Treatment of Spinal Stenosis | Neurogenic Claudication | With/Without Fusion Decision
STENOSIS TYPES
Critical Must-Knows
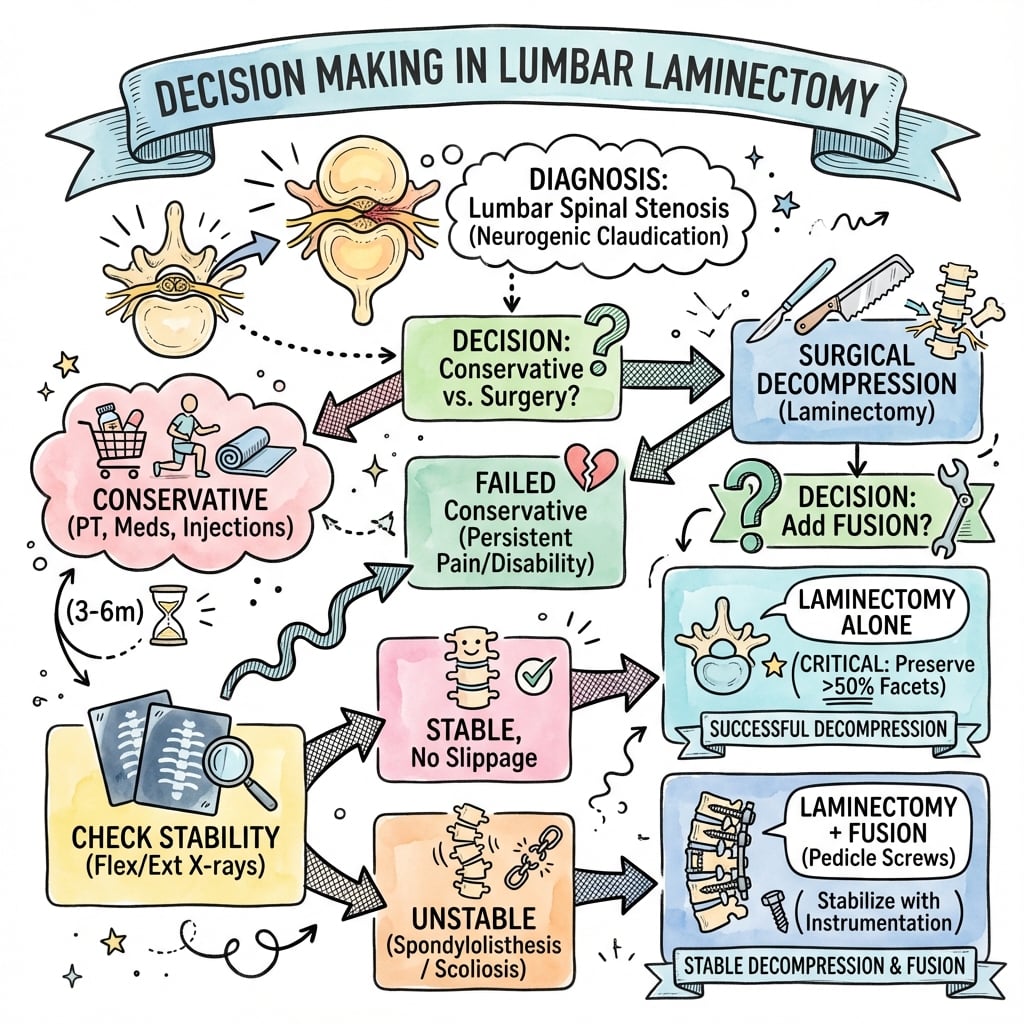
- Neurogenic claudication = bilateral leg symptoms with walking, relief with flexion/sitting
- Shopping cart sign = flexion reduces symptoms by increasing canal diameter
- Laminectomy vs fusion - add fusion if instability, deformity, or extensive facet resection
- Preserve more than 50% of facets to maintain stability without fusion
- SPORT showed surgery superior to conservative at 2-4 years for stenosis
Clinical Pearls
- "Neurogenic vs vascular claudication: flexion relief vs position-independent
- "Preserve facets (more than 50%) to avoid post-laminectomy instability
- "Fusion indications: spondylolisthesis, scoliosis, more than 50% facet removal
- "SPORT: Surgery better than conservative for stenosis
Clinical Imaging
Imaging Gallery




Critical Laminectomy Exam Points
Neurogenic vs Vascular Claudication
Neurogenic: Relieved by flexion (shopping cart), bilateral, paresthesias. Vascular: Relieved by rest alone, cramping, absent pulses. This distinction is an exam favorite!
