Spinal Cord Monitoring (Intraoperative Neuromonitoring)
- Relying on SSEP alone. SSEP watches the posterior columns and can MISS an isolated anterior-cord / motor injury — the classic "normal SSEP, woke up paraplegic" false-negative. Use MEP too.
- Forgetting the alarm criteria. SSEP alarm = roughly a 50% amplitude drop or 10% latency rise — know the numbers.
- Incompatible anaesthesia. Volatile agents and muscle relaxants abolish MEP/EMG — you need TIVA, no long-acting paralytic, or you will misread a drug effect as an injury.
- Not raising the blood pressure first. On a signal change the first physiological move is to raise the MAP (cord perfusion) and correct anaemia/hypothermia — before assuming a surgical cause.
- Continuing the correction. A genuine, persistent change is an emergency — release the correction/distraction and remove recent implants, do not push on.
- Misreading triggered EMG. A LOW stimulation threshold on a pedicle screw means a medial breach (screw near the root) — not a high one.
Overview: why monitor & the tracts at stake
The purpose of IONM is a real-time warning of an evolving neurological injury — from distraction/correction, direct trauma, implant malposition or ischaemia — so it can be reversed before it becomes permanent. Different modalities watch different tracts, and the spinal-cord cross-section is the key: the posterior (dorsal) columns carry sensation (monitored by SSEP), while the corticospinal tracts carry motor output (monitored by MEP). Because these lie in different parts of the cord with different blood supplies, no single modality is sufficient.
Monitors the dorsal (posterior) columns (sensory). Robust and continuous, but can MISS an isolated anterior-cord/motor injury (the cord's blood supply and the corticospinal tracts are anterior) — historically the cause of the false-negative "normal SSEP but woke up paraplegic".
Monitors the corticospinal (motor) tracts / anterior cord — the function that matters most and the territory at risk in anterior spinal artery injury. More immediate, but sensitive to volatile anaesthetics and paralysis. Combine with SSEP for complete coverage.
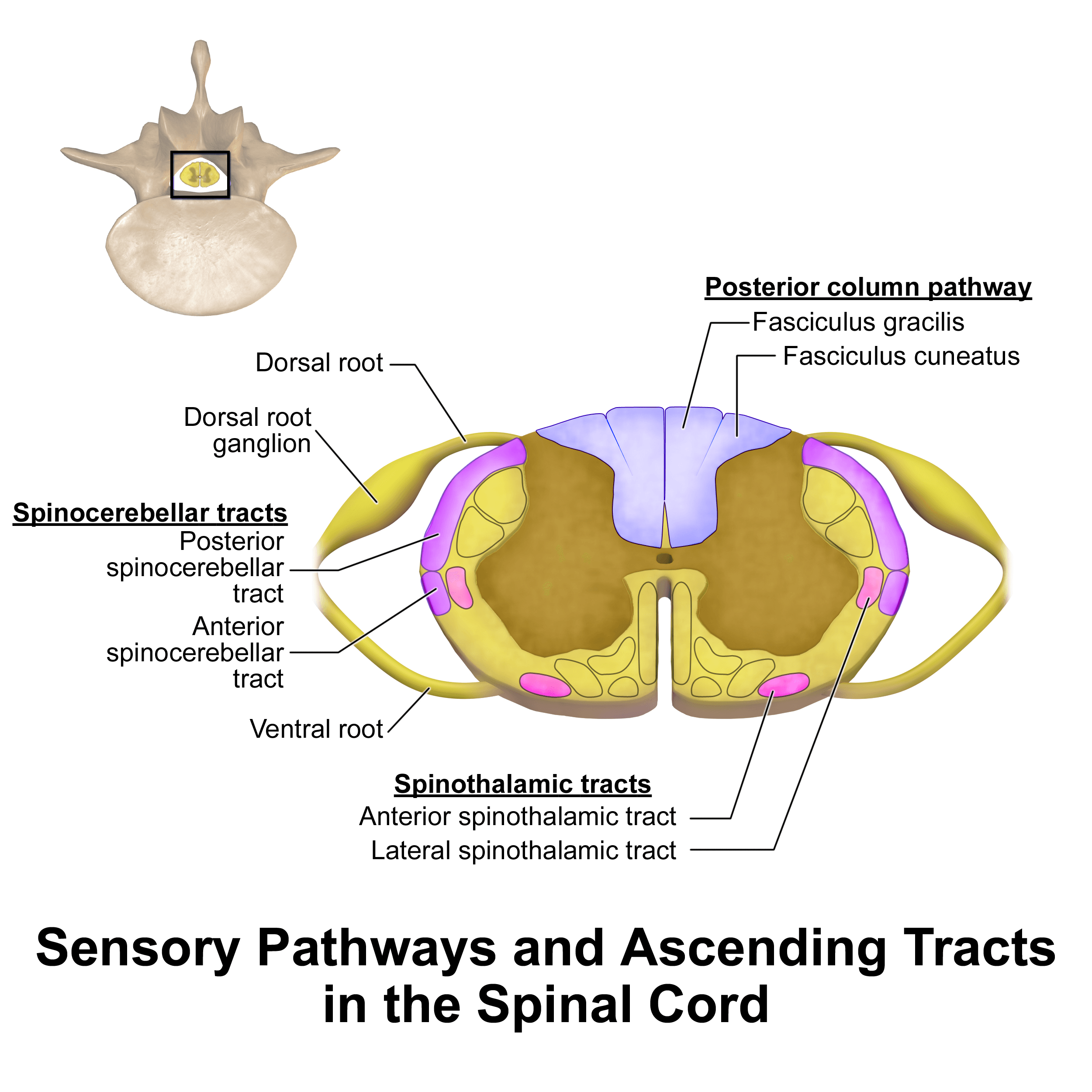
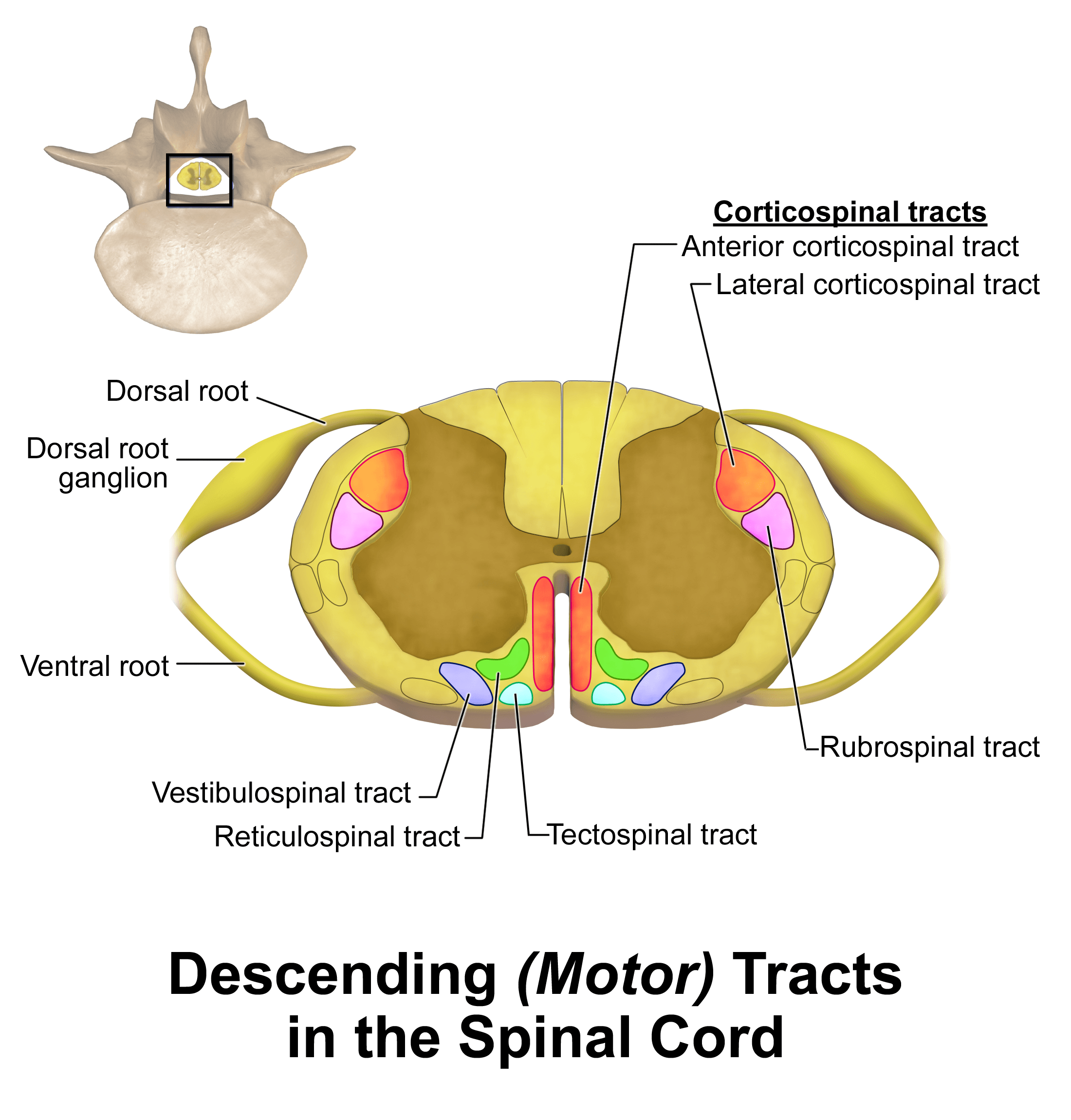
- A single anterior spinal artery supplies the anterior two-thirds of the cord — the corticospinal (motor) tracts, the spinothalamic (pain/temperature) tracts and the anterior horns.
- Paired (two) posterior spinal arteries supply the posterior third — the dorsal columns (proprioception/vibration).
