Adolescent Lumbar Avulsion | Limbus Vertebra | Mimics Disc Herniation | Bony Canal Compromise
- Posterior ring apophysis is unfused in adolescents (ossification continues to age 18-25) and is the weak point for avulsion
- Most common at L4-S1 levels in athletic adolescents with flexion/compression injury
- CT scan is the imaging of choice - shows the displaced bony fragment and canal compromise
- Mimics disc herniation clinically but contains BONE - neurologic deficit is common due to bony compression
- Treatment is fragment + disc excision (laminotomy/laminoplasty); fusion reserved for instability or recurrence
- “Suspect in an athletic adolescent with radiculopathy - this is NOT typical disc herniation
- “CT shows the displaced bony fragment - MRI alone may miss the calcified/ossified component
- “Fragment includes bone, cartilage and disc material - must excise all three for decompression
- “Delayed diagnosis is common - average 6-12 months from symptom onset in published series
Posterior ring apophysis is a secondary ossification centre at the posterior vertebral body rim. It fuses by age 18-25 (last to fuse in the spine). In adolescents it is the weakest link under flexion/compression load and avulses into the canal.
Presents like a lumbar disc herniation - radiculopathy, positive SLR, sometimes cauda equina syndrome. Key difference: it occurs in athletic adolescents, the fragment is BONY, and symptoms often follow a discrete flexion injury or repetitive sport (gymnastics, football, weightlifting).
CT scan is the gold standard for diagnosis. Demonstrates the displaced posterior bony fragment, its size, and the percentage of canal compromise. MRI assesses disc hydration, fragment composition (bony vs cartilaginous), and neural element compression.
Excise the fragment and the associated disc material via laminotomy or interlaminar approach. The fragment must be mobilised off the dura, often requiring a fine curette or pituitary rongeur. Fusion is reserved for instability or recurrent herniation.
- Diagnosis
- CT shows displaced posterior bony fragment
- Treatment
- Fragment + disc excision via laminotomy
- Key Pearl
- Fusion rarely needed; preserve motion segment
- Diagnosis
- MRI + CT confirms bony fragment with disc
- Treatment
- Decompression alone, no fusion in most cases
- Key Pearl
- Recurrence uncommon (under 10 percent)
- Diagnosis
- Urgent CT/MRI, then urgent decompression
- Treatment
- Emergency fragment excision + decompression
- Key Pearl
- Time-critical - decompress within 48 hours
APEXApophyseal Ring Fracture Anatomy
Hook:Think APEX - the adolescent ring apophysis is the weak APEX that avulses into the canal!
DISCSurgical Excision Steps
Hook:DISC excision - decompress, identify, separate, confirm root mobility!
Overview and Epidemiology
Posterior vertebral apophyseal ring fracture is a frequently missed diagnosis. It presents in athletic adolescents with the clinical picture of a disc herniation, but the compressive lesion is a BONE FRAGMENT plus disc material. Plain radiographs are typically normal, MRI may underestimate the bony element, and a CT scan is required to make the diagnosis. Delayed treatment increases the risk of permanent neurological deficit.
- Age: 13-18 years (range 8-25), peak 14-16 in athletic adolescents
- Sex: Male predominance (approximately 2:1) reflecting sport exposure
- Levels: L4-S1 in 70-80 percent (lower lumbar mobile segments)
- Mechanism: Forced flexion with axial load, often sporting injury
- Radiculopathy: 80-90 percent of symptomatic cases
- Motor weakness: 30-50 percent at presentation
- Cauda equina: Less than 5 percent but well-described
- Time to diagnosis: Often 3-12 months from symptom onset
The term limbus vertebra describes the benign, usually incidental end of this spectrum and must be distinguished from the symptomatic posterior apophyseal ring fracture this page covers. A limbus vertebra is intervertebral disc material herniating through the ring apophysis before it fuses, separating a small, triangular, well-corticated ossicle from the vertebral body corner - classically the anterosuperior corner (and a recognised feature of Scheuermann disease and repetitive flexion loading). It is typically asymptomatic, found incidentally, and needs no treatment; its importance is as a "don't-touch" mimic - the smooth, corticated separate fragment with adjacent disc material distinguishes it from an acute fracture, an infective corner lesion, or an aggressive tumour, and recognising it avoids over-investigation. The posterior ring fracture, by contrast, displaces into the canal and is symptomatic (radiculopathy, canal compromise) because of where it goes, not because it is a different lesion. Same mechanism, opposite clinical significance - location is everything.
