Progressive Instability | Mayfield Stages | Emergent Reduction | Ligament Reconstruction
MAYFIELD PROGRESSIVE PERILUNAR INSTABILITY
Critical Must-Knows
- 25% missed initially - always look for carpal arc disruption on lateral X-ray
- Spilled teacup sign = Stage IV lunate dislocation (lunate tips volar into carpal tunnel)
- Mayfield progression: SL then capitolunate then lunotriquetral ligaments fail sequentially
- Acute median nerve symptoms common in Stage IV - urgent reduction required
- Greater arc injuries = fracture-dislocations (trans-scaphoid most common)
Clinical Pearls
- "Lateral X-ray: Lunate should articulate with both radius and capitate
- "Lesser arc = pure ligamentous; Greater arc = bone fractures
- "Trans-scaphoid perilunate = scaphoid fracture + perilunate dislocation
- "Open reduction via combined volar + dorsal approach preferred
Clinical Imaging
Imaging Gallery



Critical Perilunate/Lunate Dislocation Points for Exams
25% Missed Diagnosis
One quarter of perilunate/lunate dislocations are missed on initial presentation. Always examine the lateral X-ray carefully - the lunate should articulate with both the radius and the capitate.
Mayfield Progression
Sequential ligament failure: Scapholunate (I) then capitolunate (II) then lunotriquetral (III) then lunate tips volar (IV). Understanding this helps identify the stage and predict associated injuries.
Median Nerve Emergency
Acute carpal tunnel syndrome is common across perilunate injuries (acute median neuropathy in ~47%; Wickramasinghe 2015) and is especially associated with volar lunate dislocation (Stage IV). The volarly dislocated lunate compresses the median nerve. Urgent reduction is critical to relieve sustained compression.
Greater vs Lesser Arc
Lesser arc = pure ligamentous injury around lunate. Greater arc = fractures through bones (trans-scaphoid most common). Greater arc injuries have better bone healing but worse overall outcomes.
At a Glance
Perilunate and lunate dislocations represent a spectrum of high-energy carpal injuries following the Mayfield progression of ligamentous disruption. Perilunate dislocation (Mayfield Stage III) maintains the lunate in the lunate fossa while the carpus dislocates dorsally. Lunate dislocation (Mayfield Stage IV) shows volar lunate displacement into the carpal tunnel ("spilled teacup" sign). Trans-scaphoid perilunate is the most common greater arc injury. These injuries are commonly missed on initial X-rays (25%). Treatment is urgent open reduction with ligament repair to prevent median nerve damage and progressive carpal instability.
Lunate vs Perilunate Dislocation Comparison
Greater Arc vs Lesser Arc Injuries
MnemonicCards
S-C-L-TMayfield Stages
| S | Scapholunate Stage I - SL ligament disruption |
| C | Capitolunate Stage II - Capitate dislocates from lunate |
| L | Lunotriquetral Stage III - Perilunate dislocation complete |
| T | Tipped Stage IV - Lunate tips volar (lunate dislocation) |
| S | Scapholunate Stage I - SL ligament disruption | L | Lunotriquetral Stage III - Perilunate dislocation complete |
| C | Capitolunate Stage II - Capitate dislocates from lunate | T | Tipped Stage IV - Lunate tips volar (lunate dislocation) |
Hook:S-C-L-T: Scapholunate, Capitolunate, Lunotriquetral, Tipped volar - progressive failure pattern
BONE vs LIGAGreater vs Lesser Arc
| B | Bone Greater arc passes through bones |
| O | Often scaphoid Trans-scaphoid most common |
| N | Not just ligaments Fractures present |
| E | Easier union Bone heals better than ligament |
| B | Bone Greater arc passes through bones | N | Not just ligaments Fractures present |
| O | Often scaphoid Trans-scaphoid most common | E | Easier union Bone heals better than ligament |
Hook:Greater arc = Greater bone involvement; Lesser arc = Less bone, more ligament
TRAPClosed Reduction Steps
| T | Traction Longitudinal finger traction first |
| R | Recreate Recreate deformity by extending wrist |
| A | Apply pressure Thumb pressure over dorsal carpus |
| P | Push and flex Push carpus volar while flexing wrist |
| T | Traction Longitudinal finger traction first | A | Apply pressure Thumb pressure over dorsal carpus |
| R | Recreate Recreate deformity by extending wrist | P | Push and flex Push carpus volar while flexing wrist |
Hook:TRAP the lunate back in place: Traction, Recreate, Apply pressure, Push and flex
Overview
Perilunate and lunate dislocations represent a spectrum of high-energy carpal injuries characterized by progressive failure of the perilunate ligamentous structures. These injuries are frequently missed on initial presentation (up to 25% of cases), leading to delayed diagnosis and poorer outcomes.
