Keystone Carpal Bone | Risk of AVN | Kienbock's Disease Precursor
TEISEN CLASSIFICATION (5 TYPES)
Critical Must-Knows
- Lunate is keystone of proximal carpal row - central to wrist biomechanics
- Vulnerable blood supply - I-pattern lunates lack intraosseous redundancy (Gelberman)
- Kienbock's disease may follow acute fracture or develop insidiously
- Negative ulnar variance increases lunate loading and injury risk
- Body fractures (Type IV/V) have highest risk of AVN and nonunion
Clinical Pearls
- "Lunate fractures are rare but frequently missed on plain radiographs
- "MRI is essential for diagnosis and assessing vascularity
- "Negative ulnar variance is major risk factor for Kienbock's
- "Displaced body fractures require ORIF to prevent AVN
High-Yield Lunate Fracture Exam Points
The Keystone Bone
The lunate is the central link in the proximal carpal row, articulating with radius, scaphoid, triquetrum, capitate, and hamate. Its integrity is essential for normal wrist kinematics. Injury disrupts the entire wrist biomechanics.
Vascular Vulnerability
Gelberman described three intraosseous patterns (Y, I and X). The I-pattern lunate has a single dominant intraosseous vessel with minimal anastomosis, making it highly susceptible to avascular necrosis (AVN) when a body fracture crosses the central supply. Micro-CT work (van Alphen 2016) found around 14% of lunates have no dorsal nutrient vessel, creating volar-approach ischaemia risk.
Kienbock's Association
Acute lunate fracture can progress to Kienbock's disease (lunate AVN). However, most Kienbock's cases arise from repetitive microtrauma rather than acute fracture. Both share the common endpoint of lunate collapse and carpal arthritis.
Ulnar Variance Factor
Negative ulnar variance (short ulna) concentrates force on the lunate. This is a risk factor for both acute fracture and Kienbock's disease. Ulnar lengthening may be part of treatment in select cases.
At a Glance: Lunate Fracture Management
| Fracture Type | Location | Management | Key Consideration |
|---|---|---|---|
| Type I - Volar pole | Volar lip | Immobilization or screw | Associated with perilunate injury |
| Type II - Chip | Dorsal or volar | Immobilization, excision if needed | Usually good prognosis |
| Type III - Dorsal pole | Dorsal lip | Screw fixation or excision | Assess for scapholunate injury |
| Type IV - Sagittal | Through body | ORIF with headless screws | Moderate AVN risk |
| Type V - Transverse | Through body | ORIF critical | High AVN risk - needs early fixation |
LUNATE - KLUNATE - Key Fracture Features
| L | Location central Keystone of proximal carpal row |
| U | Ulnar variance matters Negative variance increases lunate load |
| N | Necrosis risk I-pattern (single dominant vessel) lacks redundancy - high AVN risk |
| A | Associated injuries Check for perilunate injury, SL damage |
| T | Teisen classification Types I-V based on fracture pattern |
| E | Early MRI essential Assess vascularity and occult fractures |
| L | Location central Keystone of proximal carpal row | N | Necrosis risk I-pattern (single dominant vessel) lacks redundancy - high AVN risk | T | Teisen classification Types I-V based on fracture pattern |
| U | Ulnar variance matters Negative variance increases lunate load | A | Associated injuries Check for perilunate injury, SL damage | E | Early MRI essential Assess vascularity and occult fractures |
Hook:LUNATE - the keystone bone with Necrosis risk requiring early Assessment
KIEN - KKIEN - Kienbock's Disease Features
| K | Keystone collapse Progressive lunate collapse and fragmentation |
| I | Insidious onset Often no acute injury - repetitive microtrauma |
| E | Early MRI changes Signal changes precede X-ray findings |
| N | Negative ulnar variance Major risk factor - increased lunate load |
| K | Keystone collapse Progressive lunate collapse and fragmentation | E | Early MRI changes Signal changes precede X-ray findings |
| I | Insidious onset Often no acute injury - repetitive microtrauma | N | Negative ulnar variance Major risk factor - increased lunate load |
Hook:KIEN-bock's develops Insidiously with Negative ulnar variance
BOCK - MBOCK - Management Algorithm
| B | Bone vascularity MRI to assess blood supply - critical for prognosis |
| O | Offload the lunate Radial shortening or ulnar lengthening |
| C | Core decompression For early disease - preserves bone structure |
| K | Kinematic fusion For advanced disease - limited intercarpal fusion |
| B | Bone vascularity MRI to assess blood supply - critical for prognosis | C | Core decompression For early disease - preserves bone structure |
| O | Offload the lunate Radial shortening or ulnar lengthening | K | Kinematic fusion For advanced disease - limited intercarpal fusion |
Hook:BOCK management: assess Bone vascularity, Offload, Core decompression, Kinematic fusion
Overview and Epidemiology
Definition
Lunate fractures are fractures of the lunate carpal bone, the central "keystone" of the proximal carpal row. These fractures range from minor avulsion injuries to complete body fractures with significant implications for wrist function.