Pathophysiology
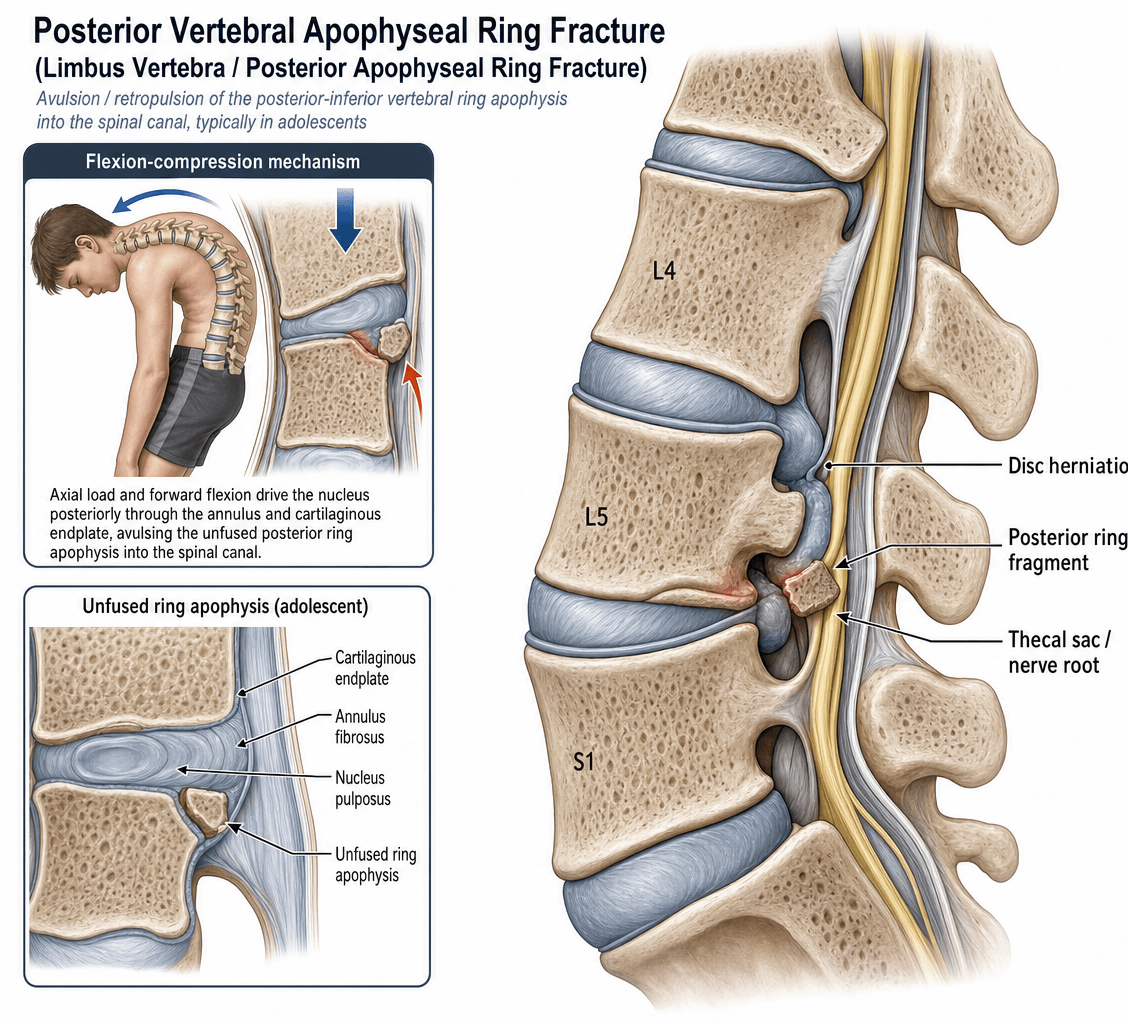
The posterior ring apophysis is a secondary ossification centre at the posterior vertebral body margin. It appears around age 6-8 and fuses with the vertebral body by age 18-25 (one of the last skeletal fusion events in the body). While unfused, it is a cartilaginous synchondrosis and the mechanical weak point of the motion segment. Under flexion with axial load, the nucleus pulposus drives the disc material posteriorly, levering off a posterior corner of the ring apophysis into the spinal canal. The avulsed fragment contains cortical bone, cancellous bone, cartilage from the apophysis, and disc material - it is therefore larger and harder than a typical disc extrusion.