Fusion Decision
Add fusion if: Pre-existing spondylolisthesis, significant scoliosis, more than 50% bilateral facetectomy needed, dynamic instability on flexion-extension. Laminectomy alone destabilizes if too much facet removed.
Preserve Facet Joints
More than 50% facet preservation required to maintain stability after laminectomy. Extensive medial facetectomy without fusion leads to progressive instability and recurrent stenosis.
SPORT Trial Results
Stenosis: Surgery superior to conservative at 2-4 years. Unlike disc herniation (similar outcomes), stenosis patients do better with surgical decompression.
At a Glance
Lumbar Laminectomy - Quick Reference
| Feature | Details |
|---|---|
| Definition | Removal of lamina and ligamentum flavum to decompress spinal canal |
| Primary indication | Lumbar spinal stenosis with neurogenic claudication |
| Most common level | L4-5 (most commonly stenotic level) |
| Success rate | 70-80% improvement in claudication |
| Key distinction | Neurogenic (flexion relief) vs vascular (rest relief) claudication |
| Fusion decision | Add if spondylolisthesis, scoliosis, or more than 50% facet removal |
| Dural tear rate | 3-5% (higher in revision, elderly, severe stenosis) |
| Hospital stay | 1-3 days for laminectomy alone, longer if fusion |
| SPORT findings | Surgery superior to conservative at 2-4 years for stenosis |
STENOS - ISTENOS - Indications for Laminectomy
| S | Stenosis confirmed on imaging MRI shows canal narrowing |
| T | Tried conservative treatment Failed 3-6 months non-operative |
| E | Examination correlates Clinical matches imaging level |
| N | Neurogenic claudication Bilateral leg symptoms with walking |
| O | Ongoing functional limitation Walking distance significantly impaired |
| S | Shopping cart sign positive Flexion relieves symptoms |
| S | Stenosis confirmed on imaging MRI shows canal narrowing | E | Examination correlates Clinical matches imaging level | O | Ongoing functional limitation Walking distance significantly impaired |
| T | Tried conservative treatment Failed 3-6 months non-operative | N | Neurogenic claudication Bilateral leg symptoms with walking | S | Shopping cart sign positive Flexion relieves symptoms |
Hook:STENOS is the indication for operating on STENOSIS
CLAUDICATE - NCLAUDICATE - Neurogenic vs Vascular
| C | Cramping = vascular Neurogenic more paresthesias |
| L | Legs (bilateral) = neurogenic Vascular often unilateral |
| A | Arterial pulses Check dorsalis pedis, posterior tibial |
| U | Uphill = vascular worse Neurogenic better (flexed posture) |
| D | Downhill = neurogenic worse Extension increases stenosis |
| I | Imaging needed MRI for stenosis, ABI for vascular |
| C | Cart (shopping) = neurogenic Leaning forward relieves symptoms |
| A | At rest relief = vascular Neurogenic needs to sit/flex |
| T | Time to relief Vascular: rest. Neurogenic: flex/sit |
| E | Exercise tolerance Fixed distance = vascular |
| C | Cramping = vascular Neurogenic more paresthesias | U | Uphill = vascular worse Neurogenic better (flexed posture) | C | Cart (shopping) = neurogenic Leaning forward relieves symptoms | E | Exercise tolerance Fixed distance = vascular |
| L | Legs (bilateral) = neurogenic Vascular often unilateral | D | Downhill = neurogenic worse Extension increases stenosis | A | At rest relief = vascular Neurogenic needs to sit/flex | ||
| A | Arterial pulses Check dorsalis pedis, posterior tibial | I | Imaging needed MRI for stenosis, ABI for vascular | T | Time to relief Vascular: rest. Neurogenic: flex/sit |
Hook:Know how to CLAUDICATE between neurogenic and vascular causes
FUSE - WFUSE - When to Add Fusion
| F | Fifty percent facet removal More than 50% facetectomy destabilizes |
| U | Unstable (spondylolisthesis) Pre-existing or dynamic instability |
| S | Scoliosis (degenerative) Curve may progress after decompression |
| E | Extensive decompression Multi-level with facet compromise |
| F | Fifty percent facet removal More than 50% facetectomy destabilizes | S | Scoliosis (degenerative) Curve may progress after decompression |
| U | Unstable (spondylolisthesis) Pre-existing or dynamic instability | E | Extensive decompression Multi-level with facet compromise |
Hook:FUSE when stability is at risk - don't just decompress
SPORT - TSPORT - Trial Key Points
| S | Stenosis responds to surgery Surgery superior at 2-4 years |
| P | Prospective randomized Landmark spine surgery trial |
| O | Outcomes favor surgery Unlike disc (similar), stenosis better with surgery |
| R | Research supports decompression Level I evidence |
| T | Two to four year benefit Durability of surgical result |
| S | Stenosis responds to surgery Surgery superior at 2-4 years | R | Research supports decompression Level I evidence |
| P | Prospective randomized Landmark spine surgery trial | T | Two to four year benefit Durability of surgical result |
| O | Outcomes favor surgery Unlike disc (similar), stenosis better with surgery |
Hook:SPORT showed stenosis should be operated on
Overview
Lumbar laminectomy is the surgical removal of the lamina (posterior arch) and ligamentum flavum to decompress the spinal canal. It is the definitive treatment for symptomatic lumbar spinal stenosis unresponsive to conservative management. The procedure may be performed alone or in combination with fusion depending on stability considerations.
