Nerve Root Compression | Dermatomal Patterns | Disc Herniation
ROOT LEVEL PATTERNS
Critical Must-Knows
- L5 root = EHL weakness (big toe dorsiflexion), L4-L5 disc most common
- S1 root = Ankle reflex ABSENT, calf weakness (heel walk), L5-S1 disc
- L4 root = Knee jerk reduced, quad weakness, anterior thigh numbness
- Conservative first: 6-12 weeks for most cases (90% improve)
- Cauda Equina: Saddle anesthesia + urinary retention = EMERGENCY surgery
Clinical Pearls
- "L5 root has NO reliable reflex - motor testing (EHL) is key
- "Leg pain WORSE than back pain distinguishes radiculopathy from axial LBP
- "SLR positive at 30-70° raises intrathecal pressure, reproduces leg pain
- "Crossed SLR (positive in contralateral leg) = high specificity for disc herniation
Clinical Imaging
Imaging Gallery




Critical Lumbar Radiculopathy Exam Points
Cauda Equina Syndrome
SURGICAL EMERGENCY: Saddle anesthesia, urinary retention, fecal incontinence, bilateral leg weakness. MRI + surgery within 24-48 hours. Delayed surgery = permanent bowel/bladder dysfunction.
L5 vs S1 Root
L5: EHL weakness (can't lift big toe), dorsum foot numbness, NO reliable reflex. S1: Calf weakness (can't heel raise), absent ankle jerk, lateral foot/sole numbness.
Conservative Trial
6-12 weeks of conservative treatment for most radiculopathy. 90% improve. Exceptions: Cauda equina syndrome, progressive neurological deficit, intractable pain requiring IV analgesia.
Microdiscectomy
Gold standard surgical treatment for disc herniation. 85-95% success. Faster recovery than conservative but similar long-term outcomes (SPORT trial). 5-10% reherniation rate.
Lumbar Root Patterns - Motor, Sensory, Reflex
| Root | Disc Level | Motor Weakness | Sensory Distribution | Reflex |
|---|---|---|---|---|
| L3 | L2-L3 | Hip flexion, knee extension | Anterior thigh | None reliable |
| L4 | L3-L4 | Tibialis anterior, Quadriceps | Medial leg, medial foot | Knee jerk (reduced) |
| L5 | L4-L5 | EHL, Hip abduction, Tibialis posterior | Lateral leg, dorsum foot, 1st web space | None reliable |
| S1 | L5-S1 | Gastrocnemius, Peroneals, Gluteus maximus | Lateral foot, sole, posterior calf | Ankle jerk (ABSENT) |
S1 RL5 vs S1 Radiculopathy
| L5 | Lift Big Toe EHL weakness - can't dorsiflex big toe |
| S1 | Standing on Tiptoes Calf weakness + absent ankle jerk |
| L5 | Lift Big Toe EHL weakness - can't dorsiflex big toe |
| S1 | Standing on Tiptoes Calf weakness + absent ankle jerk |
Hook:L5 Lifts toe up, S1 Stands on tiptoe down
SLR - SSLR - Straight Leg Raise Test
| S | Sensitivity 90% Good screening test |
| L | Low specificity (26%) Positive in many conditions |
| R | Radicular if 30-70° Positive range for disc pathology |
| S | Sensitivity 90% Good screening test |
| L | Low specificity (26%) Positive in many conditions |
| R | Radicular if 30-70° Positive range for disc pathology |
Hook:SLR is Sensitive but Low in Reliability for specificity
CAUDA - ECAUDA - Emergency Signs
| C | Continence (loss) Bowel and bladder dysfunction |
| A | Anesthesia (saddle) Perineal numbness |
| U | Urgent surgery Within 24-48 hours |
| D | Deficit bilateral Lower limb weakness both sides |
| A | Acute retention Urinary retention (overflow incontinence) |
| C | Continence (loss) Bowel and bladder dysfunction | D | Deficit bilateral Lower limb weakness both sides |
| A | Anesthesia (saddle) Perineal numbness | A | Acute retention Urinary retention (overflow incontinence) |
| U | Urgent surgery Within 24-48 hours |
Hook:CAUDA equina needs CAUDA assessment
Overview and Epidemiology
Lumbar Radiculopathy is a clinical syndrome caused by compression or irritation of a lumbar nerve root, resulting in pain, sensory changes, and/or motor weakness in the distribution of that nerve root.