The mechanism involves forced hyperextension, ulnar deviation, and intercarpal supination, typically from a fall on an outstretched hand with the wrist in dorsiflexion. The injury progresses through predictable stages (Mayfield classification) as sequential ligaments fail.
Key Concepts:
- Perilunate dislocation: Lunate remains articulated with radius; carpus dislocates dorsally around it
- Lunate dislocation: Lunate dislocates volarly while proximal carpal row reduces
- Both are part of a continuous spectrum of progressive perilunar instability
- Associated fractures (greater arc) are common, especially scaphoid
Anatomy
Perilunate Ligamentous Anatomy
The lunate is the keystone of the proximal carpal row, with critical ligamentous attachments:
Intrinsic Ligaments (Interosseous):
- Scapholunate ligament: Strongest dorsally, key stabilizer
- Lunotriquetral ligament: Strongest volarly
- Both critical for carpal stability
Extrinsic Ligaments:
- Volar radiocarpal ligaments: RSC (radioscaphocapitate), LRL (long radiolunate), SRL (short radiolunate)
- Dorsal radiocarpal ligaments: DRC (dorsal radiocarpal)
- Space of Poirier: Weak zone between RSC and LRL - path of lunate dislocation
Greater Arc vs Lesser Arc
Lesser Arc (Pure Ligamentous):
- Injury passes through ligaments only
- Arc around the lunate through SL, capitolunate space, LT ligament
- Pure soft tissue injury
- More challenging reconstruction
Greater Arc (Fracture-Dislocation):
- Injury passes through bones
- Common fracture patterns:
- Trans-scaphoid (most common)
- Trans-radial styloid
- Trans-capitate
- Trans-triquetral
- Bone healing potentially easier than ligament healing
Classification Systems
Mayfield Progressive Perilunar Instability
The Mayfield classification describes the sequential failure of perilunate structures.
Stage I - Scapholunate Dissociation: Disruption of scapholunate interosseous ligament. Scaphoid flexes, lunate extends (DISI pattern begins). Widened SL interval on PA X-ray (greater than 3mm). Terry Thomas sign (gap between scaphoid and lunate).
Stage II - Capitolunate Dissociation: Space of Poirier disrupts (between RSC and LRL ligaments). Capitate dislocates dorsally relative to lunate. Lunate still articulates with radius. Progressive ligament failure continues.
Stage III - Perilunate Dislocation: Lunotriquetral ligament fails. Entire carpus dislocates dorsally around lunate. Lunate remains in lunate fossa of radius (key point). Capitate no longer articulates with lunate. Lateral X-ray shows dorsal capitate displacement.
Stage IV - Lunate Dislocation: Dorsal radiocarpal ligament fails (final ligament). Lunate rotates and tips volarly out of lunate fossa. Lunate enters carpal tunnel ("spilled teacup"). Acute median nerve compression is common across the perilunate spectrum (reported in approximately 47% of all perilunate injuries; Wickramasinghe 2015) and is especially associated with volar lunate dislocation. Surgical emergency if nerve symptoms present.
Pathophysiology
Mechanism of Injury
Typical mechanism:
- Fall on outstretched hand (FOOSH)
- Wrist in dorsiflexion
- Combined hyperextension + ulnar deviation + intercarpal supination
- High-energy trauma (MVA, fall from height, sports)
Force transmission:
- Axial load through palm
- Ground reaction force applied to thenar eminence
- Wrist forced into hyperextension
- Sequential ligament failure from radial to ulnar side
Median Nerve Emergency
Perilunate injuries frequently cause acute median neuropathy (reported in approximately 47% across the spectrum; Wickramasinghe 2015), and acute carpal tunnel syndrome is especially associated with volar lunate dislocation (Stage IV) where the displaced lunate directly compresses the median nerve. Emergent reduction is required - prolonged sustained nerve compression risks permanent damage.