Historical Development
Laminectomy has been performed since the early 1900s. Modern techniques emphasize limited decompression preserving stabilizing structures. The transition from wide laminectomy to targeted decompression has improved outcomes and reduced post-laminectomy instability.
Epidemiology
Lumbar spinal stenosis is the most common indication for spine surgery in patients over 65 years. Prevalence increases with age due to degenerative changes. L4-5 is the most commonly affected level.
Clinical Pearl
The SPORT trial demonstrated that surgical treatment of lumbar spinal stenosis produces superior outcomes compared to conservative treatment at 2-4 years. This contrasts with disc herniation, where long-term outcomes are similar between surgical and conservative approaches.
Pathophysiology and Mechanisms
Anatomy of Stenosis
Structures Contributing to Central Stenosis:
- Ligamentum flavum hypertrophy (most significant)
- Facet joint hypertrophy
- Disc bulging
- Spondylolisthesis (if present)
Zones of Compression:
- Central canal: Cauda equina compression
- Lateral recess: Traversing nerve root
- Foramen: Exiting nerve root
Pathophysiology of Neurogenic Claudication
Mechanism:
- Standing/walking extends spine, reducing canal diameter
- Venous congestion in confined space
- Neural ischemia with ambulation
- Flexion increases canal diameter, relieves symptoms
Why Flexion Helps (Shopping Cart Sign):
- Lumbar flexion opens posterior canal
- Reduces facet joint and ligamentum flavum bulging
- Increases central canal area by 10-20%
- Classic posture: leaning on shopping cart
Stability Considerations
Facet Joint Importance:
- Primary posterior stabilizers
- Resist extension and rotation
- More than 50% bilateral facetectomy = instability risk
Risk Factors for Post-Laminectomy Instability:
- Excessive facet resection
- Pre-existing spondylolisthesis
- Degenerative scoliosis
- Young, active patient
- Multi-level decompression
Facet Preservation Critical
Preserving more than 50% of the facet joints bilaterally is essential to maintain stability after laminectomy. Extensive facet removal without fusion leads to progressive instability, recurrent stenosis, and poor outcomes.
Classification Systems
Anatomical Classification of Stenosis
Stenosis by Location
| Type | Location | Root Affected | Surgical Target |
|---|---|---|---|
| Central | Spinal canal | Cauda equina (multiple) | Laminectomy, ligamentum flavum |
| Lateral Recess | Subarticular zone | Traversing root | Medial facetectomy, undercut |
| Foraminal | Neural foramen | Exiting root | Foraminotomy, may need fusion |
The anatomical classification guides the surgical approach based on where compression occurs.