- The dominant thoracolumbar feeder is the artery of Adamkiewicz (arteria radicularis magna), usually arising on the left between about T9 and T12 and supplying the lumbar enlargement; the mid-thoracic cord (~T4–T9) is a poorly-perfused watershed.
- Why it matters for IONM: an anterior-cord ischaemic insult (correction/distraction stretching the feeders, or anterior-spinal-artery compromise) knocks out MOTOR (MEP) while sparing the dorsal columns (SSEP stays normal) — the exact "normal SSEP, lost MEP" pattern MEP was added to catch — and it is why raising the MAP to perfuse the anterior cord is the first response.
- Anterior cord syndrome: bilateral loss of motor and pain/temperature below the level with preserved proprioception/vibration/light touch — the worst-prognosis incomplete cord syndrome.
Concepts: the monitoring modalities
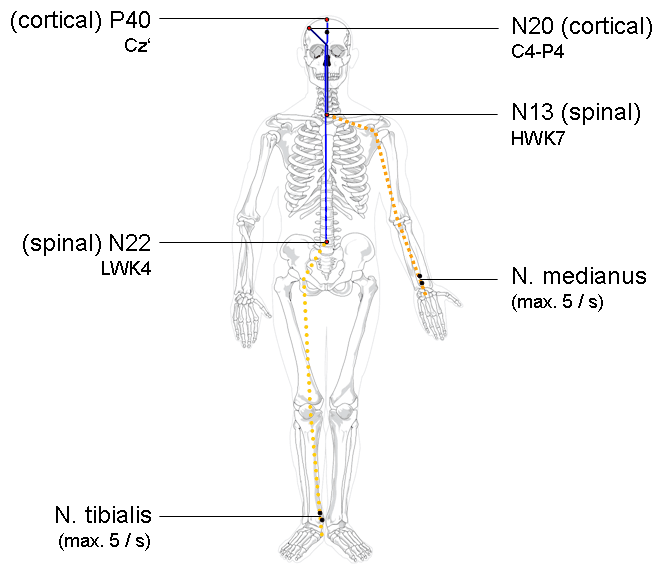
Somatosensory evoked potentials stimulate a peripheral nerve (e.g. posterior tibial, ulnar) and record the response at the cortex/scalp (and sometimes spinal/peripheral). They monitor the dorsal-column–medial-lemniscus (sensory) pathway. Standard alarm criteria are about a 50% decrease in amplitude or a 10% increase in latency. SSEP is robust and relatively anaesthesia-tolerant, but signals are averaged (slightly delayed) and it does not monitor the motor tracts, so it can miss an anterior-cord injury.