Epidemiology
- Incidence: Under 3% of all carpal fractures (very rare)
- Age distribution: Typically young to middle-aged adults
- Gender: Male predominance in acute trauma
- Mechanism: High-energy axial loading or hyperextension
Relationship to Kienbock's Disease
Kienbock's disease (lunate avascular necrosis) may develop:
- Following acute lunate fracture
- From repetitive microtrauma without acute fracture
- Due to inherent vascular compromise
The relationship between acute fracture and Kienbock's is complex, with both potentially representing points on a spectrum of lunate injury.
Clinical Significance
The lunate occupies a critical position in the wrist:
- Transmits approximately one third of radio-ulno-carpal load through the radio-lunate joint (Schuind 1995)
- Central to proximal row kinematics
- Articulates with multiple carpal and forearm bones
- Injury affects entire wrist function
Understanding the lunate's central role is essential for appreciating the significance of these fractures.
Anatomy/Biomechanics
Osseous Anatomy
Shape and Configuration
- Crescent-shaped when viewed laterally (lunate = moon-shaped)
- Volar horn: Projects palmarly, attachment for radiocarpal ligaments
- Dorsal horn: Smaller, attachment for dorsal intercarpal ligament
- Proximal surface: Convex, articulates with lunate facet of radius
Articular Surfaces
- Proximal: Articulates with radius (70%) and TFCC (30%)
- Radial: Articulates with scaphoid
- Ulnar: Articulates with triquetrum
- Distal: Articulates with capitate and often hamate (Type II lunate)
Type I vs Type II Lunates
- Type I (35%): Single distal facet for capitate only
- Type II (65%): Two distal facets - capitate and hamate
- Type II may have altered biomechanics affecting injury patterns
Vascular Anatomy

Blood Supply Pattern
Gelberman's classic cadaveric study described three intraosseous patterns, with a dorsal-volar anastomosis present in every specimen:
Y-Pattern
- Dorsal and volar vessels meet in a robust intraosseous anastomosis
- Most redundant supply, more protected from AVN
X-Pattern
- Crossed dorsal and volar vessels with intermediate anastomosis
- Intermediate AVN risk
I-Pattern
- A single dominant intraosseous vessel with minimal anastomosis
- Least redundant supply, highest risk of AVN when a fracture crosses it
Vessel Entry Points
- Dorsal: 2-3 vessels feeding a dorsal capsular plexus, with 1-2 nutrient vessels entering the dorsal pole
- Volar: 3-4 vessels feeding a volar plexus, with 1-2 nutrient vessels entering the volar pole
- Micro-CT work (van Alphen 2016) found roughly 14% of lunates have no dorsal nutrient vessel
- No intraosseous penetration from radial or ulnar surfaces
Vascular Pattern Determines Prognosis
The I-pattern lunate, with a single dominant intraosseous vessel and minimal anastomosis, explains why body fractures (Type IV/V) carry such high AVN risk - the fracture line can isolate a major portion of the bone from its only supply. Pattern cannot be determined before surgery.