Clinical Assessment
Distinguishing Neurogenic from Vascular Claudication
Neurogenic vs Vascular Claudication
| Feature | Neurogenic | Vascular |
|---|---|---|
| Distribution | Bilateral, buttock to legs | Calves, unilateral or bilateral |
| Character | Aching, paresthesias, weakness | Cramping, tightness |
| Onset | Variable walking distance | Fixed walking distance (claudication distance) |
| Relief | Flexion/sitting (shopping cart) | Standing rest (no need to sit) |
| Uphill walking | Better (flexed posture) | Worse (more work) |
| Downhill walking | Worse (extended posture) | Better |
| Bicycle tolerance | Good (flexed) | Limited (cardiovascular) |
| Pulses | Normal | Diminished or absent |
Physical Examination
Neurological Assessment:
- Often normal at rest
- Motor, sensory, reflex examination
- Wide-based gait may be present
- Positive Romberg (proprioceptive loss)
Provocative Tests:
- Walking test: Reproduce symptoms, note distance
- Extension test: May reproduce symptoms
- Flexion relief: Supports neurogenic cause
Vascular Assessment:
- Peripheral pulses
- Ankle-brachial index (ABI) if concern
- Skin changes (hair loss, trophic changes)
Patient Selection
Good Surgical Candidate
- Neurogenic claudication confirmed
- Imaging correlates with symptoms
- Failed 3-6 months conservative treatment
- Significant functional limitation
- No severe cardiopulmonary comorbidities
- Realistic expectations
Poor Surgical Candidate
- Vascular claudication (needs vascular surgery)
- Minimal functional limitation
- Severe medical comorbidities
- Predominant back pain without leg symptoms
- Imaging does not correlate
- Unrealistic expectations
Differential Diagnosis of Leg Pain on Walking
Differential Diagnosis - Exertional Leg Symptoms
| Condition | Distinguishing Features | Key Investigation |
|---|---|---|
| Neurogenic claudication (stenosis) | Bilateral, flexion relief (shopping cart), normal pulses, variable distance | MRI lumbar spine |
| Vascular claudication (PAD) | Calf cramp, fixed distance, rest relief without flexion, absent pulses, trophic skin | Ankle-brachial index, duplex |
| Lumbar radiculopathy (disc) | Dermatomal, often unilateral, positive straight-leg raise, present at rest | MRI lumbar spine |
| Hip osteoarthritis | Groin/buttock pain, restricted internal rotation, worse weight-bearing | Pelvis/hip radiograph |
| Peripheral neuropathy | Stocking sensory loss, burning, distance-independent, often diabetic | Nerve conduction studies, HbA1c |
| Trochanteric/greater trochanteric pain | Lateral hip tenderness, pain on direct pressure, not position-dependent canal | Clinical, ultrasound |
Clinical Pearl
The shopping cart sign is pathognomonic for neurogenic claudication: patients lean on a shopping cart (flexed posture) and can walk further because flexion opens the spinal canal. Vascular claudication is relieved by simply stopping, without needing to flex. Always remember that vascular claudication and neurogenic claudication can coexist in the elderly, so check pulses and the ankle-brachial index even when stenosis is confirmed on MRI.
Investigations
Gold Standard for Stenosis Evaluation
Standard Protocol:
- Sagittal T1, T2
- Axial T2 at each level
- STIR for edema assessment
Key Findings:
- Central canal diameter (less than 10mm concerning)
- Ligamentum flavum thickness
- Facet hypertrophy
- Disc bulging contribution
- Lateral recess and foraminal stenosis
Correlation Important:
- Imaging findings common in asymptomatic elderly
- Clinical correlation mandatory
- Multi-level disease may need to identify worst level
MRI provides essential anatomic detail for surgical planning and helps identify the primary pathology.
Flexion-Extension Radiographs
Purpose: Assess dynamic instability
Instability Criteria:
- Translation more than 4mm
- Angulation more than 10-15° change
Clinical Significance:
- If unstable: Consider fusion with decompression
- Affects surgical planning significantly
Imaging Gallery
Surgical Technique and Outcomes

Management Algorithm
Conservative Management
First-Line Treatment (60-70% may improve):
- Activity modification
- NSAIDs, acetaminophen
- Physical therapy (flexion-based exercises)
- Epidural steroid injections
Conservative Trial Duration:
- 3-6 months typically
- May continue if symptoms manageable
- No evidence conservative prevents progression
Conservative management is the first-line approach for most patients with lumbar stenosis.
Surgical Technique
Preoperative Planning
Positioning: Prone on Wilson frame or Jackson table
- Abdomen free
- Hip flexed to flatten lordosis
- Eyes protected
Level Confirmation:
- Fluoroscopy mandatory
- Mark levels preoperatively
Approach and Exposure:
- Midline incision over affected levels
- Subperiosteal dissection to expose laminae
- Retract paraspinal muscles laterally
- Identify interlaminar spaces
- Confirm level with fluoroscopy
Decompression:
- Remove spinous process (optional, depends on technique)
- Use Kerrison rongeurs to remove lamina
- Remove hypertrophied ligamentum flavum
- Undercut medial facet for lateral recess
- Preserve more than 50% of facet joint
- Decompress to visualize normal dura proximally and distally
- Probe foramen for exiting root
The goal is adequate decompression while preserving as much stabilizing structure as possible.