- Apophyseal Ring Fracture
- 13-18 years (apophysis unfused)
- Typical Disc Herniation
- 30-50 years (disc degenerate)
- Apophyseal Ring Fracture
- Bony fragment + cartilage + disc
- Typical Disc Herniation
- Disc material (soft tissue)
- Apophyseal Ring Fracture
- Displaced posterior bony fragment
- Typical Disc Herniation
- No bony fragment, soft tissue only
- Apophyseal Ring Fracture
- Poor - bony fragment will not resorb
- Typical Disc Herniation
- Often improves over 6-12 weeks
- Apophyseal Ring Fracture
- Approximately 70-80 percent
- Typical Disc Herniation
- Approximately 10-15 percent
Forced flexion + axial load in an adolescent athlete:
- Nucleus pulposus under high pressure drives posteriorly
- Posterior ring apophysis (cartilaginous) avulses
- Fragment includes bone, cartilage, and disc material
- Fragment displaced into spinal canal
- Compression of dural sac and/or exiting nerve root
Common sports: football, gymnastics, weightlifting, wrestling
Bone does not resorb spontaneously.
- Soft disc herniations can shrink over 6-12 months
- Bony fragments remain in the canal as a fixed compressive lesion
- Inflammatory reaction around bone can worsen symptoms
- Time to surgical decompression is the only modifiable prognostic factor
Indication for surgery is therefore often established at presentation.
Classification and Types
Takata Classification (1988)
The most widely used classification of posterior apophyseal ring fractures, based on CT appearance of the fragment and its relationship to the vertebral body.
- Description
- Avulsion of central cartilaginous node, no cortical bone
- Bony Content
- Cartilage only
- Surgical Approach
- Simple excision; rarely requires bone work
- Description
- Avulsion of posterior rim fragment (cortical + cancellous)
- Bony Content
- Cortical and cancellous bone + cartilage
- Surgical Approach
- Interlaminar approach, fragment removal + disc excision
- Description
- Large osseous fragment, includes vertebral body corner
- Bony Content
- Substantial bone from posterior vertebral body
- Surgical Approach
- May need wider exposure, fragment mobilisation off dura
Type II is the most common. Type I is the least common and is sometimes considered a separate entity (Schmorl-type central herniation).
TYPETakata Classification
Hook:TYPE I-III - always excise the TYPE of fragment along with the disc!
Clinical Assessment
- Age: Adolescent (13-18 years)
- Sport: Football, gymnastics, weightlifting, wrestling, rugby
- Onset: Often discrete injury with flexion/axial load
- Pain: Radicular leg pain (greater than back pain)
- Neurologic symptoms: Numbness, weakness, gait disturbance
- Spine: Reduced flexion, paravertebral spasm, scoliosis (antalgic)
- SLR: Limited on affected side, often under 60 degrees
- Neurologic: Dermatomal sensory loss, myotomal weakness
- Cauda equina screen: Saddle anaesthesia, sphincter disturbance
Adolescents do not get disc herniations (or very rarely). Any adolescent with radiculopathy, motor weakness, or persistent pain beyond 4-6 weeks requires cross-sectional imaging. A diagnosis of "muscular back pain" in a teenager with radiculopathy and positive SLR should prompt CT and MRI to exclude apophyseal ring fracture. Plain radiographs miss the lesion in most cases.