Clinical Assessment
History
Mechanism:
- High-energy trauma typically
- Fall on outstretched hand
- Motor vehicle accident
- Sports injury (contact sports, cycling)
Symptoms:
- Severe wrist pain
- Rapid swelling
- Inability to move wrist
- Numbness in median nerve distribution (especially Stage IV)
- History may include feeling of "pop" or "shift"
Physical Examination
Inspection:
- Marked swelling of wrist
- Loss of normal wrist contour
- May see dorsal prominence (perilunate) or volar fullness (lunate)
- Skin tension assessment critical
Palpation:
- Diffuse tenderness
- Possible palpable lunate volarly (Stage IV)
- Assess for open injury or skin compromise
Neurovascular Examination:
- Critical: Median nerve function assessment
- Sensation in thumb, index, middle finger
- Thenar muscle strength (opponens pollicis)
- Two-point discrimination
- Compare with contralateral side
Range of Motion:
- Severely limited due to pain
- Do not force examination
- Document baseline for postoperative comparison
Red Flags Requiring Emergent Intervention
- Acute carpal tunnel symptoms (numbness, tingling, weakness)
- Open injury
- Skin blanching or tension
- Vascular compromise
- Compartment syndrome signs
Differential Diagnosis
The painful, swollen, deformed wrist after a fall on the outstretched hand has several mimics. The single most important discriminator is the lateral radiograph: in a perilunate/lunate dislocation the normal radius-lunate-capitate colinearity is lost. Failure to make this distinction underlies the 25% missed-diagnosis rate (Herzberg 1993).
Differential Diagnosis of the Acutely Injured Wrist
Investigations
Plain Radiographs
Standard Views:
- PA (posteroanterior)
- True lateral
- Oblique views
PA View Findings:
Normal landmarks (Gilula's arcs):
- Arc I: Proximal articular surfaces of proximal row
- Arc II: Distal articular surfaces of proximal row
- Arc III: Proximal articular surfaces of capitate/hamate
Abnormal findings:
- Disruption of Gilula's arcs
- Widened SL interval (greater than 3mm = "Terry Thomas sign")
- Overlap or crowding of carpal bones
- Triangular or pie-shaped lunate = rotated lunate
Lateral View Findings:
Normal alignment:
- Radius, lunate, and capitate should be collinear
- Lunate "cup" should hold capitate "ball"
Perilunate dislocation (Stage III):
- Lunate remains in lunate fossa
- Capitate dislocated dorsally
- Lunate no longer articulates with capitate
Lunate dislocation (Stage IV):
- Lunate tilted volarly out of fossa
- "Spilled teacup" appearance
- Capitate may partially reduce into lunate fossa
Spilled Teacup Sign