Intraoperative Considerations
Dural Tear Prevention:
- Anticipate adherent dura in severe stenosis
- Careful technique with Kerrison
- Start at less stenotic area if possible
Hemostasis:
- Epidural veins can bleed significantly
- Bipolar cautery, hemostatic agents
- Avoid epidural hematoma
Nerve Root Protection:
- Identify and protect throughout
- Gentle retraction only
Complications
Intraoperative Complications
Intraoperative Complications
| Complication | Incidence | Prevention | Management |
|---|---|---|---|
| Dural tear | 3-5% | Careful technique, anticipate adhesions | Primary repair, sealant, bed rest |
| Nerve root injury | Less than 1% | Identify roots, gentle retraction | Observation, steroids |
| Wrong level | Rare | Fluoroscopic confirmation | Correct immediately, document |
| Bleeding | Variable | Meticulous hemostasis | Bipolar, hemostatic agents |
Postoperative Complications
Early:
- Wound infection (1-3%)
- Epidural hematoma (rare, emergency if symptomatic)
- CSF leak (if dural tear)
- Urinary retention
Late:
- Recurrent stenosis (regrowth of tissue)
- Post-laminectomy instability
- Adjacent segment disease
- Failed back surgery syndrome
Post-Laminectomy Instability
Risk Factors:
- Excessive facet removal (more than 50%)
- Pre-existing spondylolisthesis not fused
- Multi-level decompression
- Young, active patient
Presentation:
- Recurrent symptoms after initial improvement
- Progressive back pain and leg symptoms
- Imaging shows slip progression
Prevention:
- Limit facet resection
- Add fusion when risk factors present
- Preserve posterior tension band
Clinical Pearl
Post-laminectomy instability is preventable by preserving more than 50% of facet joints bilaterally and adding fusion when instability risk factors are present. Once it develops, salvage fusion is more complex.
Postoperative Care
Immediate Postoperative (Laminectomy Alone)
Day 0-1:
- Mobilize day of surgery or next day
- Neurological assessment
- Pain management
- DVT prophylaxis
Day 1-3:
- Increase ambulation
- Physiotherapy assessment
- Discharge when ambulatory, pain controlled
With Fusion - Modified Protocol
Differences:
- Longer hospital stay (2-5 days)
- Bracing may be required
- More restricted activity initially
- Fusion precautions for 3-6 months
Activity Guidelines
Recovery Timeline
| Activity | Laminectomy Alone | With Fusion |
|---|---|---|
| Hospital stay | 1-3 days | 2-5 days |
| Walking | Immediate | Immediate with precautions |
| Driving | 2-4 weeks | 4-6 weeks |
| Sedentary work | 2-4 weeks | 4-6 weeks |
| Physical work | 6-12 weeks | 3-6 months |
| Full activity | 3 months | 6-12 months |
Rehabilitation
Physical Therapy:
- Core strengthening (delayed 4-6 weeks)
- Flexibility exercises
- Aerobic conditioning
- Posture and body mechanics
Lifestyle:
- Weight optimization
- Smoking cessation (especially if fusion)
- Activity modification as needed
Outcomes and Prognosis
Success Rates
Laminectomy for Stenosis:
- Improvement in claudication: 70-80%
- Patient satisfaction: 70-80%
- Improvement in walking distance: Significant
- Back pain improvement: Variable (50-60%)
SPORT Trial Results
Key Findings for Stenosis:
- Surgical treatment superior to conservative
- Benefits seen at 2-4 years
- Walking capacity improved significantly
- This differs from disc herniation results
Durability of Results
Long-term Follow-up:
- Most maintain improvement 5-10 years
- Some recurrence due to regrowth
- Adjacent segment disease may develop
- Reoperation rate approximately 18% at 8 years in the SPORT surgical stenosis cohort, with recurrent stenosis and progressive spondylolisthesis the leading indications (Gerling et al., 2016)
Prognostic Factors
Favorable:
- Predominant leg symptoms
- Severe imaging stenosis correlating with symptoms
- Short symptom duration
- No major comorbidities
- Non-smoker
Unfavorable:
- Predominant back pain
- Mild imaging stenosis
- Long symptom duration
- Major comorbidities
- Obesity, smoking
- Psychiatric comorbidity
Evidence-Based Practice
SPORT Trial - Stenosis (Weinstein et al., 2008)
- Multicentre randomised and observational cohorts (n=289 randomised, 365 observational) of decompressive surgery vs usual non-operative care for stenosis WITHOUT spondylolisthesis
- Intention-to-treat analysis (randomised cohort): significant benefit favouring surgery on SF-36 bodily pain (mean difference 7.8, 95% CI 1.5 to 14.1), but not physical function or Oswestry at 2 years
- As-treated combined analysis: significant advantage for surgery across all primary outcomes from 3 months, maintained at 2 years
- Establishes surgery as more effective than non-operative care for symptomatic stenosis
- Defining Level I evidence underpinning surgical decompression for stenosis
SPORT Stenosis - 4-Year Outcomes (Weinstein et al., 2010)