- Age
- 13-18 years
- Imaging Finding
- Displaced posterior bony fragment on CT
- Discriminating Feature
- Sport history, hard compression, bony lesion
- Age
- 13-21 years
- Imaging Finding
- Disc extrusion without bony fragment
- Discriminating Feature
- Purely soft tissue lesion on MRI
- Age
- 10-18 years
- Imaging Finding
- Pars defect on oblique X-ray / CT
- Discriminating Feature
- Extension-related back pain, hamstring tightness
- Age
- 12-16 years
- Imaging Finding
- Anterior wedging, Schmorl nodes
- Discriminating Feature
- Thoracic kyphosis, fixed round back
- Age
- Any age
- Imaging Finding
- Lesion on CT/MRI
- Discriminating Feature
- Night pain, NSAID-responsive (osteoid osteoma)
- Age
- Adolescent to adult
- Imaging Finding
- Negative spine imaging
- Discriminating Feature
- SI joint tenderness, positive Patrick / FABER test
A young athlete with radiculopathy who has not responded to 4-6 weeks of conservative care needs cross-sectional imaging. MRI alone is insufficient - it can miss the calcified or ossified element of the fragment and underestimate the size of the bony component. Always add a thin-slice CT (or CT myelogram) before planning surgery. The fragment is harder than a disc and requires different instrumentation (pituitary rongeur, fine osteotome, high-speed burr) to mobilise.
The posterior apophyseal ring fracture and the pars interarticularis stress fracture (spondylolysis) arise in the same adolescent athlete from the same repetitive flexion-extension and axial overload, and the two are recognised to co-exist - a young athlete can have both a canal-compromising ring fragment and a pars defect at the same or an adjacent level. This matters because it changes the work-up and the plan: the thin-slice CT obtained for the ring fragment should be reviewed for a pars defect (and a SPECT or MRI STIR can show an active, healing-capable pars stress reaction), and a co-existing pars defect with any listhesis raises the question of segmental instability - influencing whether a decompression should be accompanied by stabilisation/fusion rather than fragment excision alone, and lengthening the return-to-sport timeline. So in the adolescent athlete, do not stop at the ring fragment - actively look for spondylolysis on the same imaging.
Investigations
Imaging Protocol
Views: AP, lateral, oblique of lumbar spine
Look for: Displaced posterior vertebral body corner, loss of disc height, scoliotic list
Limitation: Misses the fragment in over 80 percent of cases - the bony fragment is often only 2-5 mm and is obscured by overlapping structures
Indication: Any adolescent with radiculopathy not responding to 2-4 weeks of conservative care
Technique: Thin-slice (1 mm) axial with sagittal and coronal reformats
What it shows: Displaced posterior bony fragment, its size, shape, and position within the canal; relationship to nerve roots
Advantage: Defines the bone - surgical planning depends on it
Indication: Assess disc hydration, neural element compression, and rule out other pathology
Sequences: T2 sagittal and axial, T1 axial, STIR (for oedema)
What it shows: Disc desiccation, extruded disc material, neural element compression, sometimes the bony fragment as low signal
Limitation: Underestimates bony element; supplement with CT
Indication: When MRI is contraindicated or when CSF leak suspected
What it shows: Block of contrast column, dural compression, root cut-off
Use: Largely supplanted by MRI + CT in modern practice
The CT scan is the single most useful investigation. It answers the two key surgical questions: where is the fragment? and how big is the bony element? MRI complements by showing the soft tissue (disc) component and the neural elements. Most published surgical series plan the approach from the CT, not the MRI.
