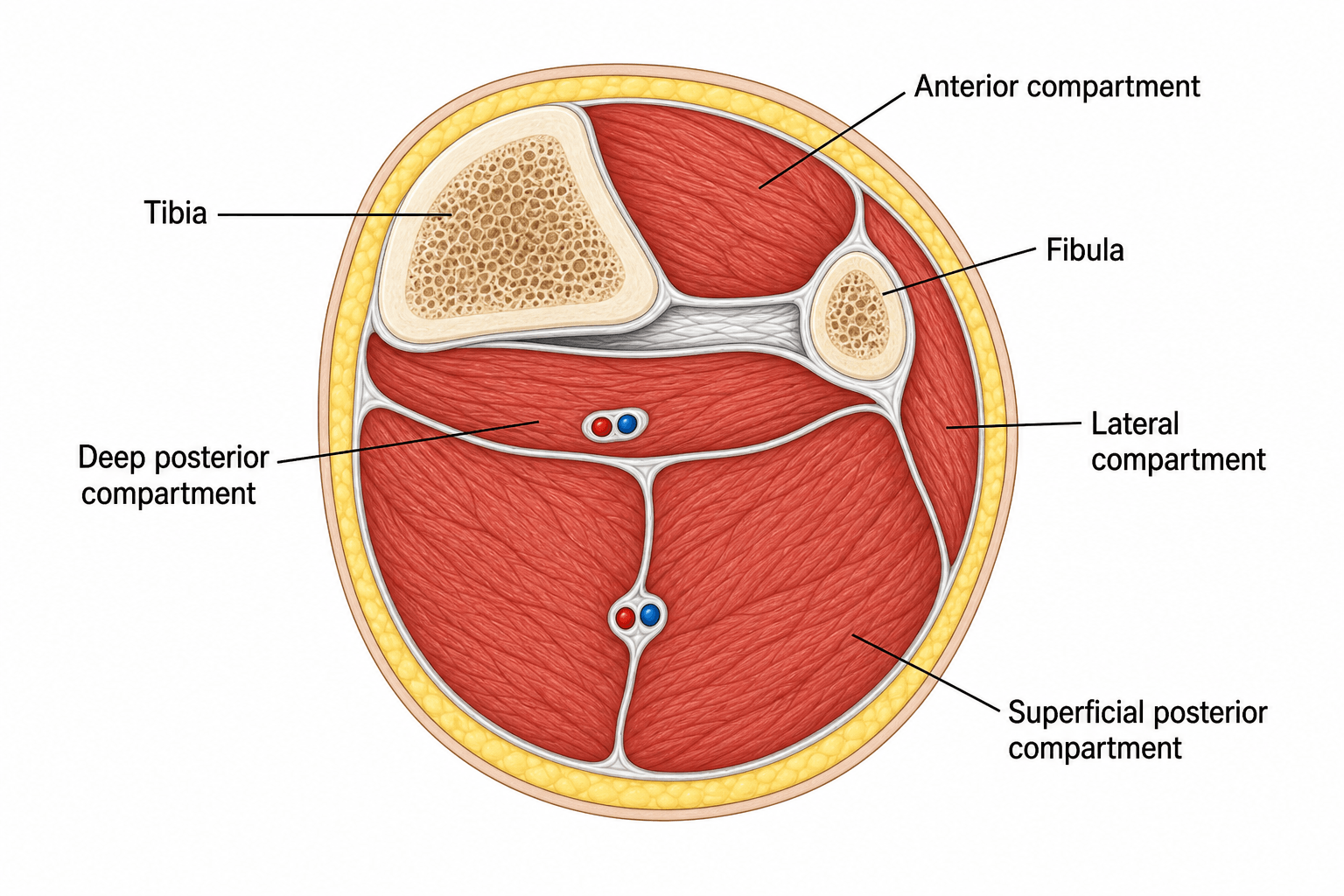
The leg is divided into four osteofascial compartments by the tibia, fibula, the interosseous membrane and the anterior and posterior intermuscular septa. Each is a relatively inelastic box containing a functional muscle group with its motor nerve and (with one exception) a named artery — and it is precisely this inelasticity that makes the leg the classic site of acute compartment syndrome. The exam value of the anatomy is therefore inseparable from the emergency it underlies: you learn the contents so you can recognise which function and sensation fail first, confirm that every box has been opened at fasciotomy, and protect the structures that lie at the decompression incisions. Hold three layers together — the contents of each compartment, the clinical syndrome (pain on passive stretch, the differential-pressure threshold), and the operation (a two-incision four-compartment release).
The Four Compartments
Anterior Compartment
- Muscles: tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius.
- Nerve: deep peroneal (fibular) nerve.
- Artery: anterior tibial artery.
- Action: ankle dorsiflexion and toe extension.
- Note: the most common compartment to develop acute compartment syndrome; bordered by the tibia, fibula, interosseous membrane and anterior intermuscular septum.