- Four-year follow-up of the SPORT stenosis cohort (decompressive laminectomy vs non-operative care)
- As-treated analysis: clinically significant advantages for surgery maintained through 4 years
- Treatment effects - bodily pain 12.6 (95% CI 8.5-16.7), physical function 8.6 (95% CI 4.6-12.6), Oswestry -9.4 (95% CI -12.6 to -6.2)
- Secondary measures (bothersomeness, satisfaction, self-rated progress) also favoured surgery
- Demonstrates durability of surgical benefit over the medium term
Swedish Spinal Stenosis Study - Decompression +/- Fusion (Försth et al., 2016)
- 247 patients (50-80 years) with stenosis at 1-2 levels, randomised to decompression plus fusion vs decompression alone; stratified by presence of degenerative spondylolisthesis (135 patients)
- No significant difference in 2-year Oswestry (27 fusion vs 24 decompression-alone, P=0.24) or 6-minute walk (397 m vs 405 m, P=0.72)
- Results similar WITH and WITHOUT spondylolisthesis - fusion gave no clinical advantage in either subgroup
- Fusion increased hospital stay (7.4 vs 4.1 days), operating time, blood loss and cost
- Reoperation during mean 6.5-year follow-up similar (22% fusion vs 21% decompression-alone)
SLIP Trial - Laminectomy +/- Fusion for Grade I Spondylolisthesis (Ghogawala et al., 2016)
- 66 patients with stable Grade I degenerative spondylolisthesis (3-14 mm) and stenosis, randomised to laminectomy alone vs laminectomy plus instrumented posterolateral fusion
- Fusion gave a greater 2-year SF-36 physical-component gain (15.2 vs 9.5; difference 5.7, 95% CI 0.1-11.3, P=0.046), sustained at 3 and 4 years
- Oswestry change did not differ significantly at 2 years (-26.3 fusion vs -17.9 decompression-alone, P=0.06)
- Cumulative reoperation lower with fusion (14% vs 34%, P=0.05)
- Published alongside Försth - the two trials give discordant conclusions on fusion for spondylolisthesis
LESS Trial - Epidural Glucocorticoid for Stenosis (Friedly et al., 2014)
- Double-blind multisite RCT, 400 patients with central stenosis and moderate-to-severe leg pain, glucocorticoid plus lidocaine vs lidocaine alone
- No significant 6-week difference in Roland-Morris disability (adjusted -1.0, 95% CI -2.1 to 0.1, P=0.07)
- No significant difference in leg-pain intensity (adjusted -0.2, 95% CI -0.8 to 0.4, P=0.48)
- No benefit on prespecified interlaminar vs transforaminal subgroup analysis
- Adding the corticosteroid offered minimal or no short-term benefit over local anaesthetic alone
Schizas MRI Morphological Grading of Stenosis (Schizas et al., 2010)
- Derived a 7-grade (A1-D) qualitative classification of central stenosis from the dural sac rootlet/CSF morphology on axial T2 MRI
- Grades A-B retain visible CSF; grades C-D show no CSF around the rootlets
- Intra-observer agreement substantial (k=0.65), inter-observer moderate (k=0.44)
- Grade C-D patients were more likely to fail conservative treatment, supporting prognostic value
- Morphological grading identified different patients as stenotic than dural sac cross-sectional area alone
SPORT - Reoperation After Surgery for Stenosis (Gerling et al., 2016)
- Subanalysis of 417 surgically treated stenosis patients from SPORT (88% decompression only, 5% non-instrumented and 6% instrumented fusion)
- Reoperation rate 18% at 8 years; 52% of reoperations for recurrent stenosis or progressive spondylolisthesis
- Of those reoperated, 42% within 2 years, 70% within 4 years, 84% within 6 years
- Patients without a baseline neurological deficit were more likely to undergo reoperation (P=0.04)
- Patient-reported outcomes were worse in the reoperation group at 8 years
Special Considerations
Multi-Level Stenosis
Considerations:
- Longer operative time
- More blood loss
- Higher dural tear risk
- Greater instability potential
- May need fusion if extensive
Technique:
- Prioritize symptomatic levels
- Limited laminotomy vs full laminectomy
- Preserve facets at each level
Stenosis with Degenerative Spondylolisthesis
Classic Presentation:
- L4-5 most common level
- Female predominance
- Associated facet arthropathy
- Dynamic instability common
Treatment Decision:
- The SLIP trial (Ghogawala et al., 2016) showed adding instrumented fusion to laminectomy improved SF-36 physical health and roughly halved reoperation (14% vs 34%) in stable Grade I slips
- The Swedish Spinal Stenosis Study (Försth et al., 2016) found no advantage of fusion regardless of spondylolisthesis, with similar 2-year outcomes and reoperation
- These two Level I trials are discordant; the decision is individualised on slip stability, facet integrity and patient factors
- A mobile/unstable slip on flexion-extension imaging strengthens the case for fusion; a stable slip with preserved facets supports decompression alone