On lateral X-ray, the lunate normally appears like a cup holding the capitate. In Stage IV lunate dislocation, the lunate rotates and "spills" volarly - the spilled teacup sign. This is pathognomonic for lunate dislocation.
CT Scan
Indications:
- Confirm diagnosis
- Identify associated fractures (greater arc injuries)
- Pre-operative planning
- Assess reduction quality post-operatively
Key Findings:
- Fracture lines in scaphoid, capitate, triquetrum, or styloid
- Extent of articular involvement
- Fragment size and displacement
MRI
Indications:
- Usually not needed acutely
- May help assess ligament integrity subacutely
- Useful for planning staged reconstruction
Findings:
- Ligament tears (SL, LT)
- Bone bruising pattern
- TFCC injury assessment
Management Algorithm
Initial Assessment and Closed Reduction
Initial Assessment:
- Assess neurovascular status immediately (critical: median nerve function)
- Document mechanism of injury
- Assess skin integrity and tension
- Obtain PA, lateral, and oblique X-rays
- Splint in position of comfort initially
Indications for Emergent Closed Reduction:
- Acute carpal tunnel syndrome (Stage IV lunate dislocation)
- Skin compromise or threatened skin
- Open injury
- Vascular compromise
Closed Reduction Technique (TRAP):
- Traction: Apply longitudinal traction through fingers
- Recreate: Initially increase wrist extension to disengage and recreate deformity
- Apply pressure: Thumbs over dorsum, apply pressure over dorsal carpus
- Push and flex: Push carpus volarly while flexing wrist
- Verify reduction: Immediate post-reduction films
- Analgesia: Regional block or procedural sedation required
Post-Reduction Management:
- Splint in neutral position
- Repeat neurovascular examination
- Confirm reduction on X-ray
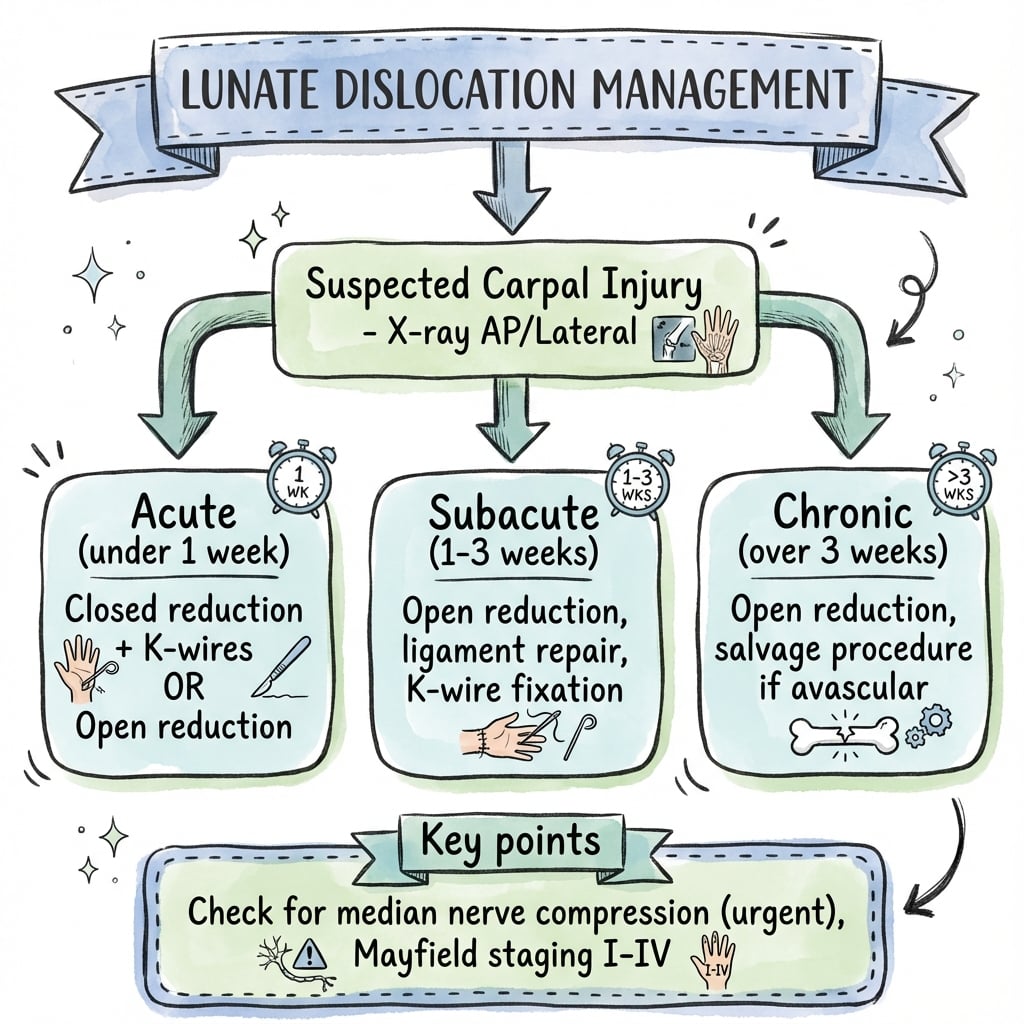
- Arrange definitive surgery within 24-72 hours (within 7-14 days ideally)
Critical Note: Closed reduction is temporizing only. ALL perilunate/lunate dislocations require definitive surgical treatment. Closed treatment alone results in unacceptable rates of instability and arthritis.
If Closed Reduction Fails: Emergent open reduction in operating theater. Interposed tissue is preventing reduction.
Surgical Technique
Positioning and Preparation
Patient Positioning:
- Supine position
- Arm on hand table
- Upper arm tourniquet applied
- Exsanguinate with elevation (avoid Esmarch if concern for fracture displacement)
Approach Selection: Combined volar plus dorsal approach preferred for all perilunate/lunate dislocations. Volar approach performed first for carpal tunnel release and lunate visualization. Dorsal approach then used for definitive reduction and fixation. Single approach inferior to combined approach which provides better visualization and outcomes.