Know which fascial wall separates which compartment — the examiner will make you draw it. The four boxes are bounded not just by the tibia and fibula but by named fascial structures: the deep (crural) fascia forms the outer envelope; the interosseous membrane separates the anterior compartment from the deep posterior; the anterior intermuscular septum (fibula to deep fascia) separates the anterior from the lateral compartment; the posterior intermuscular septum separates the lateral from the superficial posterior compartment; and the transverse intermuscular septum separates the superficial posterior (gastroc-soleus) from the deep posterior compartment. Drawing this correctly also explains the incisions: the anterolateral fasciotomy is placed over the anterior intermuscular septum so one skin incision reaches both the anterior and lateral boxes, and the posteromedial incision lies behind the medial tibia to reach the superficial and (through the transverse septum) the deep posterior boxes. The exam point: each compartment is a fascial box with a specific wall between it and its neighbour — name the septa, not just "intermuscular septa."
Neurovascular Contents by Compartment
The single highest-yield table in this topic — know the muscles, nerve, artery and action of each compartment cold, because the examiner will ask you to recite them and then link each to a clinical deficit.
- Muscles
- TA, EHL, EDL, peroneus tertius
- Nerve
- Deep peroneal
- Artery
- Anterior tibial
- Action
- Dorsiflexion
- Deficit if affected
- Foot drop; lost first-web-space sensation (earliest in ACS)
- Muscles
- Peroneus longus & brevis
- Nerve
- Superficial peroneal
- Artery
- (perforators)
- Action
- Eversion
- Deficit if affected
- Weak eversion; lost dorsolateral foot sensation
- Muscles
- Gastrocnemius, soleus, plantaris
- Nerve
- Tibial (muscles); sural (cutaneous)
- Artery
- Sural/perforators
- Action
- Plantarflexion
- Deficit if affected
- Weak push-off
- Muscles
- Tibialis posterior, FDL, FHL, popliteus
- Nerve
- Tibial
- Artery
- Posterior tibial + peroneal
- Action
- Inversion, toe flexion
- Deficit if affected
- Clawed toes, lost sole sensation (most often MISSED at fasciotomy)
ALSDLeg Compartment Contents
Hook:Four compartments A-L-S-D; the deep peroneal nerve (anterior) and first web space fail first in ACS.
Surgical Relevance: Fasciotomy
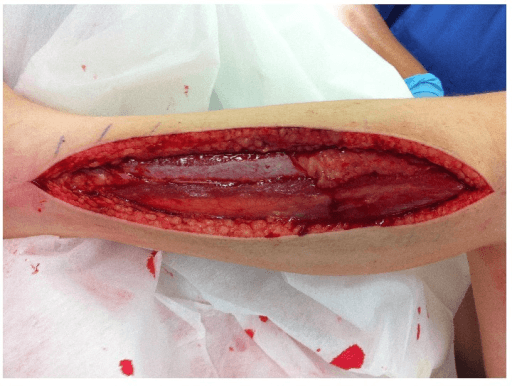
The standard surgical decompression of the leg is the two-incision technique, releasing all four compartments. Failure to release every compartment is the commonest reason a fasciotomy fails.
- Anterolateral incision (lateral to the tibial crest, centred over the anterior intermuscular septum): decompresses the anterior and lateral compartments. Identify the septum and the superficial peroneal nerve in the distal lateral compartment.
- Posteromedial incision (about 1-2 cm posterior to the medial tibial border): decompresses the superficial and deep posterior compartments - protect the saphenous vein and nerve, and ensure the deep posterior compartment (tibialis posterior) is genuinely released.
- A single-incision perifibular (Matsen) technique can release all four compartments through one long lateral incision over the fibula, but it is more demanding, gives poorer access to the deep posterior compartment, and risks the superficial peroneal nerve — the two-incision technique is preferred for completeness and is the safer answer in a viva.
- Whichever technique, incisions must be generous (typically the length of the leg segment) — short skin incisions cause skin-level constriction and an incomplete release.
- Wounds are left open and managed with delayed closure or skin grafting.

The "fifth compartment" — tibialis posterior in its own fascial sheath. A recurring anatomical reason the deep posterior compartment is the one most often left under-decompressed is that tibialis posterior frequently lies in its own separate fascial subcompartment within the deep posterior space (some describe it as the "fifth compartment of the leg"). Opening the deep posterior fascia and seeing FDL and FHL is therefore not enough — the tibialis posterior sheath must be specifically identified and released along the back of the tibia, or it can remain tight and ischaemic despite an apparently complete fasciotomy. The practical drill at the posteromedial incision: after releasing the superficial posterior (gastroc-soleus) and the main deep posterior fascia, deliberately detach soleus from the posteromedial tibia, follow the neurovascular bundle, and confirm the tibialis posterior fascia itself is opened. The exam point: the deep posterior compartment is functionally subdivided, so "I released the deep posterior compartment" must include the tibialis posterior sheath.
Clinical Correlations: Acute Compartment Syndrome
Acute compartment syndrome (ACS) results from raised pressure within a closed osteofascial compartment that exceeds capillary perfusion pressure, producing ischaemia, muscle and nerve necrosis, and ultimately an unsalvageable limb if not decompressed. It is the clinical reason the compartment anatomy matters.