Stenosis with Degenerative Scoliosis
Considerations:
- Curve may progress after decompression
- Coronal and sagittal balance important
- Multi-level disease common
Treatment:
- May need fusion and possibly correction
- Decompression alone may worsen deformity
- Complex surgical planning
Elderly and Medically Complex Patients
Considerations:
- Higher perioperative risk
- Careful patient selection
- May accept limited improvement
- Conservative treatment remains option
Modifications:
- Limited decompression
- Avoid fusion if possible
- Optimize medical status preoperatively
Clinical Algorithm
Management Pathway
Step 1: Confirm Neurogenic Claudication
- Bilateral leg symptoms with walking
- Relief with flexion/sitting
- Rule out vascular claudication (ABI if needed)
Step 2: Imaging Correlation
- MRI confirms stenosis
- Correlate imaging level with symptoms
- Assess stability (flexion-extension views)
Step 3: Conservative Trial
- 3-6 months physical therapy, NSAIDs
- Consider epidural steroid injection
- Document functional limitation
Step 4: Surgical Decision
- If failed conservative: Proceed with surgery
- Assess need for fusion (spondylolisthesis, instability, scoliosis)
Step 5: Surgical Planning
- Laminectomy alone if stable, no spondylolisthesis
- Add fusion if instability or more than 50% facet removal needed
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Neurogenic Claudication with Shopping Cart Sign
"A 70-year-old woman presents with 2 years of bilateral leg pain and numbness when walking. She can walk 100 meters before needing to stop. She finds relief when pushing a shopping trolley. Peripheral pulses are normal. MRI shows L4-5 central stenosis. How would you manage her?"
Intraoperative Discovery of Spondylolisthesis
"During a planned L4-5 laminectomy for stenosis, you find the patient has degenerative spondylolisthesis that was not clearly appreciated on supine MRI. What do you do?"
Recurrent Symptoms Post-Laminectomy
"A 65-year-old man presents 2 years after L4-5 laminectomy with recurrent bilateral leg symptoms. He had excellent relief initially. What is your approach?"
Neurogenic vs Vascular Claudication Differentiation
"How do you distinguish neurogenic claudication from vascular claudication in a patient with leg pain on walking?"
MCQ Practice Points
Neurogenic vs Vascular Claudication
Q: What feature best distinguishes neurogenic from vascular claudication?
A: Relief with flexion (shopping cart sign). Neurogenic claudication is relieved by sitting or bending forward because flexion increases spinal canal diameter. Vascular claudication is relieved by rest in any position because the issue is cardiovascular, not spinal.
Indications for Fusion
Q: When should instrumented fusion be added to lumbar laminectomy for stenosis?
A: Fusion should be added in the presence of:
- Degenerative spondylolisthesis
- Pre-existing spinal instability (greater than 4mm translation on flexion-extension views)
- Removal of more than 50% of facet joints (iatrogenic instability)
- Significant degenerative scoliosis Laminectomy alone is appropriate for stable stenosis without spondylolisthesis.
SPORT Trial Evidence
Q: What did the SPORT trial show for lumbar spinal stenosis treatment?
A: The SPORT trial demonstrated that surgery was superior to conservative treatment at 2-4 years for symptomatic lumbar stenosis. Patients had significant improvement in walking capacity, pain, and function. Unlike disc herniation, the stenosis cohort showed sustained surgical benefit. Intent-to-treat analysis was limited by high crossover rate.
Most Common Level Affected
Q: What is the most commonly affected level in lumbar spinal stenosis?
A: L4-5 is the most commonly affected level (approximately 80% of cases), followed by L3-4. The L4-5 level is susceptible due to its high mobility and degenerative stress concentration.
Facet Preservation
Q: What percentage of facet joint should be preserved during laminectomy to maintain spinal stability?
A: More than 50% of the facet joint should be preserved. Removing more than 50% of the facet bilaterally risks iatrogenic instability and post-laminectomy spondylolisthesis, which may require subsequent fusion.
Guidelines, Registries & Global Practice
Global Epidemiology
Degenerative lumbar spinal stenosis is the leading indication for spinal surgery in adults over 65, and its prevalence rises steeply with age as the world's population ages. Decompression for stenosis is one of the highest-volume elective spinal procedures worldwide. Cross-country comparisons consistently show wide variation in rates of decompression and, in particular, in the proportion of decompressions accompanied by fusion - reflecting genuine clinical equipoise on the fusion question rather than differences in disease burden.