Definition:
The term "sciatica" refers specifically to radicular pain along the sciatic nerve distribution (L4-S3), typically affecting the buttock and posterior/lateral leg. True radiculopathy includes neurological deficit (weakness, numbness, reflex changes) in addition to pain.
Epidemiology:
| Factor | Details |
|---|---|
| Prevalence | 5-10% of patients with low back pain |
| Peak age | 30-50 years (disc degeneration begins) |
| Gender | Slight male predominance (1.5:1) |
| Most common root | L5 (from L4-L5 disc) |
| Second most common | S1 (from L5-S1 disc) |
| Bilateral involvement | Rare - consider cauda equina or central disc |
Natural History:
The majority of disc herniations causing radiculopathy will improve without surgery. This forms the basis for conservative management in most cases.
Anatomy and Biomechanics
Lumbar Nerve Root Anatomy
Nerve Root Numbering:
In the lumbar spine, nerve roots exit BELOW the correspondingly numbered pedicle. The L4 root exits below the L4 pedicle, between L4 and L5.
| Disc Level | Exiting Root | Traversing Root |
|---|---|---|
| L3-L4 | L3 | L4 |
| L4-L5 | L4 | L5 |
| L5-S1 | L5 | S1 |
Posterolateral vs Central Herniation:
Most disc herniations are posterolateral, compressing the TRAVERSING root (the root that continues down to exit below the next level).
| Herniation Type | Root Affected | Example |
|---|---|---|
| Posterolateral | Traversing root | L4-L5 PL herniation → L5 root |
| Far lateral (foraminal) | Exiting root | L4-L5 FL herniation → L4 root |
| Central | Cauda equina | Large central L4-L5 → multiple roots |
Dermatomal Patterns
L4 Dermatome:
- Anterior thigh
- Medial leg to medial malleolus
- Medial foot
L5 Dermatome:
- Lateral leg
- Dorsum of foot
- First web space (pathognomonic)
- Great toe
S1 Dermatome:
- Posterior calf
- Lateral foot
- Sole of foot
- Small toe
Pathophysiology
Mechanisms of Nerve Root Compression
Mechanical Compression:
The most common cause is disc herniation, where the nucleus pulposus protrudes through a tear in the annulus fibrosus. The disc material directly compresses the nerve root against the bony canal.
| Disc Terminology | Description |
|---|---|
| Bulge | Symmetric, circumferential extension |
| Protrusion | Focal, base wider than apex |
| Extrusion | Apex wider than base, through annulus |
| Sequestration | Free fragment, separated from disc |
Chemical Inflammation:
The nucleus pulposus contains inflammatory mediators (phospholipase A2, TNF-alpha) that cause local inflammation and sensitization of the nerve root. This explains why some small herniations cause severe symptoms while large herniations may be asymptomatic.
Other Causes of Radiculopathy
Most Common Cause (90%)
Mechanism: Nucleus pulposus herniates through annular tear, compressing nerve root mechanically and chemically.
Risk Factors: Repetitive flexion-rotation loading, heavy lifting, vibration exposure (truck drivers), smoking (disc nutrition), genetic factors.
Age Pattern: Peak in 30-50 years when disc is still hydrated enough to herniate. Older patients more likely to have stenosis.
Pain Physiology
Nerve Root Pain Characteristics:
Radicular pain differs from referred pain. Radicular pain follows a dermatomal distribution and is often described as sharp, shooting, or electric. Referred pain is duller, more diffuse, and doesn't follow nerve root patterns.
Sensitization:
Chronic compression leads to nerve root sensitization, with lowered thresholds for pain signaling. This explains why minor movements can trigger severe radicular symptoms.
Classification
By Root Level
L3-L4 Disc Herniation
Motor: Knee extension (quadriceps) weakness. Difficulty rising from chair or climbing stairs.
Sensory: Anterior thigh and medial leg to medial malleolus.
Reflex: Reduced or absent knee jerk (L3-L4 reflex arc).
Clinical Tip: Less common than L5/S1. Consider femoral nerve palsy in differential. Femoral stretch test (reverse SLR) may be positive.