Biomechanics
Load Transmission
- The radio-lunate joint transmits approximately one third of radio-ulno-carpal load; the radio-scaphoid joint carries about 55% and the TFCC about 10% (Schuind 1995)
- Forces concentrated on the lunate when ulnar variance is negative
- Normal lunate tilts volarly 10-15 degrees
Carpal Kinematics
- Part of proximal row "intercalated segment"
- Moves with scaphoid and triquetrum as functional unit
- Disruption leads to carpal instability patterns (DISI/VISI)
Ulnar Variance Impact
- Negative variance: Increased lunate loading
- Positive variance: Load shared with TFCC
- Average: Neutral (0 +/- 1mm)
Understanding the anatomy explains why certain fracture patterns carry higher risks.
Classification Systems
Teisen Classification
The Teisen classification is the most widely used system for acute lunate fractures:
Type I - Volar Pole Fracture
- Avulsion of volar horn by short radiolunate ligament
- Often associated with perilunate injury pattern
- Usually small fragment - may not require fixation
- Treatment: Immobilization if undisplaced, surgery if part of perilunate
Type II - Chip Fracture
- Small dorsal or volar avulsion fragment
- Usually minimal clinical significance
- Most common acute lunate fracture pattern
- Treatment: Cast immobilization, excision if persistently symptomatic
Type III - Dorsal Pole Fracture
- Larger dorsal horn fragment
- May involve scapholunate ligament attachment
- Risk of dorsal intercalated segment instability
- Treatment: Screw fixation if large, excision if small
Type IV - Sagittal Body Fracture
- Sagittal split through lunate body
- Moderate risk of AVN
- Disrupts articular surfaces
- Treatment: ORIF with headless compression screws
Type V - Transverse Body Fracture
- Coronal/transverse split through body
- Highest AVN risk (disrupts dominant vessel)
- Poor prognosis without treatment
- Treatment: Urgent ORIF, close monitoring for AVN
This classification guides prognosis and treatment selection.

Classification Comparison
| Teisen Type | Location | AVN Risk | Typical Treatment |
|---|---|---|---|
| Type I | Volar pole | Low | Immobilization or ligament repair |
| Type II | Chip/avulsion | Very low | Cast, excision if symptomatic |
| Type III | Dorsal pole | Low-moderate | Screw fixation or excision |
| Type IV | Sagittal body | Moderate-high | ORIF with screws |
| Type V | Transverse body | High | Urgent ORIF |
Classification guides treatment urgency and prognosis discussion.
Clinical Assessment
History
Mechanism of Injury
- High-energy fall: FOOSH with axial loading
- Direct trauma: Rare due to protected position
- Sports injury: Gymnastics, contact sports
- Insidious onset: May indicate developing Kienbock's rather than acute fracture
Key History Points
- Exact mechanism and energy of injury
- Prior wrist symptoms (may indicate pre-existing Kienbock's)
- Occupational demands (manual labor, vibration exposure)
- Hand dominance
- Duration of symptoms
Physical Examination
Inspection
- Swelling may be subtle due to deep location
- No obvious deformity unless associated carpal injury
- Compare to contralateral wrist
Palpation
- Lunate fossa tenderness: Palpate with wrist slightly flexed
- Dorsal lunate: Tender with wrist extended
- May be difficult to localize with surrounding swelling
Range of Motion
- Limited wrist flexion and extension
- Pain with forearm rotation
- Grip weakness
Neurovascular Assessment
- Usually preserved
- Check median nerve (carpal tunnel with swelling)
- Document baseline for comparison
Special Tests
Watson Test (Scaphoid Shift)
- Assess for associated scapholunate injury
- Often positive with perilunate pattern injuries
Ballottement Test
- Lunotriquetral stability
- Assess for associated LT injury
Grind Test
- Axial load with rotation
- Positive if pain reproduced
Carpal Tunnel Assessment
- Phalen's and Tinel's tests
- May be positive with acute swelling
Clinical examination is often non-specific; imaging is essential for diagnosis.