- CT Scan
- Excellent - shows the calcified/ossified element
- MRI
- Moderate - may underestimate bony component
- CT Scan
- Indirect (non-enhancing soft tissue)
- MRI
- Excellent - shows hydrated disc, extrusion
- CT Scan
- Indirect (canal compromise percentage)
- MRI
- Excellent - direct visualisation of roots and sac
- CT Scan
- Primary modality - approach and instrument choice
- MRI
- Adjunct - confirms disc, soft tissue, root position
- CT Scan
- Yes (modest, lumbar-limited)
- MRI
- No

Management Algorithm
Initial Non-Operative Care (Selected Cases)
Goal: Allow symptoms to settle; consider in mild cases with small fragments and no significant deficit
Treatment Protocol
Activity restriction: No sport, no heavy lifting
Analgesia: NSAIDs, paracetamol, short course oral steroids if radiculopathy severe
Education: Avoid flexion, avoid axial loading
Physiotherapy: Core stabilisation, neural gliding (gentle)
Monitor: Pain, neurology, function
Failure indicators: Persistent radiculopathy, progressive deficit, intolerance of activity
CT/MRI: Re-image if not improving, or sooner if deficit worsens
Surgical referral: If any red flag or no improvement by 4-6 weeks
Surgery indicated: Persistent radiculopathy or any motor deficit at 6 weeks
Conservative continuation: Only if symptoms fully resolved
Return to sport: Gradual, only when pain-free and neurologically intact
Imaging: Repeat CT/MRI if any recurrence
Most published series report surgical treatment in 70-80 percent of cases. The bony fragment will not resorb; the indication for surgery is therefore often present at diagnosis. Conservative care is reasonable only for mild, non-deficit cases with small fragments. A patient with motor weakness or persistent radiculopathy at 4-6 weeks should be offered surgery - delay risks permanent deficit.
Complications
- Incidence
- 2-5 percent
- Risk Factors
- Adhesions from delayed surgery, large central fragment
- Management
- Primary repair with patch graft if needed
- Incidence
- 5-10 percent
- Risk Factors
- Incomplete disc clearance, early return to sport
- Management
- Revision decompression, consider fusion
- Incidence
- 5-15 percent
- Risk Factors
- Chronic compression, double-level lesion, incomplete decompression
- Management
- Re-image, consider revision if fragment missed
- Incidence
- Less than 2 percent
- Risk Factors
- Operative mishap, haematoma, retraction injury
- Management
- Urgent re-exploration if recognised early
- Incidence
- 1-3 percent
- Risk Factors
- Excessive facetectomy, pre-existing spondylolisthesis
- Management
- Fusion at same or staged procedure
- Incidence
- Less than 1 percent
- Risk Factors
- Contamination, haematoma
- Management
- Antibiotics, possible washout and biopsy
The two most common errors are: (1) operating without a CT and missing a sizeable bony fragment, and (2) removing only the disc and leaving the bone because the fragment was not visualised or not mobilised off the dura. Both result in persistent or recurrent radiculopathy. Pre-operative CT is mandatory; intra-operative identification of the fragment with fluoroscopy or radiograph before closure is recommended.
Outcomes and Prognosis
- Symptom Relief
- 85-95 percent good/excellent relief of radiculopathy
- Return to Sport
- 3-6 months post-op, near-universal return
- Long-term Sequelae
- Low recurrence (under 10 percent), preserved motion
- Symptom Relief
- 40-60 percent symptom resolution over 6-12 months
- Return to Sport
- Variable, often 6-12 months
- Long-term Sequelae
- Persistent canal compromise, risk of deficit
- Symptom Relief
- 85-90 percent relief, added morbidity of fusion
- Return to Sport
- 6-12 months (longer than decompression alone)
- Long-term Sequelae
- Adjacent segment disease, hardware-related issues
Best prognosis: Young athletic patient, Type II fragment, no delay, complete excision, dedicated rehabilitation
Poor prognosis: Delayed diagnosis over 6 months, pre-existing motor deficit (especially foot drop), cauda equina syndrome, multilevel disease
Key threshold: 6 weeks - outcomes decline significantly after 6 weeks of conservative care if there is motor deficit.