By Herniation Type
| Type | Location | Root Affected | Clinical Features |
|---|---|---|---|
| Posterolateral | Lateral recess | Traversing root | Classic radiculopathy, SLR positive |
| Foraminal | Neural foramen | Exiting root | One level up, may be missed on MRI |
| Central | Central canal | Multiple roots | Bilateral symptoms, cauda equina risk |
| Extraforaminal | Far lateral | Exiting root | Femoral stretch test may be positive |
Severity Grading
Motor Weakness Grading (MRC Scale):
| Grade | Description | Clinical Implication |
|---|---|---|
| 5 | Normal power | No motor deficit |
| 4 | Movement against resistance | Mild weakness - conservative |
| 3 | Movement against gravity only | Moderate weakness - consider surgery |
| 2 | Movement with gravity eliminated | Severe weakness - surgery recommended |
| 1 | Flicker of contraction | Near complete deficit - urgent surgery |
| 0 | No contraction | Complete deficit - emergency surgery |
Clinical Presentation
History
Pain Characteristics:
| Feature | Radiculopathy Pattern |
|---|---|
| Location | Leg pain worse than back pain (key feature) |
| Character | Sharp, shooting, electric |
| Distribution | Dermatomal (follows nerve root) |
| Aggravating | Sitting, coughing, straining, forward flexion |
| Relieving | Standing, lying, walking (unlike stenosis) |
Red Flags (Cauda Equina Syndrome):
Cauda Equina Syndrome - Emergency
Any combination of: saddle anesthesia, urinary retention or incontinence, fecal incontinence, bilateral leg weakness, sexual dysfunction. Requires URGENT MRI and surgical decompression within 24-48 hours.
Duration and Progression:
- Acute onset suggests disc herniation
- Gradual onset may indicate stenosis
- Progressive weakness is concerning
- Bilateral symptoms suggest central pathology
Physical Examination
Observation:
- Antalgic gait
- List away from painful side (sciatic scoliosis)
- Limited lumbar flexion
Palpation:
- Paravertebral muscle spasm
- Sciatic notch tenderness
Neurological Examination:
| Test | L4 | L5 | S1 |
|---|---|---|---|
| Motor | Knee extension | EHL, hip abduction | Plantar flexion, hip extension |
| Reflex | Knee jerk | None reliable | Ankle jerk |
| Sensory | Medial leg/foot | Lateral leg, dorsum foot | Lateral foot, sole |
Special Tests:
| Test | Technique | Positive Finding | Sensitivity/Specificity |
|---|---|---|---|
| SLR | Raise straight leg, hip flexed, knee extended | Pain 30-70° in radicular distribution | 90% sensitive, 26% specific |
| Crossed SLR | SLR reproduces pain in opposite leg | Pain in contralateral leg | Low sensitivity, HIGH specificity (90%) |
| Femoral stretch | Prone, extend hip with knee flexed | Pain in anterior thigh | Positive for L4, L3 radiculopathy |
| Slump test | Seated, chin to chest, extend knee | Reproduces radicular pain | Tension test for dura |
Crossed SLR
If raising the UNAFFECTED leg reproduces pain in the AFFECTED leg, this has 90% specificity for disc herniation. It indicates a large disc that is tenting the dura.
Differential Diagnosis
Leg pain is not always radicular. The examiner wants to see you actively exclude mimics before committing to a disc-based diagnosis. The single most useful discriminator is whether the pain is genuinely dermatomal and reproduced by neural tension, versus regional, mechanical or vascular.