Causes: most commonly a tibial diaphyseal fracture (the single commonest cause), but also crush injury, reperfusion after vascular injury/ischaemia, a tight cast or dressing, burns with circumferential eschar, high-energy soft-tissue injury, bleeding (anticoagulation/coagulopathy), and extravasation. It can occur with open fractures — an open wound does NOT decompress all compartments and does not exclude ACS.
Diagnosis is clinical
The earliest and most reliable findings are pain out of proportion to the injury and pain on passive stretch of the muscles in the affected compartment. A tense, swollen compartment supports the diagnosis. The classic "5 P's" are LATE and unreliable — by the time they appear the limb is often already lost.
- Sign
- Pain out of proportion + pain on passive stretch
- Note
- The two findings to act on; a tense compartment supports it
- Sign
- Paraesthesia (nerve ischaemia)
- Note
- First-web-space numbness in anterior ACS (deep peroneal nerve)
- Sign
- Paralysis, Pallor, Pulselessness
- Note
- Late and unreliable — a palpable pulse does NOT exclude ACS
Intracompartmental pressure measurement
Where the patient is obtunded, anaesthetised, a child, or the picture is equivocal, measure intracompartmental pressure (within about 5 cm of the fracture, all compartments). Act on the differential (delta) pressure rather than the absolute value:
ΔP = diastolic blood pressure − measured compartment pressure. A ΔP of 30 mmHg or less is the threshold for fasciotomy. Using the differential pressure (which accounts for the patient's perfusion pressure) rather than an absolute pressure threshold avoids both missed cases and unnecessary fasciotomies — in McQueen & Court-Brown's prospective tibial-fracture series a ΔP threshold of 30 mmHg missed no cases, whereas an absolute threshold of 30 mmHg would have led to a 43 percent (unnecessary) fasciotomy rate.
Timing and complications
Decompression should be as early as possible (ideally within 6 hours); irreversible muscle necrosis follows prolonged ischaemia. Complications of missed or delayed ACS include Volkmann's ischaemic contracture (fibrotic, contracted, functionless muscle), rhabdomyolysis with acute kidney injury and hyperkalaemia, infection, amputation, and death. A very late presentation (established necrosis, typically beyond 36–48 hours) is one situation where fasciotomy may be withheld, because opening dead muscle risks fatal infection — a difficult, senior decision. Missed ACS is one of the commonest sources of successful orthopaedic litigation, so document serial examinations and act decisively.
The P's — but only the first two are earlySigns of acute compartment syndrome
Hook:Act on the first two P's (pain out of proportion + pain on passive stretch). If you wait for pallor, pulselessness and paralysis, the limb is already lost.
Guidelines, Registries & Global Practice
Global Practice Picture
Leg compartment anatomy is universal core knowledge for trauma and the basis of fasciotomy. The internationally consistent teaching: know the four compartments and their contents, diagnose acute compartment syndrome clinically (pain out of proportion, pain on passive stretch) with pressure measurement when equivocal, and decompress all four compartments emergently - most reliably via the two-incision technique. (The full neurovascular contents are tabulated in the Neurovascular Contents by Compartment section above.)
Evidence Base
The two review articles below frame ACS as a time-critical, medicolegally fraught clinical diagnosis. The pivotal primary paper for the exam is McQueen & Court-Brown's prospective tibial-fracture study, which established the differential-pressure (ΔP ≤ 30 mmHg) threshold now used worldwide — quote it whenever you are asked how to interpret a compartment pressure. The recurring evidence theme across all three is that history and examination cannot reliably exclude ACS, so a low threshold for serial review (and pressure measurement in the obtunded) is essential.
Compartment monitoring in tibial fractures. The pressure threshold for decompression
- Prospective continuous anterior-compartment monitoring of 116 tibial diaphyseal fractures
- Acute compartment syndrome occurred in 3 patients (2.6%)
- A differential pressure (diastolic minus compartment pressure) threshold of 30 mmHg missed no cases of ACS
- An absolute pressure threshold of 30 mmHg would have led to a 43 percent unnecessary fasciotomy rate
Acute lower-leg compartment syndrome
- Reviews diagnosis of acute compartment syndrome of the lower leg
- Diagnosis is not always straightforward and carries a high risk of limb morbidity if missed or delayed
- Failure to diagnose and treat is among the most common causes of successful medical liability claims
- Discusses intracompartmental pressure measurement and emerging non-invasive diagnostic technologies
Evaluation and Management of Acute Compartment Syndrome in the Emergency Department
- Acute compartment syndrome most commonly follows fractures or trauma to the involved area
- Pain out of proportion and pain on passive stretch are early findings; pulselessness/paralysis are late
- History and examination are unreliable to rule out the diagnosis; intracompartmental pressure measurement is the most reliable test
- Treatment is emergent fasciotomy with resuscitation and management of complications such as rhabdomyolysis