Guidelines, Registries & Global Practice
- Posterior apophyseal ring fractures are uncommon but well-recognised across all regions, with most published series from North America, Europe, and East Asia
- Peak incidence is age 14-16 in athletic adolescents, with male predominance in contact and throwing sports
- Lower lumbar spine (L4-S1) is the predominant location in over 70 percent of cases
- Mechanism is forced flexion with axial load - football, gymnastics, weightlifting, wrestling, rugby
- High-resource settings: MRI + thin-slice CT routinely; microsurgical or tubular decompression with fragment and disc excision
- Limited-resource settings: MRI or CT alone (not both); open laminotomy with standard instruments; outcomes reported as comparable in small series
- Sport-specific guidance: Some national sporting bodies mandate CT before return to contact sport in adolescents with prior apophyseal injury
- Surgical threshold: Decreases in regions with specialist paediatric spine centres (lower threshold for early decompression)
- Diagnosis emphasis
- CT for bony fragment; MRI for neural element; both recommended in adolescents
- Acute treatment
- Decompression with fragment + disc excision for symptomatic cases
- Long-term guidance
- Fusion reserved for instability or recurrence
- Diagnosis emphasis
- Cross-sectional imaging (MRI + CT) for any adolescent radiculopathy lasting over 4-6 weeks
- Acute treatment
- Microdiscectomy / fragment excision via interlaminar approach
- Long-term guidance
- Return to sport at 3-6 months after symptom resolution
- Diagnosis emphasis
- CT is the imaging of choice; MRI adjunct for disc and neural element
- Acute treatment
- Interlaminar decompression with fragment and disc removal
- Long-term guidance
- Fusion rarely indicated; outcome data support decompression alone
- Diagnosis emphasis
- Thin-slice CT for fragment characterisation; MRI for soft tissue
- Acute treatment
- Laminotomy with fragment excision; fusion only for instability
- Long-term guidance
- Encourage early decompression within 6 weeks for motor deficit
There is no dedicated national registry for posterior apophyseal ring fractures; the evidence base consists of case series and operative-technique reviews. Reported series are typically 10-50 patients with 2-5 year follow-up, and consistently support decompression alone (no fusion) for the typical lesion. The Takata classification (1988) and Dake CT criteria (1985) remain the diagnostic and treatment cornerstones. Health-economic arguments increasingly favour early MRI + CT to avoid prolonged conservative care that ultimately fails in 70-80 percent of cases.
Record in every adolescent with radiculopathy:
- Age, sport, mechanism of injury
- Neurologic examination findings (motor, sensory, reflexes, perianal tone)
- Imaging obtained (MRI, CT, or both) and the location and size of the fragment
- Indication for surgery (radiculopathy duration, motor deficit, fragment size)
- Operative findings (Takata type, fragment size, disc material excised)
- Post-op plan (mobilisation, return-to-sport timeline)
- Follow-up plan (clinical review at 6 weeks, 3 months, 6 months)
A missed or delayed diagnosis leading to permanent neurological deficit is a recurring source of complaint in this age group. Always perform and document a complete neurologic examination including perianal tone in any adolescent with persistent radicular pain.
Controversies & Areas of Uncertainty
Small non-randomised series suggest carefully selected patients with small fragments, mild symptoms, and no deficit can be managed conservatively. However, the bony fragment will not resorb, and the majority of patients (70-80 percent) ultimately come to surgery. There is no high-quality RCT; threshold for surgery is therefore pragmatic and surgeon-dependent.
The standard is decompression alone, even for large Type III fragments. Fusion is reserved for documented instability (iatrogenic, pre-existing spondylolisthesis) or recurrence. Small series show no benefit of routine fusion at the index procedure, with the added morbidity of hardware and adjacent segment risk.
Most published series advise 3-6 months before return to contact or high-load sport. There is no high-quality evidence defining the minimum safe interval, and many surgeons individualise the decision based on neurologic recovery, residual imaging findings, and the demands of the sport.
MRI alone can miss the bony component; CT alone can miss the disc and root compression. There is consensus that both are ideal, but in resource-limited settings either alone may be acceptable. Where both are available, both should be obtained before surgical planning.
MCQ Practice Points
Q: What is the posterior ring apophysis, and why is it relevant to adolescent spinal pathology? A: The posterior ring apophysis is a secondary ossification centre at the posterior vertebral body rim. It appears at age 6-8 and fuses with the vertebral body by age 18-25 (one of the last skeletal fusion events in the body). While unfused, it is a cartilaginous synchondrosis and the mechanical weak point of the motion segment. Under flexion with axial load, the disc material levering against the posterior corner can avulse this apophysis into the spinal canal, producing a posterior apophyseal ring fracture.