Complications
Early Complications
Median Nerve Injury:
- Acute compression from displaced lunate (Stage IV)
- Iatrogenic during reduction
- Carpal tunnel syndrome post-operatively
- Usually improves with reduction and CTR
Infection:
- Higher risk with open injuries
- Standard surgical infection risk
Failure of Reduction:
- Interposed tissue (capsule, tendons)
- Inadequate surgical technique
- May require repeat surgery
Late Complications
Post-traumatic Arthritis:
- Most common long-term complication
- Occurs in 50-70% at long-term follow-up
- May be asymptomatic
- Radiocarpal and midcarpal joints affected
Carpal Instability:
- Recurrent SL or LT dissociation
- Progressive collapse patterns (SLAC, SNAC equivalent)
- May require salvage procedures
Scaphoid Nonunion:
- In trans-scaphoid perilunate injuries
- Risk factors: Delay, inadequate fixation, smoking
- Requires revision surgery with bone grafting
AVN of Lunate:
- Rare but devastating
- Blood supply vulnerable during injury
- May lead to Kienböck's pattern
- Limited salvage options
Stiffness:
- Expected to some degree
- ROM typically 50-70% of normal
- Grip strength 60-80% of normal
- Therapy critical for optimization
Complex Regional Pain Syndrome
- Rare but serious complication
- Early recognition and treatment essential
- Multidisciplinary approach required
Postoperative Care
Immediate Postoperative (Day 0-2):
- Strict elevation to reduce swelling
- Neurovascular checks every 2 hours initially
- Watch for compartment syndrome (rare but catastrophic)
- Pain control with multimodal analgesia
- Finger range of motion exercises started immediately
Week 0-2:
- Volar splint or short arm cast
- Strict wrist immobilization
- Continue finger ROM
- First dressing change at 2 weeks
- Wound check and suture removal
Week 2-6:
- Continue immobilization
- May transition to removable splint for hygiene
- No active wrist motion yet
- K-wires remain in situ
- Serial X-rays every 2 weeks to assess alignment
Week 6-8 (K-wire Removal):
- X-rays to confirm maintained reduction
- K-wire removal in clinic (local anesthesia)
- Begin gentle active ROM exercises
- Avoid forceful grip or loading
- Hand therapy initiated
Week 8-12:
- Progressive ROM exercises
- Begin gentle strengthening
- Therapist-supervised program
- May use heat before exercises
- Continue to protect from forceful loading
Week 12-16:
- Unrestricted ROM exercises
- Progressive strengthening with weights
- Putty and grip exercises
- Functional activities
Month 4-6:
- Return to work (light duty may be earlier)
- Sports return based on individual progress
- Heavy labor typically 6 months minimum
- Expect ROM 50-70% of normal long-term
- Expect grip strength 60-80% of normal
Long-Term Follow-Up:
- X-rays at 6 months and 1 year
- Monitor for post-traumatic arthritis development
- Counsel regarding arthritis risk (50-70%)
- Salvage options if symptomatic arthritis develops
Outcomes/Prognosis
Functional Outcomes
Range of Motion:
- Expect 50-70% of normal wrist ROM long-term
- Extension typically most affected (loss of 30-40 degrees)
- Flexion loss of 20-30 degrees
- Radial/ulnar deviation relatively preserved
- Forearm rotation usually normal
Strength:
- Grip strength typically 60-80% of contralateral side
- Improves with therapy and time
- Plateaus around 12-18 months
Pain:
- Most patients have some residual pain
- Usually activity-related
- May worsen with arthritis development
- Pain scores improve with time if no arthritis
Return to Activities:
- Light work: 3-4 months
- Heavy labor: 6 months minimum
- Contact sports: 6-9 months
- Full recovery plateau: 12-18 months
Prognostic Factors
Good Prognosis Factors:
- Early treatment (within 7-14 days)
- Anatomic reduction achieved
- Secure ligament repair
- Greater arc injury (paradoxically - better bone healing)
- Young patient with good bone quality
- Compliant with therapy
Poor Prognosis Factors:
- Delayed diagnosis (over 4 weeks)
- Incomplete or malreduced carpus
- Failed ligament repair
- Lesser arc injury (poorer ligament healing)
- Associated nerve injury
- Multiple carpal fractures
- High-energy mechanism
Long-Term Arthritis Risk
Post-Traumatic Arthritis:
- Develops in 50-70% of patients by 5-10 years
- Radiographic arthritis often asymptomatic initially
- Risk factors:
- Residual carpal malalignment
- Articular cartilage damage at injury
- Chronic instability
- Delayed treatment
Arthritis Patterns:
- Radiocarpal joint most commonly affected
- Midcarpal joint (capitolunate) also common
- May progress to scaphoid nonunion advanced collapse (SNAC) or scapholunate advanced collapse (SLAC) equivalent pattern
Management of Symptomatic Arthritis:
- Conservative: NSAIDs, activity modification, splinting
- Injections: Corticosteroid for temporary relief
- Salvage surgery options:
- Proximal row carpectomy (if capitate articular surface intact)
- Four-corner fusion
- Total wrist fusion (last resort for severe symptoms)
- Wrist denervation for pain relief
Evidence Base
Carpal Dislocations: Pathomechanics & Progressive Perilunar Instability (Landmark)
- Cadaveric study loading 32 wrists to failure produced 13 perilunate and 2 lunate dislocations via a reproducible mechanism of extension, ulnar deviation and intercarpal supination.