- Monitors
- Posterior columns (sensory)
- Alarm / signal
- ~50% amplitude drop or ~10% latency increase
- Key caveat
- Misses isolated motor/anterior-cord injury; averaged (delayed)
- Monitors
- Corticospinal (motor) / anterior cord
- Alarm / signal
- Significant amplitude loss / threshold rise
- Key caveat
- Very sensitive to volatile agents & paralysis (need TIVA, no relaxant)
- Monitors
- Nerve-root irritation
- Alarm / signal
- Bursts / neurotonic discharges
- Key caveat
- Non-specific; needs no muscle relaxant
- Monitors
- Pedicle screw position
- Alarm / signal
- LOW stimulation threshold = medial breach
- Key caveat
- Threshold cut-offs vary; needs no relaxant
- Monitors
- Gross voluntary motor function
- Alarm / signal
- Patient cannot move feet on command
- Key caveat
- Single time point; interrupts surgery; risks (recall, extubation, embolism)
Transcranial MEP is powerful but not free of hazards — examinable safety points the topic should state:
- Relative contraindications: epilepsy/seizure disorder, cortical lesions or skull defects near the stimulating electrodes, implanted intracranial electrodes/vascular clips/shunts, a cardiac pacemaker or implantable defibrillator, and cochlear/other electronic implants.
- Complications: the commonest is a tongue or lip laceration (and dental/jaw injury) from the masseter/temporalis contraction the stimulus evokes — so a soft bite block is mandatory; the limb twitch can interrupt surgery at the critical moment; and rarely seizures, cardiac arrhythmias or scalp burns at the electrode sites.
- Limitations: MEP is unreliable in young children (the corticospinal tract is not fully myelinated in the first few years) and a baseline is hard to obtain in a pre-existing motor deficit / established myelopathy — so confirm a reliable baseline at the start before trusting later changes.
Clinical relevance: anaesthesia & the response to a signal change