Lumbar Radiculopathy vs Common Mimics
| Condition | Pain Pattern | Key Discriminator | Confirmatory Test |
|---|---|---|---|
| Disc radiculopathy | Dermatomal, leg worse than back | Positive SLR / femoral stretch, motor-sensory in one root | MRI concordant with level |
| Neurogenic claudication (central stenosis) | Bilateral buttock/leg, worse standing/walking | Relieved by flexion (shopping-cart sign), pulses normal | MRI central canal stenosis |
| Vascular claudication (PAD) | Calf cramp with exertion, fixed claudication distance | Relieved by standing still, absent pulses, no postural change | ABPI reduced, arterial duplex |
| Hip osteoarthritis | Groin/anterior thigh, rarely below knee | Pain on hip rotation (FABER/FADIR), no neuro deficit | Hip radiograph, intra-articular block |
| Greater trochanteric pain syndrome | Lateral hip/thigh | Point tenderness over trochanter, normal neurology | Resisted abduction, ultrasound |
| Peripheral neuropathy (e.g. diabetic, peroneal palsy) | Glove-and-stocking or single peripheral nerve | Does not follow a single root; NCS abnormal distally | EMG/NCS |
| Piriformis / deep gluteal syndrome | Buttock to posterior thigh | Tenderness deep to gluteus, pain on resisted external rotation | Diagnosis of exclusion, MRI normal canal |
| Sinister (tumour, infection, fracture) | Night pain, constant, non-mechanical | Red flags: weight loss, fever, malignancy history, age extremes | MRI with contrast, inflammatory markers |
The discriminator that matters
A truly positive straight leg raise (reproducing radicular leg pain at 30-70 degrees, worsened by ankle dorsiflexion) shifts you strongly toward a nerve-root cause. Pain only in the back, or only at extremes of range, is not a positive SLR and should make you reconsider a mechanical or hip source.
Investigations
Imaging Protocol
MRI (Gold Standard):
| Sequence | What It Shows |
|---|---|
| T2 sagittal | Disc degeneration (dark disc), herniations, spinal alignment |
| T2 axial | Nerve root compression, lateral recess stenosis |
| T1 | Anatomy, fat in foramen (should be bright), bone marrow |
| STIR | Bone marrow edema, infection, tumor |
When to Image:
Standard recommendation is to wait 6 weeks before MRI if no red flags, as many herniations resolve spontaneously.
Indications for Early MRI:
- Cauda equina syndrome (URGENT)
- Progressive neurological deficit
- Suspected tumor or infection
- Severe, unremitting pain
- Prior malignancy
CT Myelography:
Alternative when MRI contraindicated (pacemaker, severe claustrophobia). Shows contrast around nerve roots but less soft tissue detail.
Electrodiagnostic Studies
EMG/NCS:
| Finding | Interpretation |
|---|---|
| Denervation changes | Positive waves, fibrillations at 3+ weeks |
| Reduced recruitment | Chronic nerve injury |
| Normal study | Does NOT rule out radiculopathy (may be too early) |
Indications:
- Unclear clinical picture
- Differentiating radiculopathy from peripheral neuropathy
- Medicolegal documentation
- Pre-operative confirmation
Diagnostic Injections
Selective Nerve Root Block:
Can be diagnostic if unclear which root is symptomatic. Relief with block confirms that specific root as pain generator.
Epidural Steroid Injection:
More therapeutic than diagnostic. May provide short-term relief and help avoid surgery.
Imaging Gallery
Anatomical Relationships and Pathophysiology
Management
Treatment Algorithm
Conservative Management (First Line):
| Intervention | Evidence | Details |
|---|---|---|
| Activity modification | Strong | Avoid aggravating activities, NOT bed rest |
| NSAIDs | Strong | First-line pharmacotherapy |
| Oral steroids | Moderate | Short course (6 days) may help acute phase |
| Physical therapy | Strong | Core strengthening, McKenzie extension |
| Epidural steroid injection | Moderate | 50% avoid surgery at 1 year (Riew) |
Duration: 6-12 weeks trial before surgery unless red flags present.
Indications for Surgery:
| Indication | Timing |
|---|---|
| Cauda equina syndrome | URGENT (24-48 hours) |
| Progressive motor deficit | Early (within days) |
| Severe weakness (MRC ≤3) | Early consideration |
| Failed conservative (6-12 weeks) | Elective |
| Intractable pain | Elective |
Surgical Management
Gold Standard for Disc Herniation
Technique: Small incision, limited laminotomy/flavectomy, remove herniated disc fragment, preserve as much normal disc as possible.
Outcomes: 85-95% leg pain relief. SPORT trial showed faster recovery than conservative but similar long-term outcomes.
Complications: Dural tear (1-7%), recurrent herniation (5-10%), wrong level (rare but serious), infection (1-2%).
Reherniation: Higher risk with larger annular defect, younger age, male sex, smoking.
SPORT Trial Key Points
Spine Patient Outcomes Research Trial (SPORT): in the randomised intent-to-treat analysis, between-group differences favoured surgery but were small and not statistically significant, with very high crossover in both directions. Both groups improved substantially over 2 years. The message for the viva: surgery accelerates recovery, but it is NOT mandatory for uncomplicated disc herniation, and conservative care remains reasonable first-line treatment.