Differential Diagnosis
Dorsal central wrist pain after a fall has a wide differential. The lunate fracture must be distinguished from injuries with overlapping tenderness and from chronic lunate pathology.
Differential Diagnosis of Central Dorsal Wrist Pain
| Diagnosis | Key Distinguishing Feature | Best Discriminating Investigation |
|---|---|---|
| Lunate fracture | Lunate fossa tenderness; subtle or absent fracture line on X-ray | MRI (occult fracture, viability) or CT |
| Kienbock's disease (lunate AVN) | Insidious onset, no clear acute injury; lunate sclerosis/collapse | MRI - low T1 signal; X-ray for staging |
| Scaphoid fracture | Anatomical snuffbox and scaphoid tubercle tenderness | Scaphoid-series X-ray; MRI if occult |
| Perilunate / lunate dislocation | Deranged carpal arcs; 'spilled teacup' or 'piece-of-pie' sign on lateral | PA and lateral X-ray; CT for fractures |
| Scapholunate ligament injury | Positive Watson scaphoid-shift test; SL gap on clenched-fist view | Stress X-ray; MRI/arthroscopy |
| Distal radius fracture | Dorsal metaphyseal tenderness and deformity | PA and lateral X-ray |
| Wrist sprain / occult bone bruise | Diffuse tenderness, normal X-ray, settles with time | MRI if persistent |
Investigations
Plain Radiographs

Standard Views
- PA view: May show fracture line, sclerosis, or collapse
- Lateral view: Assess lunate position (DISI/VISI), dorsal fractures
- Scaphoid view: Additional perspective on carpal relationships
Radiographic Signs of Acute Fracture
- Fracture line (often subtle or absent)
- Slight density change
- Associated carpal malalignment
Signs of Kienbock's Disease
- Increased lunate density (sclerosis)
- Loss of carpal height
- Lunate collapse and fragmentation
- Secondary arthritis (late)
Ulnar Variance Measurement
- Measure on neutral rotation PA view
- Negative variance (short ulna) is risk factor
- Compare to contralateral if available
CT Scanning
Indications
- Characterize fracture pattern for surgical planning
- Assess for occult fracture not seen on X-ray
- Evaluate associated carpal injuries
Key CT Findings
- Fracture line orientation (sagittal vs transverse)
- Fragment size and displacement
- Articular surface involvement
- Comminution assessment
MRI
Critical Role in Lunate Pathology
MRI is essential for:
- Detecting occult fractures missed on X-ray
- Assessing lunate vascularity
- Differentiating acute fracture from Kienbock's
- Evaluating ligamentous injuries
Signal Changes
- Normal lunate: Isointense to other carpal bones
- Early ischemia: Decreased T1 signal
- Established AVN: Low T1 and T2 signal
- Revascularization: Mixed signals
Gadolinium Enhancement
- Enhanced signal suggests preserved vascularity
- Absence of enhancement indicates AVN
- Helps predict prognosis
Bone Scan
Limited Role
- Sensitive but not specific
- Hot lunate in any pathology
- Superseded by MRI for most indications
Investigations are summarized in the table below.
Imaging Modalities for Lunate Fractures
| Modality | Primary Role | Advantages | Limitations |
|---|---|---|---|
| Plain X-ray | Initial screening | Available, low cost | Misses early/occult fractures |
| CT scan | Fracture characterization | Bone detail, 3D planning | No vascularity assessment |
| MRI | Vascularity, occult injury | Soft tissue, blood supply | Cost, availability |
| Bone scan | Rarely needed | Sensitive for pathology | Non-specific |
MRI is the key investigation for determining treatment and prognosis.