Guideline and Registry Comparison
Guidance and Registry Evidence Across Bodies
| Body / Source | Position on Decompression and Fusion | Evidence Basis |
|---|---|---|
| NASS (North American Spine Society) | Decompression recommended for symptomatic stenosis failing non-operative care; fusion reserved for instability/deformity, not routine for stenosis alone | Level I-II RCT evidence (SPORT, SLIP, Swedish study) |
| NICE (UK, NG59 low back pain & sciatica) | Consider decompression for stenosis when non-surgical care fails and symptoms warrant; does not endorse routine fusion for uncomplicated stenosis | Systematic review, Grade based |
| AAOS / spine collaboratives | Endorse decompression for refractory neurogenic claudication; individualised fusion decision based on stability | RCT and registry-informed |
| European (EFORT/Eurospine consensus) | Decompression first-line surgical option; fusion when documented instability or significant deformity | Consensus plus RCT evidence |
The two pivotal fusion trials published together in 2016 - the Swedish Spinal Stenosis Study (no fusion benefit) and the SLIP trial (fusion benefit in Grade I slip) - reached discordant conclusions, which is why guideline bodies converge on an individualised, stability-driven decision rather than a blanket recommendation. Registry data (for example large national spine registries in Sweden, Norway and the United Kingdom) broadly corroborate that decompression alone produces durable patient-reported improvement and that the addition of fusion increases cost, length of stay and morbidity without a consistent outcome advantage in stable stenosis.
Current Practice in Australia
Lumbar laminectomy is one of the most commonly performed spinal procedures in Australia, particularly in the ageing population, and is undertaken by both orthopaedic spine surgeons and neurosurgeons across public and private hospitals. Practice patterns align with international evidence, with emphasis on appropriate patient selection, an adequate trial of non-operative management, and an individualised approach to fusion based on stability assessment. Australian use of fusion-supplemented decompression mirrors the international debate, with most stable stenosis managed by decompression alone.
Documentation and Medicolegal Considerations
Key documentation requirements include confirmation of neurogenic versus vascular claudication, imaging correlation with symptoms, a documented trial of conservative treatment, explicit discussion of whether fusion is required, and informed consent for potential complications including dural tear. Standing (and where indicated flexion-extension) radiographs should form part of the preoperative workup, because spondylolisthesis and dynamic instability may not be apparent on supine MRI.
Lumbar Laminectomy Key Points
Clinical summary
Neurogenic vs Vascular Claudication
- •Neurogenic: flexion relieves (shopping cart sign)
- •Vascular: rest alone relieves
- •Neurogenic: better uphill, worse downhill
- •Vascular: worse uphill, better downhill
- •Check pulses, ABI if uncertain
Fusion Decision (FUSE)
- •Fifty percent facet removal (more than 50%)
- •Unstable (spondylolisthesis, dynamic instability)
- •Scoliosis (degenerative)
- •Extensive multi-level decompression
SPORT Trial - Stenosis
- •Surgery SUPERIOR to conservative (unlike disc)
- •Benefits at 2-4 years, durable
- •Walking capacity, function improved
- •Level I evidence supports surgery
Surgical Technique
- •Prone positioning, fluoroscopy for level
- •Preserve more than 50% facet bilaterally
- •Remove ligamentum flavum (main contributor)
- •Dural tear 3-5%
Complications
- •Dural tear: 3-5%
- •Post-laminectomy instability if too much facet removed
- •Recurrent stenosis over time
- •Adjacent segment disease
Outcomes
- •70-80% improvement in claudication
- •Duration of benefit: 5-10 years
- •Reoperation rate: ~18% at 8 years (SPORT)
- •Surgical advantage durable to 4 years (SPORT)
Summary
Key Takeaways
-
Distinguish Neurogenic from Vascular Claudication: The shopping cart sign (flexion relief) is pathognomonic for neurogenic claudication. Vascular claudication improves with rest alone and has a fixed walking distance.
-
SPORT Supports Surgery for Stenosis: Unlike disc herniation, the SPORT trial showed surgery is superior to conservative treatment for stenosis at 2-4 years with durable results.
-
Preserve Facets for Stability: More than 50% of facet joints must be preserved bilaterally to maintain stability after laminectomy. Excessive resection leads to post-laminectomy instability.
-
Know When to Fuse: Add fusion when spondylolisthesis, dynamic instability, degenerative scoliosis, or more than 50% facet removal is required. FUSE mnemonic helps remember indications.
-
L4-5 Most Common Level: L4-5 is the most commonly stenotic level. Ligamentum flavum hypertrophy is a major contributor to stenosis.
-
Dural Tear is Common: 3-5% dural tear rate, higher in revision surgery and severe stenosis. Know repair techniques and postoperative management.
-
Patient Selection Matters: Best outcomes when leg symptoms predominate over back pain and imaging correlates with clinical presentation.