Complications
Complications of Conservative Management
Delayed Recovery:
- Prolonged disability if not appropriately managed
- Chronic pain syndrome development
- Muscle atrophy from disuse
- Psychological impact (depression, anxiety)
Missed Cauda Equina:
- Progressive neurological deficit if cauda equina not recognized
- Permanent bladder/bowel dysfunction
Surgical Complications
Intraoperative:
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Dural tear | 1-7% | Careful technique, primary repair, fibrin glue |
| Wrong level | 0.1-0.3% | Intraoperative imaging, confirm with X-ray |
| Nerve root injury | 0.1-0.5% | Adequate visualization, gentle retraction |
| Vascular injury | Very rare | Avoid plunging instruments anteriorly |
Postoperative:
| Complication | Incidence | Management |
|---|---|---|
| Recurrent herniation | 5-10% | May require revision surgery |
| Infection | 1-2% | Antibiotics, possible washout |
| Epidural hematoma | Rare | Urgent decompression if symptomatic |
| Chronic pain (FBSS) | 10-40% | Multidisciplinary management |
Long-Term Complications
Recurrent Disc Herniation:
- 5-10% at same level
- Risk factors: Large annular defect, male, smoking, young age, heavy lifting
- Treatment: Revision discectomy or fusion if recurrent
Failed Back Surgery Syndrome (FBSS):
- Persistent pain after lumbar spine surgery
- Causes: Wrong diagnosis, incomplete decompression, new pathology, scar tissue
- Management: Spinal cord stimulation, multidisciplinary pain program
Adjacent Segment Disease:
- Rare after discectomy alone
- More common after fusion
Evidence Base
All primary trials below have been verified against PubMed. According to PubMed, the records and DOIs are accurate as cited.
SPORT - Surgery vs Nonoperative Care for Lumbar Disc Herniation (RCT)
- Multicentre RCT, 501 surgical candidates with imaging-confirmed disc herniation and radiculopathy of at least 6 weeks (mean age 42, 42% women)
- Intent-to-treat differences favoured surgery for all outcomes but were small and not statistically significant for the primary measures
- Crossover was high: 50% assigned to surgery had it by 3 months, while 30% assigned to nonoperative care also had surgery
- Both groups improved substantially over 2 years; large crossover precluded firm conclusions of superiority or equivalence by ITT
Surgery vs Prolonged Conservative Treatment for Sciatica (Leiden Trial)
- RCT of 283 patients with severe sciatica for 6-12 weeks: early surgery vs prolonged conservative care with surgery if needed
- 39% of the conservative arm eventually required surgery (mean 18.7 weeks)
- Early surgery gave faster leg-pain relief and faster perceived recovery (HR 1.97, 95% CI 1.72-2.22)
- At 1 year the probability of perceived recovery was 95% in BOTH groups
Lumbar Disc Herniation - Controlled Prospective Study, 10-Year Observation
- Landmark trial; 126 patients with uncertain surgical indication randomised to surgery vs conservative care
- Statistically significant advantage for surgery at 1 year
- By 4 years the operated group was still better but the difference was no longer significant; minimal change thereafter to 10 years
- Overall natural history of radiculopathy was favourable
Guidelines, Registries & Global Practice
Global Epidemiology
- Lifetime prevalence of sciatica/radicular leg pain is commonly cited at roughly 10-40%, with annual incidence around 1-5% in adult populations.
- Radiculopathy accounts for roughly 5-10% of patients presenting with low back pain.
- Peak incidence is in the fourth and fifth decades, when the disc is still hydrated enough to herniate; in older adults degenerative foraminal and central stenosis becomes a relatively more common cause.
- L4-L5 and L5-S1 together account for the large majority of herniations, making L5 and S1 the most frequently affected roots worldwide.