- Established the four sequential stages of perilunar instability (PLI), from scapholunate diastasis (Stage I) to complete lunate dislocation (Stage IV), with progressively greater carpal instability.
- Reduction was achieved by reversing the mechanism (intercarpal pronation, radial deviation, palmar flexion).
Perilunate Dislocations & Fracture-Dislocations: Multicentre Study (Landmark)
- In 166 injuries from 7 centres the diagnosis was missed initially in 41 cases (25%).
- Displacement was dorsal in 97%; trans-scaphoid perilunate fracture-dislocation accounted for 61% of the whole series.
- Open injury and delayed treatment adversely affected clinical results; post-traumatic arthritis occurred in 56% even in early-treated cases.
Outcomes of Acute Perilunate Injuries: Systematic Review & Meta-Analysis
- Pooled 550 patients with 553 operatively treated acute perilunate injuries (106 dislocations, 447 fracture-dislocations).
- Overall complication rate 15.0%, driven by secondary loss of reduction (10.1%); reoperation 10.4% and salvage procedures only 2.8%.
- Secondary loss of reduction was higher for pure dislocations than fracture-dislocations (24.2% vs 7.0%, RR 3.5). Radiological osteoarthritis was common and increased with follow-up but did not correlate with reduced function or dissatisfaction.
Perilunate Injury Timing & Treatment Options: Systematic Review
- Perilunate injuries represent approximately 7% of all carpal traumas and are frequently missed.
- Clinical outcomes are good when surgery is performed within 7 days; outcomes are inferior with delay and worst when treatment is delayed beyond 6 weeks.
- Chronic pure dislocations fare worse than chronic fracture-dislocations, supporting early referral to centralised units.
Acute Median Neuropathy & Carpal Tunnel Release in Perilunate Injuries
- Across 71 patients with perilunate dislocation or fracture-dislocation over 10 years at two trauma centres, acute median neuropathy was diagnosed in 33 patients (47%).
- No demographic or injury factor reliably predicted who developed median nerve symptoms.
- Carpal tunnel release during initial surgery was related to the presence of median nerve symptoms.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Missed Perilunate Dislocation
"A 35-year-old motorcyclist presents 2 weeks after a fall with persistent wrist pain and weakness. Initial X-rays at another hospital were reported as 'normal'. Current examination shows median nerve paresthesias. You review the original X-rays."
Exceptional Answer Framework:
This scenario illustrates the commonly missed perilunate injury - 25% are missed initially (Herzberg 1993). The key to diagnosis is careful examination of the lateral X-ray: the lunate should articulate with both the radius and the capitate. If the capitate is dorsal to the lunate, it's a perilunate dislocation (Stage III); if the lunate has tipped volar, it's a lunate dislocation (Stage IV).
Clinical assessment: Median nerve symptoms suggest significant injury. I would examine for acute carpal tunnel syndrome - sensory loss in median territory, thenar weakness, Phalen's and Tinel's positive.
Management of delayed presentation:
- Urgent CT to assess reduction status and identify any fractures
- Surgery indicated despite delay - outcomes worse but still better than non-operative
- Combined volar-dorsal approach: Volar for CTR and direct visualization of lunate; Dorsal for ligament repair
- Ligament repair may be more difficult due to scarring
- Consider ligament reconstruction if primary repair not possible
Counsel patient: increased risk of stiffness and arthritis with delayed treatment. Expected ROM 50-70% of normal. Radiographic arthritis develops in 50-70% long-term.