For MEP (and EMG) to work, the anaesthetic must preserve neuromuscular transmission and cortical excitability: use total intravenous anaesthesia (TIVA), avoid or minimise volatile (inhalational) agents (which suppress MEP), and avoid long-acting muscle relaxants once motor monitoring is running. Maintain stable physiology — adequate mean arterial pressure, normothermia and haemoglobin — because hypotension, hypothermia and anaemia themselves reduce signals and threaten cord perfusion.
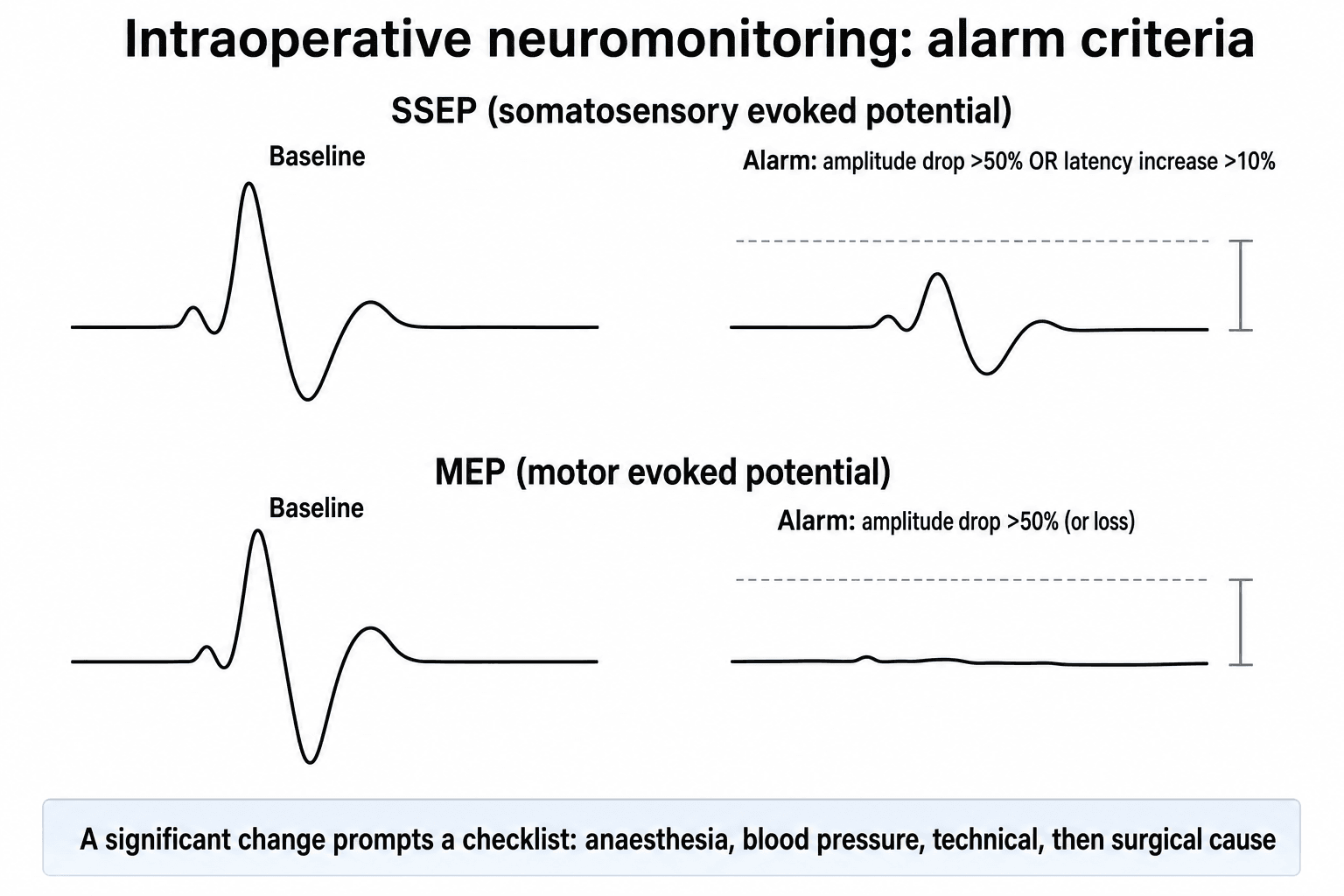
- 1Confirm it is realCheck for technical/equipment causes and verify with the neurophysiologist; note whether it is SSEP, MEP, EMG or all — and whether unilateral or bilateral.
- 2Anaesthetic & physiologicalRaise the mean arterial pressure (improve cord perfusion); correct hypotension, anaemia, hypothermia and hypocapnia; confirm the patient is not inadvertently paralysed or too deeply anaesthetised.
- 3SurgicalRelease/reduce the correction or distraction, remove recently placed instrumentation or grafts, decompress and inspect the cord, then reassess the signals.
- 4Confirm & treatConsider a Stagnara wake-up test; if a true deficit persists, maintain a high MAP, consider steroids per local protocol, and plan imaging/management. Act quickly — the goal is to reverse before it becomes permanent.
Mnemonics & memory aids
SAMEWhat each modality monitors
Hook:SAME: SSEP sensory, Anterior cord = MEP, Multimodal, EMG for roots/screws.
TIVAMonitoring-friendly anaesthesia
Hook:TIVA keeps the signals alive: total IV anaesthesia, no volatile, no paralytic, good perfusion.
ALARMResponding to an alarm
Hook:On an ALARM: confirm + anaesthesia, lift the BP, fix anaemia/temp, release the correction, then wake-up test.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“During scoliosis correction, what neuromonitoring modalities would you use, what does each monitor, and why is multimodal monitoring preferred?”