Management Algorithm
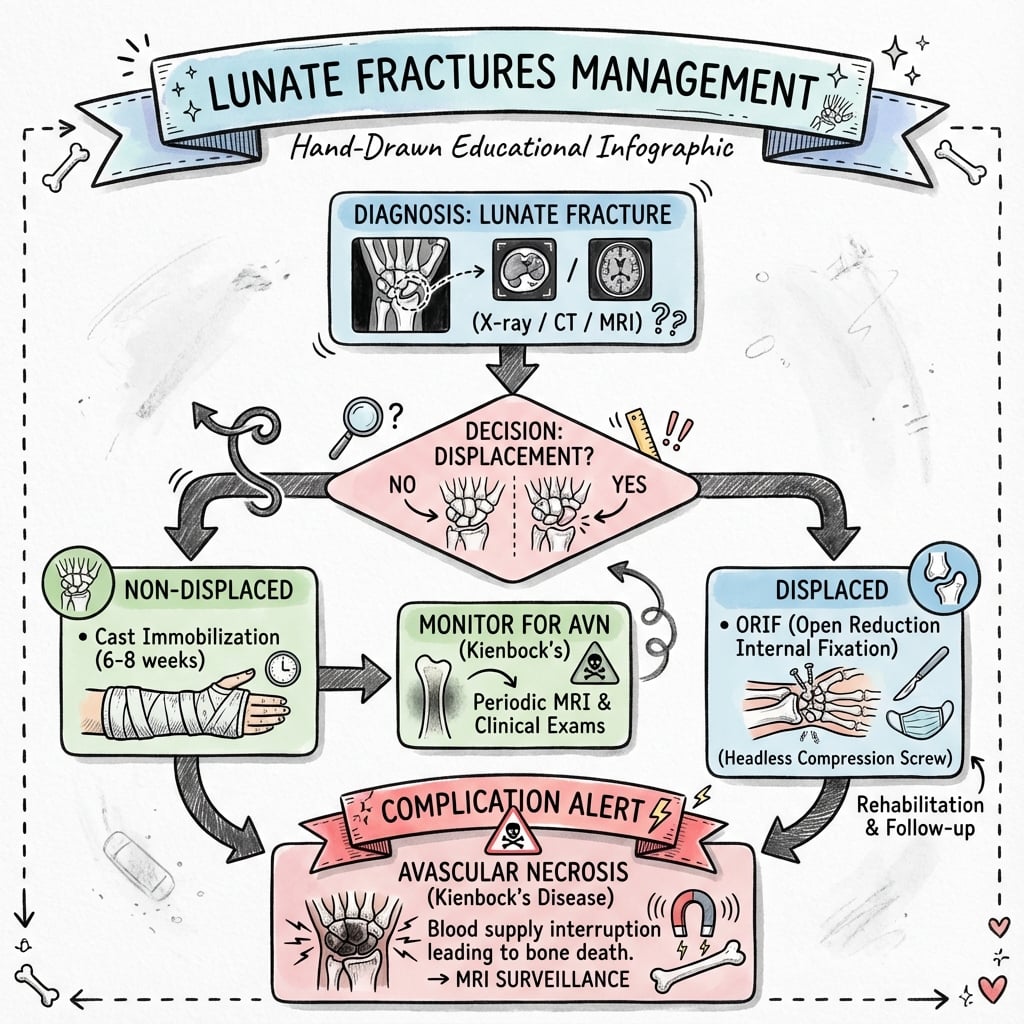
Non-Operative Management
Indications
- Type I (volar pole) - undisplaced
- Type II (chip fractures) - most cases
- Type III (dorsal pole) - small, undisplaced fragments
- Elderly, low-demand patients with body fractures
Protocol
Immobilization
- Short arm cast or splint
- Wrist in neutral position
- Include thumb if scaphoid concern
- Duration: 6-8 weeks minimum
Follow-Up
- Week 2: Clinical review, check cast
- Week 6: Repeat radiographs
- Week 8-12: MRI if symptoms persist
- Monitor for AVN development (may take months)
Transition to Rehabilitation
- Begin ROM when clinically healed
- Progressive strengthening
- Monitor for late complications
Expected Outcomes
- Type II fractures: Excellent prognosis
- Type I/III: Good with proper immobilization
- Body fractures: Higher failure rate with non-operative treatment
Non-operative management requires vigilant monitoring for AVN.