Side-by-Side Guideline Comparison
How Major Societies Frame Radiculopathy Care
| Body | Imaging Stance | Injections | Surgery Threshold |
|---|---|---|---|
| NICE NG59 (UK) | Only if it will change management; not routine in primary care | Consider epidural LA + steroid for acute severe sciatica | Decompression when conservative care fails AND imaging is concordant |
| NASS (North America) | MRI is the imaging of choice for suspected herniation | Transforaminal ESI an option for short-term relief | Discectomy for persistent concordant radiculopathy failing 6+ weeks conservative care |
| AO Spine / general consensus | MRI to confirm level and laterality before surgery | Reasonable adjunct/diagnostic tool | Urgent surgery for CES or progressive deficit; otherwise elective |
| Broad international consensus | Avoid early imaging without red flags | Modest, mainly short-term benefit | Red flags (CES, progressive motor loss) override the conservative trial |
The areas of genuine agreement are larger than the disagreements: avoid early imaging without red flags, offer a conservative trial of around 6-12 weeks for uncomplicated cases, and decompress urgently for cauda equina or progressive deficit. Differences are mostly of emphasis - the relative weight placed on injections and the exact conservative-trial duration.
Registry and Outcome Notes
- Spine surgery registries (for example the Norwegian NORspine registry and several national spine outcome databases) consistently report substantial improvement in leg pain and disability after microdiscectomy, with reoperation/recurrence rates in the order of 5-15% over medium-term follow-up.
- Registry data reinforce the RCT message: minimally invasive and open microdiscectomy yield comparable patient-reported outcomes, so technique choice is driven by expertise rather than a proven outcome advantage.
High- vs Limited-Resource Practice Variation
| Setting | Typical Pathway | Rationale / Constraint |
|---|---|---|
| Well-resourced | Early MRI when red flags present, ready access to ESI and elective microdiscectomy, emergency MRI for suspected CES | Imaging and theatre access readily available |
| Limited-resource | Greater reliance on clinical diagnosis and conservative care; selective use of MRI; CT myelography where MRI is scarce | MRI access and cost limit early imaging; clinical examination carries more diagnostic weight |
A clinically confident diagnosis of single-level radiculopathy can be made and managed conservatively on history and examination alone; advanced imaging is mandatory before surgery and for any suspicion of cauda equina, infection or tumour.
Controversies and Areas of Uncertainty
Timing of surgery
Early surgery clearly speeds recovery (Peul, Leiden trial), but 1-year outcomes match watchful waiting. Whether earlier surgery prevents long-term residual deficit in those with motor weakness remains debated.
Epidural / nerve-root steroid injections
Benefit is real but mainly short-term and modest. Their role as a surgery-sparing tool (Riew) versus a temporising measure of limited durability is still contested across guidelines.
The 'safe' window in cauda equina
The 48-hour signal from meta-analysis (Ahn) should not be read as permission to wait. Most surgeons decompress as soon as feasible; incomplete CES (CES-I) carries a better prognosis than retention (CES-R), and the data are retrospective.
Minimally invasive vs open
Long-term RCT data show no clinically meaningful difference. Endoscopic and tubular techniques offer perioperative advantages in selected hands but no proven superiority in patient-reported outcomes.
Additional unsettled questions include: the value of routine EMG/NCS (rarely changes management in clinically clear cases), how aggressively to operate on isolated painless motor weakness, and whether sequestrated fragments resorb often enough to justify prolonged conservative care even with large herniations.
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Classic L5 Radiculopathy
"A 38-year-old male presents with 6 weeks of right leg pain radiating to the dorsum of the foot. He has weakness lifting his big toe. MRI shows L4-L5 right posterolateral disc herniation."
Cauda Equina Syndrome
"The same patient now presents to emergency with bilateral leg weakness, difficulty voiding, and numbness around the perineum."
S1 Radiculopathy with Absent Reflex
"A 45-year-old female presents with 8 weeks of left posterior calf pain and numbness on the sole of her foot. Ankle jerk is absent on the left. SLR is positive at 45 degrees."
Far Lateral Disc Herniation
"A 52-year-old male has 4 weeks of anterior thigh pain and weakness climbing stairs. SLR is negative, but femoral stretch test is positive. MRI shows L3-L4 far lateral disc herniation."