Acute Lunate Dislocation with CTS
"A 28-year-old man presents to ED 4 hours after a high-speed motorcycle accident. He has severe wrist pain and reports numbness in his thumb, index, and middle fingers that is worsening. X-rays show a Stage IV lunate dislocation with the lunate tilted into the carpal tunnel."
Exceptional Answer Framework:
This is a surgical emergency. Stage IV lunate dislocation with acute median nerve compression requires urgent intervention. The median nerve can suffer permanent damage with sustained compression beyond 6-8 hours.
Immediate management:
- Document neurovascular status carefully (baseline for comparison)
- Closed reduction under sedation in ED - do not delay for theater
- Technique (TRAP): Traction, Recreate deformity with extension, Apply dorsal thumb pressure, Push volar while flexing
- Post-reduction X-ray and neurovascular reassessment
- Splint in neutral
If reduction successful: Neurovascular symptoms should improve. Proceed to definitive surgery within 24-72 hours via combined approach with mandatory CTR.
If reduction fails: Emergent open reduction in operating theater. This is an absolute indication for immediate surgery - interposed tissue preventing reduction.
Surgical approach: Combined volar + dorsal approach preferred. Volar for CTR and direct lunate reduction; dorsal for ligament repair and K-wire fixation. Consider suture anchor repair of SL ligament. Cast 6 weeks, K-wires out at 6-8 weeks.
Trans-Scaphoid Perilunate Fracture-Dislocation
"A 32-year-old construction worker fell from scaffolding. X-rays show a perilunate dislocation with a scaphoid waist fracture. The carpus is displaced dorsally with the lunate remaining in the lunate fossa. No median nerve symptoms."
Exceptional Answer Framework:
This is a trans-scaphoid perilunate fracture-dislocation - the most common greater arc injury. The force passes through the scaphoid (fracture) and then through the LT ligament (disruption), rather than through the SL ligament as in lesser arc injuries.
Key distinction: Greater arc injuries involve bone fractures; lesser arc are pure ligamentous. The scaphoid fracture actually simplifies one aspect - bone heals better than ligament - but we must still address the LT ligament.
Surgical approach:
- Combined volar + dorsal approach (even without acute CTS, volar gives scaphoid access)
- Reduce and fix scaphoid first - anatomic reduction, headless compression screw (Herbert type)
- Dorsal approach for LT ligament repair - suture anchor or direct repair
- K-wire augmentation of reduction (LT, possibly SC)
- Capsular repair and closure
Prognosis considerations: Interestingly, greater arc injuries may have better overall outcomes than pure ligamentous injuries because bone heals more reliably than ligament. However, scaphoid nonunion is a risk, and post-traumatic arthritis still occurs in 50-70%.
MCQ Practice Points
Mayfield Staging Question
Q: In Mayfield Stage III perilunate instability, where is the lunate located?
A: In Stage III (perilunate dislocation), the lunate remains in the lunate fossa of the radius. The capitate and rest of the carpus dislocate dorsally around it. In Stage IV (lunate dislocation), the lunate tips volarly out of the fossa.
Lateral X-ray Interpretation Question
Q: What is the "spilled teacup" sign?
A: The spilled teacup sign is seen on lateral X-ray in Stage IV lunate dislocation. Normally, the lunate looks like a cup holding the capitate. When the lunate dislocates volarly and rotates, it appears to have "spilled" out of its normal position - pathognomonic for lunate dislocation.
Greater vs Lesser Arc Question
Q: What is the difference between greater and lesser arc injuries in perilunate dislocations?
A: Lesser arc injuries are pure ligamentous - the injury arc passes through the SL ligament, around the lunate, and through the LT ligament. Greater arc injuries involve fractures - the arc passes through bones (most commonly trans-scaphoid). Greater arc injuries have fractures that need fixation in addition to ligament repair.
Emergency Management Question
Q: What is the urgency of treatment for a Stage IV lunate dislocation with median nerve symptoms?
A: This is a surgical emergency. The volarly dislocated lunate compresses the median nerve in the carpal tunnel. Urgent closed reduction should be attempted immediately (within hours), and definitive surgical treatment with carpal tunnel release is required. Permanent median nerve damage can occur with compression beyond 6-8 hours.