Q: An athletic 15-year-old presents with radiculopathy. MRI shows a disc extrusion with a low-signal focus adjacent to it. What is the most likely diagnosis and what is the next imaging step? A: The most likely diagnosis is a posterior apophyseal ring fracture. The 'low-signal focus' on MRI represents the avulsed bony fragment. The next imaging step is a thin-slice CT scan of the lumbar spine, which is the gold standard for confirming and characterising the bony fragment. The CT defines the fragment size, location, and relationship to the neural elements, and is essential for surgical planning.
Q: Why is CT scan superior to MRI for diagnosing posterior apophyseal ring fractures? A: CT directly visualises bone and shows the displaced posterior bony fragment, its size, shape, and relationship to the spinal canal. MRI shows the disc and neural element compression well, but underestimates the calcified or ossified component of the fragment. Plain radiographs miss the fragment in over 80 percent of cases. For surgical planning, CT is the primary imaging modality, with MRI as the adjunct.
Q: What is the surgical treatment of a posterior apophyseal ring fracture at L4-L5 in a 15-year-old with persistent radiculopathy and EHL weakness? A: Decompression via interlaminar approach with excision of the bony fragment and the associated disc material. Steps: (1) prone position, fluoroscopic level confirmation; (2) subperiosteal exposure and limited laminotomy on the affected side; (3) identify the fragment between the thecal sac and the vertebral body; (4) develop a plane between fragment and dura using a fine curette; (5) excise the fragment with a pituitary rongeur or fine osteotome; (6) clear the disc space of any loose disc material; (7) confirm a free nerve root. Fusion is not required in the typical case. Post-op: mobilise day 1, return to sport 3-6 months.
Q: When is conservative care appropriate for a posterior apophyseal ring fracture? A: Conservative care is appropriate only in selected mild cases: small Type I or small Type II fragments, no motor deficit, and tolerable pain. Bone does not resorb spontaneously, so most cases (70-80 percent) ultimately require surgery. Indications for surgery include: persistent radiculopathy beyond 4-6 weeks, motor weakness, cauda equina syndrome, or a sizeable fragment on CT. Delay beyond 6 weeks in a patient with motor deficit is associated with worse outcomes.
Q: Describe the Takata classification of posterior apophyseal ring fractures. A: Type I: Avulsion of the central cartilaginous node, no cortical bone (least common, often Schmorl-node variant). Type II: Avulsion of the posterior rim fragment, containing cortical and cancellous bone with overlying cartilage (most common). Type III: Large osseous fragment, including a substantial portion of the posterior vertebral body corner (requires wider surgical exposure).
Clinical Imaging
Every adolescent with radiculopathy or sciatica must be imaged with both MRI (to assess disc and neural elements) AND CT (to characterise the bony fragment and its location within the canal). Plain radiographs miss the fragment in most cases; MRI alone may underestimate the bony size. CT is diagnostic and surgical planning.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 15-year-old competitive football player presents with a 6-week history of left leg pain and paraesthesia in the L5 dermatome following a hyperextension tackle. He has a positive straight leg raise at 30 degrees on the left, weakness of extensor hallucis longus (4/5), and reduced sensation over the dorsum of the foot. X-rays are reported as normal. MRI shows a large left paracentral disc extrusion at L4-L5 with what is described as a 'small low-signal focus' adjacent to it. What is the most likely diagnosis and what is your next step?”
“A 14-year-old gymnast presents to the emergency department with a 36-hour history of bilateral leg pain, urinary retention (requiring catheterisation), saddle anaesthesia, and reduced perianal tone. She had been complaining of back pain for several weeks but had not sought medical attention. MRI shows a large central posterior mass at L5-S1 compressing the thecal sac. CT confirms a large bony fragment with disc material. How would you manage this?”