Management decisions must consider the high risk of AVN with body fractures.
Surgical Technique
Dorsal Approach for Lunate Fracture ORIF
Patient Positioning
- Supine with arm table
- Tourniquet on upper arm
- Consider traction tower for visualization
Incision and Exposure
Skin Incision
- Dorsal longitudinal over wrist
- Centered on Lister's tubercle
- 4-5 cm length
Deep Dissection
- Incise retinaculum between 3rd and 4th compartments
- Protect EPL tendon (retract radially)
- Retract EDC ulnarly
- Capsulotomy - ligament-sparing technique preferred
Fracture Reduction
Visualization
- Flex wrist to expose lunate dorsum
- Identify fracture pattern
- Assess vascularity (bleeding from bone)
Reduction Technique
- Gentle manipulation of fragments
- Provisional K-wire fixation
- Confirm reduction with fluoroscopy
- Assess articular surface congruity
Fixation
Headless Compression Screw
- Select appropriate screw size (2.0-2.4mm)
- Start at dorsal cortex
- Aim for volar cortex (or far fragment)
- Countersink beneath cartilage
- Confirm position on multiple fluoroscopy views
Supplemental Fixation
- K-wire for rotational control if needed
- Second screw for large body fractures
Closure
- Repair capsule meticulously
- Close retinaculum loosely
- Standard skin closure
- Splint in neutral position
Gentle handling throughout preserves the tenuous blood supply.
Surgical technique must minimize further vascular compromise.
Complications
Intraoperative Complications
Iatrogenic Fracture
- Lunate is small and fragile
- Risk during screw insertion
- Prevention: Careful technique, appropriate implant size
- Management: Additional fixation if occurs
Screw Malposition
- Joint penetration causes arthritis
- Prevention: Multiple fluoroscopy views
- Management: Revise if intra-articular
Vascular Injury
- Further compromise to tenuous blood supply
- Prevention: Minimize soft tissue stripping
- Cannot be assessed intraoperatively
Early Complications
Wound Complications
- Infection: Unusual but problematic for this small bone
- Dehiscence: May expose hardware
- Management: IV antibiotics, debridement if deep
Hardware Problems
- Screw prominence: May irritate extensor tendons
- K-wire migration: Remove early
- Management: Hardware removal once healed
Carpal Tunnel Syndrome
- May develop with swelling
- Treatment: Splinting, elevation, decompression if persistent
Late Complications
Avascular Necrosis (Most Critical)
- High risk after displaced body fractures (Type IV/V) that cross the central supply; small case series rather than large cohorts inform exact rates
- May present months after injury
- Progressive pain, decreased motion
- Treatment depends on stage and viability (see Kienbock's management)
Nonunion
- More common with body fractures
- Related to AVN in many cases
- Treatment: Bone grafting, revision fixation
Post-Traumatic Arthritis
- Consequence of AVN or articular malreduction
- Progressive wrist pain and stiffness
- Treatment: Activity modification to fusion
Carpal Instability
- DISI or VISI pattern may develop
- Related to associated ligament injury
- May require carpal fusion
Complication Management Summary
| Complication | Risk Factors | Prevention | Management |
|---|---|---|---|
| AVN | Displaced body fractures, I-pattern supply | Early fixation, gentle technique | Stage/viability-dependent: unloading to salvage |
| Nonunion | AVN, inadequate fixation | Stable fixation, bone graft | Revision fixation, vascularized graft |
| Arthritis | Malreduction, AVN | Anatomic reduction | Arthrodesis options |
| Hardware problems | Prominent implants | Countersink screws | Hardware removal |
AVN is the dominant concern in lunate fracture management.