“Midway through the correction the MEPs are lost. What anaesthetic conditions are required for monitoring, and how do you respond to this signal change?”
Exam cheat sheet
Modalities & what they monitor
- SSEP = posterior columns (sensory); alarm ~50% amplitude drop or ~10% latency rise
- MEP = corticospinal (motor)/anterior cord; immediate; anaesthesia-sensitive
- EMG: free-run (root irritation) + triggered (low threshold = medial pedicle-screw breach)
Why multimodal
- SSEP misses motor/anterior-cord injury; MEP misses sensory
- Multimodal (SSEP + MEP ± EMG) is now standard
- Risk factors for signal change: preop deficit, severe kyphosis, large curve, cord shortening (VCR)
Anaesthesia
- TIVA; avoid/minimise volatile agents (suppress MEP)
- No long-acting muscle relaxant once MEP/EMG running
- Maintain MAP, normothermia, Hb (perfusion)
Response to a signal change
- Confirm real (technical/neurophysiologist); check anaesthesia/paralysis
- Raise MAP; correct hypotension/anaemia/hypothermia
- Release correction/distraction, remove recent instrumentation; Stagnara wake-up test; treat if true deficit
Evidence Base
The use of IONM in scoliosis/deformity surgery has risen steadily, and multimodal monitoring (e.g. combined SSEP + EMG, increasingly with MEP) is used more often than single-modality monitoring, because the modalities are complementary. Risk factors for intraoperative signal changes include a pre-operative neurological deficit, severe kyphosis, a large curve magnitude, and significant cord shortening (e.g. during vertebral column resection). Definitive randomised proof that monitoring reduces deficits is hard to obtain (the highest-risk cases are the ones monitored), but multimodal IONM allows potential injuries to be localised and managed in real time and is considered a valuable safety tool in deformity surgery.
Somatosensory evoked potential spinal cord monitoring reduces neurologic deficits after scoliosis surgery: results of a large multicenter survey
- Landmark Scoliosis Research Society multicentre survey of SSEP spinal-cord monitoring during scoliosis surgery.
- Experienced SSEP monitoring teams had FEWER THAN HALF as many neurologic deficits per 100 cases as inexperienced teams; false-negative monitoring (a definite deficit despite stable SSEPs) occurred in only 0.063% of patients.
- Surgeon experience and use of the wake-up test were also independently associated with fewer deficits.
Neuromonitoring in spinal deformity surgery: a multimodality approach
- Multimodal intraoperative monitoring (SSEP, MEP, EMG) localises and manages potential neurologic injuries in real time and is a valuable tool for the safety of spinal deformity surgery.
- Risk factors for intraoperative signal changes include preoperative neurologic deficit, severe kyphosis, increased curve magnitude and significant cord shortening (e.g. vertebral column resection).
- Although no evidence-based treatment algorithm exists for signal changes, structured strategies help prevent and address neurologic alarms.
Demographic trends in the use of intraoperative neuromonitoring for scoliosis surgery in the United States
- Use of intraoperative neuromonitoring for scoliosis surgery rose from 27% (2005) to 46.9% (2011); multimodal monitoring was used more commonly than unimodal (64.6% vs 35.4%).
- The most commonly used combination was SSEP + EMG, and the least used was MEP alone.
- Observed neurological-injury rates were similar with and without monitoring (1.8% vs 2.0%), but the authors caution this likely reflects that higher-risk surgeries preferentially use monitoring.
The foundational efficacy data (experienced SSEP teams under half the deficit rate; false-negatives only 0.063%) come from the SRS multicentre survey, Nuwer et al. 1995 (DOI); the multimodal approach, risk factors for signal changes and the real-time-management rationale from Laratta et al. 2017 (DOI); and the usage trends/modality data from Ajiboye et al. 2018 (DOI). The specific SSEP alarm criteria (50% amplitude / 10% latency), the SSEP-vs-MEP tract distinction, triggered-EMG pedicle-screw testing, the TIVA/no-relaxant requirement and the Stagnara wake-up test are standard, well-established neuromonitoring teaching.