Key Anatomy
- Posterior ring apophysis = secondary ossification centre at posterior vertebral body rim
- Fuses at age 18-25 (last spinal fusion in body), weakest point when unfused
- Avulsed fragment contains bone + cartilage + disc material (NOT just disc)
- Most common at L4-S1 in athletic adolescents (age 13-18, male predominance)
Diagnosis
- Adolescent athlete with radiculopathy after flexion/axial load injury
- Motor weakness in 30-50 percent; positive SLR, dermatomal sensory loss
- CT scan is the gold standard imaging - shows displaced bony fragment
- MRI is the adjunct - shows disc and neural element compression
- Plain radiographs miss the fragment in over 80 percent of cases
Takata Classification
- Type I - central cartilaginous node separation (no bone, uncommon)
- Type II - posterior rim fragment with cortical and cancellous bone (most common)
- Type III - large osseous fragment from vertebral body corner (wider exposure)
- All three types require surgical excision of fragment AND disc material
Treatment Algorithm
- Conservative care - selected mild cases, no deficit, small fragment (minority)
- Surgery - persistent radiculopathy over 4-6 weeks, motor deficit, or sizeable fragment
- Decompression alone (laminotomy) with fragment and disc excision - standard
- Fusion reserved for instability, recurrence, or pre-existing spondylolisthesis
- Cauda equina syndrome = emergency decompression within 24-48 hours
Surgical Pearls
- Interlaminar approach on the side of the fragment; bilateral for central
- Develop a plane between fragment and dura with a fine curette - never lever against dura
- Excise BOTH the bone and the disc material - missing the disc risks recurrence
- Confirm a free nerve root that moves 1 cm on palpation before closure
- Use intraoperative fluoroscopy to confirm level and check for residual fragment
Complications
- Dural tear (2-5 percent) - repair primarily, patch if needed
- Recurrent herniation (5-10 percent) - incomplete disc clearance, early sport return
- Persistent radiculopathy (5-15 percent) - missed fragment, chronic compression
- Iatrogenic instability (1-3 percent) - excessive facetectomy, warrants fusion
- Worsening deficit (under 2 percent) - haematoma, retraction injury, urgent re-exploration
Prognosis
- Decompression alone: 85-95 percent good/excellent radicular relief
- Return to sport: 3-6 months in most cases
- Recurrence: under 10 percent with complete fragment and disc excision
- Best prognosis: young athletic patient, Type II fragment, no delay, complete excision
- Poor prognosis: motor deficit over 6 weeks, cauda equina, multilevel disease
Evidence Base and Key Trials
Fracture of the posterior margin of a lumbar vertebral body in children and adolescents. A report of seven cases
- Original description of posterior apophyseal ring fracture in seven adolescents with mean age 14 years
- Introduces the three-type classification (central cartilaginous separation, posterior rim avulsion, large corner fragment) still used today
- All seven cases involved lower lumbar spine (L4-S1) and presented with radiculopathy following sport
- Surgical excision of the fragment produced complete relief in all cases
Computed tomography of posterior lumbar apophyseal ring fractures
- First series to define CT appearance of posterior apophyseal ring fractures in adolescents
- CT reliably shows the displaced bony fragment, its size, and its relationship to the canal and neural elements
- Plain radiographs and tomograms consistently underestimate or miss the fragment
- Authors argue that CT should be the imaging of choice when this diagnosis is suspected
Association of vertebral end plate fracture with pediatric lumbar intervertebral disk herniation: value of CT and MR imaging
- Correlates CT and MRI findings with surgical confirmation in pediatric disc herniations with end plate / apophyseal avulsion
- CT best for the bony component; MRI best for the disc and neural element compression
- Combined CT + MRI protocol changes surgical plan in a substantial proportion of pediatric cases
- Apophyseal ring avulsion present in a significant minority of pediatric 'disc herniations' when both modalities are used
Posterior lumbar apophyseal fractures
- Larger surgical series of posterior apophyseal fractures across pediatric and young adult patients
- Confirms that simple fragment excision (decompression alone) is sufficient in the majority of cases, with no need for fusion
- Recurrence rate is low (under 10 percent) when the fragment and the associated disc material are excised
- Long-term follow-up shows preserved motion and good functional outcome in the majority of patients