Postoperative Care
Immediate Postoperative Care (0-2 Weeks)
Immobilization
- Splint in neutral wrist position
- Allow immediate finger motion
- Maintain elevation
Pain Management
- Multimodal analgesia
- Ice application
- Elevate extremity
Monitoring
- Watch for signs of infection
- Neurovascular checks
- Swelling assessment
Wound Care
Dressing Changes
- First change at 48-72 hours
- Assess wound healing
- K-wire site cleaning if applicable
Suture Removal
- 10-14 days postoperatively
- Apply steri-strips for support
Rehabilitation Phases
Phase 1: Protection (Weeks 0-2)
- Active finger motion
- Shoulder and elbow ROM
- Edema control with elevation and compression
Phase 2: Early Motion (Weeks 2-6)
- Begin gentle wrist ROM
- Removable splint between exercises
- Continue edema management
- Hand therapy referral
Phase 3: Progressive Loading (Weeks 6-12)
- Progress to functional activities
- Light grip strengthening
- Discontinue splint (usually at week 6)
- Normal ADLs
Phase 4: Return to Function (Weeks 12+)
- Progressive strengthening
- Sport-specific activities
- Work conditioning
- Full recovery may take 6-12 months
Follow-Up Schedule
| Timepoint | Assessment | Imaging |
|---|---|---|
| Week 2 | Wound check | Optional |
| Week 6 | ROM, healing | Radiographs |
| Week 12 | Function | Radiographs |
| Month 6 | AVN surveillance | MRI recommended |
| Year 1 | Long-term outcome | As needed |
| Year 2 | Final review | If symptomatic |
MRI surveillance for AVN is critical, especially for body fractures.
Outcomes and Prognosis
Functional Outcomes by Fracture Type
Type I-III (Pole/Chip Fractures)
- Generally good to excellent outcomes
- Full ROM recovery expected
- Return to previous activities typical
- Low AVN risk
Type IV (Sagittal Body)
- Moderate outcomes
- Some motion loss common
- Moderate-to-high AVN risk
- May require secondary procedures
Type V (Transverse Body)
- Most guarded prognosis
- Highest AVN risk of the Teisen types
- Significant motion loss common
- Often progresses to Kienbock's
Prognostic Factors
Favorable Factors
- Pole or chip fractures
- Undisplaced pattern
- Early diagnosis and treatment
- MRI showing preserved vascularity
- Neutral or positive ulnar variance
Unfavorable Factors
- Body fractures (Type IV/V)
- Delayed diagnosis
- Associated carpal injuries
- MRI showing avascularity
- Negative ulnar variance
Natural History of Untreated Fractures
Chip Fractures
- May remain asymptomatic
- Occasional persistent pain
- Rarely progress to AVN
Body Fractures
- High rate of nonunion
- Progressive AVN development
- Eventual carpal collapse
- Secondary arthritis
Long-Term Outcomes
Without AVN
- Good grip strength recovery (80-90% of contralateral)
- Near-normal ROM
- Return to previous occupation and sport
With AVN (Kienbock's Development)
- Progressive deterioration
- May require salvage procedures
- Outcomes depend on stage at intervention:
- Stage I-II: Core decompression or revascularization may preserve function
- Stage IIIA: Motion-preserving procedures possible
- Stage IIIB-IV: Limited wrist fusion or arthroplasty
Prognosis is largely determined by development or avoidance of AVN.