Missed Diagnosis Question
Q: What percentage of perilunate/lunate dislocations are missed on initial presentation?
A: 25% (one quarter) of these injuries are missed initially. This emphasizes the importance of careful examination of the lateral X-ray and maintaining high clinical suspicion. The lunate should articulate with both the radius and the capitate on a normal lateral view.
Guidelines, Registries & Global Practice
Global Epidemiology
Perilunate injuries are rare but consistently under-recognised. They constitute roughly 7% of all carpal traumas in a pooled systematic review (van der Oest 2021), and pure carpal-bone dislocations are far less common than the much more frequent scaphoid fracture in population series (in a Singapore carpal-fracture cohort the scaphoid accounted for 99 of 162 carpal fractures, with only a small minority being perilunate fracture-dislocations; Hey 2011). Across the literature the demographic is strikingly uniform worldwide: young men injured by high-energy mechanisms (falls from height, road trauma, sport), reflecting the force required to fail the perilunate ligamentous ring.
Global Epidemiology & Burden (PubMed-verified)
Guideline & Consensus Landscape
No major society publishes a disease-specific clinical practice guideline dedicated to perilunate/lunate dislocations; management rests on body-of-evidence consensus rather than formal AAOS/NICE guidance. The points of broad international agreement are summarised below.
Consensus Across Guidance Bodies & Evidence Synthesis
Registries
There is no dedicated international perilunate-injury registry, and arthroplasty registries (AOANJRR, the UK NJR, the American AJRR) do not capture these soft-tissue/carpal injuries because they are not arthroplasty procedures. The best population-level data therefore come from trauma databases and pooled systematic reviews (Liechti 2023; van der Oest 2021) rather than from a formal registry.
Practice Variation & Service Delivery
Internationally, the dominant modifiable factor is timely recognition and referral rather than choice of implant. Practice variation centres on approach (combined dorsal-volar versus dorsal-only versus arthroscopic-assisted reduction and fixation) and on routine versus selective carpal tunnel release; pooled data favour less invasive techniques where the injury pattern allows (Liechti 2023). High-income trauma systems with 24/7 hand-surgery cover and ready CT access achieve earlier definitive fixation, whereas in many settings inter-hospital transfer from regional centres is the rate-limiting step to surgery within the optimal window.
Australian Context
In Australia these high-energy injuries are triaged through major trauma networks to centres with hand-surgery support; inter-hospital transfer from regional centres is often required to achieve timely definitive fixation. CT is readily available at major trauma centres and is essential to distinguish trans-scaphoid (greater-arc) fracture-dislocations from pure ligamentous injuries and to plan fixation. Hand-therapy rehabilitation is accessible through public and private sectors, with return to heavy manual work typically around 4-6 months, though access can be limited in rural and remote regions. Workplace injuries are covered by state-based workers' compensation (WorkCover) schemes and road-trauma cases by state compulsory third-party (CTP) insurance; careful documentation of mechanism, initial neurovascular status and functional impairment is important for medico-legal and permanent-impairment assessment.
LUNATE AND PERILUNATE DISLOCATIONS
Clinical summary
Mayfield Stages
- •Stage I: SL dissociation
- •Stage II: Capitolunate dissociation
- •Stage III: Perilunate dislocation (lunate in fossa, carpus dorsal)
- •Stage IV: Lunate dislocation (lunate volar = spilled teacup)
Key X-ray Findings
- •Lateral: Lunate should articulate with radius AND capitate
- •PA: Disrupted Gilula's arcs, triangular lunate
- •Spilled teacup = Stage IV lunate dislocation
- •25% missed on initial X-ray
Greater vs Lesser Arc
- •Lesser arc: Pure ligamentous (SL, LT)
- •Greater arc: Fractures through bones (trans-scaphoid most common)
- •Greater arc needs fracture fixation + ligament repair
Emergency Management
- •Assess median nerve - acute CTS is emergency
- •Closed reduction: TRAP (Traction, Recreate, Apply pressure, Push)
- •Closed reduction is temporizing only
- •All require definitive surgical treatment
Surgical Principles
- •Combined volar + dorsal approach preferred
- •CTR mandatory (even without acute CTS)
- •K-wire fixation: SL, SC, LT
- •Greater arc: Screw fixation of fractures + ligament repair