Management Algorithm
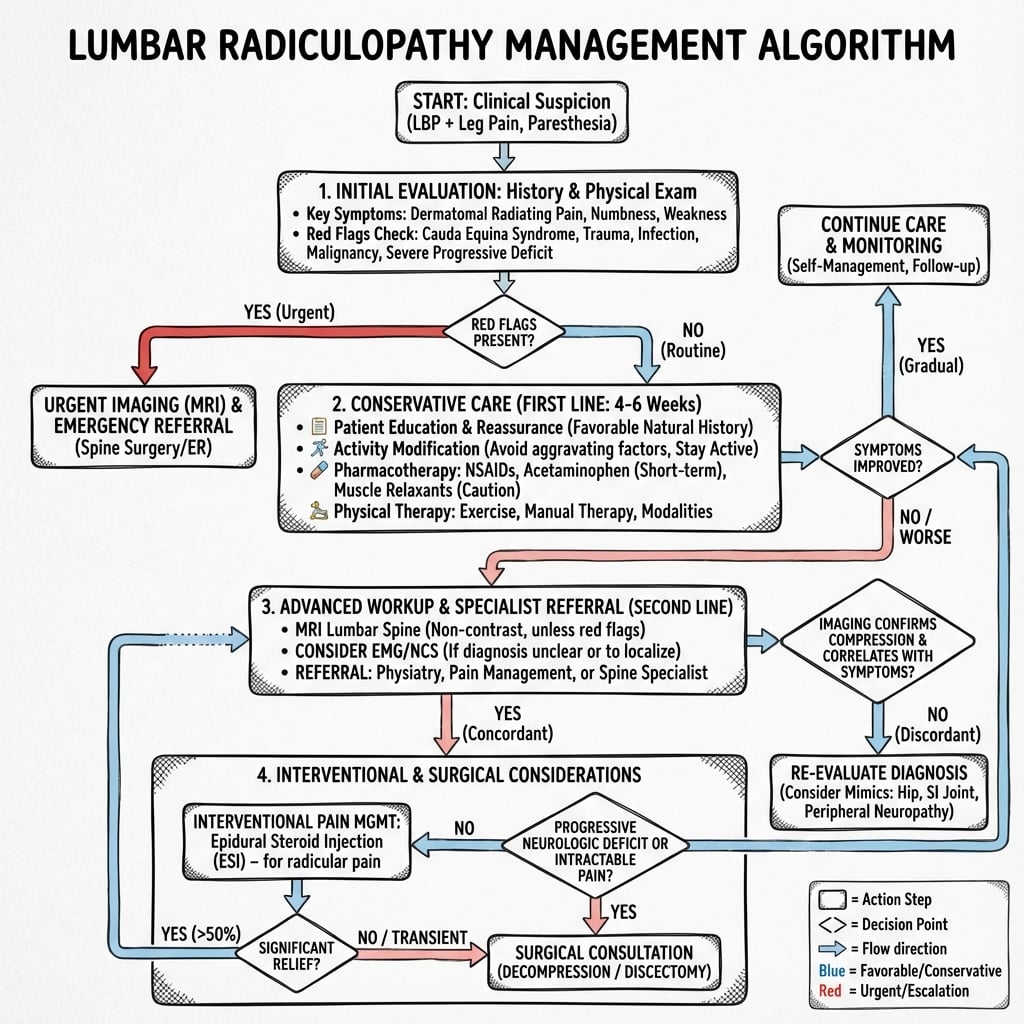
LUMBAR RADICULOPATHY
Clinical summary
ROOT PATTERNS
- •L4: Knee extension weak, reduced knee jerk, medial leg
- •L5: EHL weakness, NO reflex, dorsum foot/1st web space
- •S1: Calf weakness, ABSENT ankle jerk, lateral foot/sole
KEY CLINICAL FEATURES
- •Leg pain WORSE than back pain
- •Dermatomal distribution of symptoms
- •SLR positive at 30-70 degrees
- •Crossed SLR = high specificity for disc
DISC MECHANICS
- •Posterolateral herniation affects TRAVERSING root
- •Far lateral herniation affects EXITING root (one level up)
- •L4-L5 PL = L5 root; L4-L5 FL = L4 root
- •Central herniation = risk of cauda equina
CAUDA EQUINA EMERGENCY
- •Saddle anesthesia + urinary retention
- •Bilateral leg symptoms
- •MRI + surgery within 24-48 hours
- •Delayed surgery = permanent deficits
MANAGEMENT PEARLS
- •Conservative first: 6-12 weeks, 90% improve
- •Microdiscectomy: 85-95% leg pain relief
- •SPORT trial: surgery faster but similar long-term
- •ESI: 50% avoid surgery at 1 year (Riew)