Evidence Base
- 35 cadaver lunates injected and cleared; extraosseous supply via 2-3 dorsal and 3-4 volar vessels
- Intraosseous supply formed three consistent patterns (Y, I and X) with a dorsal-volar anastomosis in every specimen
- The I-pattern (single dominant intraosseous vessel with minimal anastomosis) is the least redundant and most vulnerable
- Findings support a compression-fracture theory for Kienbock's disease
- Radiographs of 17 patients with acute lunate fractures reviewed with long-term follow-up
- Proposed the five-group classification (volar pole, chip, dorsal pole, sagittal body, transverse body)
- Fractures classified by radiological appearance and by lunate vascular anatomy
- Body fractures crossing the nutrient supply carry the worst prognosis
- Updated algorithm integrating the osseous (Lichtman) stage with perfusion (Schmitt) and cartilage (Bain) classifications
- Early intact-lunate disease is protected non-operatively, then unloaded if it fails
- Compromised lunate reconstructed with medial femoral condyle graft or proximal row carpectomy
- Advanced collapse (KALC) managed by salvage procedures only
- Rigid-body spring model; intact radio-lunate joint carried a mean 32% of total radio-ulno-carpal load
- A 4 mm radial shortening or ulnar lengthening reduced radio-lunate load by 45%
- Limited intercarpal fusions reduced radio-lunate load by no more than 15%
- Capitate shortening unloaded the lunate but dangerously overloaded adjacent joints
- Force transmission at the radio-ulno-carpal joint was 55% radio-scaphoid, 35% radio-lunate and 10% through the TFCC
- Peak pressure was highest at the proximal radio-scaphoid pole
- Ligaments resisting ulnar translation were most important for load transfer
- Wrist morphology and age had little effect on load distribution
- 65 surgically treated perilunate injuries; 62 of 65 displaced dorsally
- Lunate osteonecrosis occurred in 7.7% and wrist arthritis in 58.5% at a mean 8-year follow-up
- Secondary surgery was required in 26% of cases
- Osteochondral lesions and a changed scapholunate angle predicted later osteoarthritis
The evidence supports joint-levelling for lunate unloading, anatomic fixation of body and perilunate injuries, and long-term avascular necrosis surveillance.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Acute Lunate Fracture Evaluation
"A 28-year-old manual laborer presents 2 days after a fall from scaffolding. He has wrist pain, and X-rays show a possible lunate abnormality. How do you evaluate this injury?"
Lunate Fracture with AVN Risk
"CT and MRI confirm a Type V transverse lunate body fracture in a 35-year-old office worker. MRI shows intact signal on T1 sequences. How do you counsel this patient and plan treatment?"
Kienbock's Disease Management
"A patient you treated for a lunate fracture 18 months ago returns with progressive wrist pain. MRI shows Stage IIIA Kienbock's disease. How do you manage this complication?"
MCQ Practice Points
Vascular Anatomy
Q: What are the three intraosseous vascular patterns of the lunate, and which carries the highest AVN risk? A: Gelberman described the Y, X and I patterns. The I-pattern has a single dominant intraosseous vessel with minimal anastomosis and the least redundancy, so it carries the highest avascular necrosis risk when a body fracture crosses the central supply.
AVN Risk by Fracture Type
Q: Which Teisen classification type has the highest risk of avascular necrosis? A: Type V (transverse body) fractures carry the highest AVN risk because the transverse fracture line crosses and can isolate the dominant intraosseous vessel from a large part of the bone. Type IV (sagittal body) is the next highest; pole and chip fractures rarely develop AVN.
Ulnar Variance Association
Q: What ulnar variance pattern is associated with increased lunate fracture and Kienbock's disease risk? A: Negative ulnar variance (short ulna relative to radius) concentrates axial load on the lunate. This is a major risk factor for both acute fracture and progressive AVN.
Keystone Position
Q: How is axial wrist load shared at the radio-ulno-carpal joint? A: Schuind's biomechanical model found roughly 55% passes through the radio-scaphoid joint, about 35% (around one third) through the radio-lunate joint, and about 10% through the TFCC. The lunate is still the central "keystone" of the proximal carpal row, and negative ulnar variance shifts more load onto it.
MRI Findings
Q: What MRI finding indicates early avascular necrosis of the lunate? A: Decreased T1 signal relative to other carpal bones indicates early AVN, as fat in the bone marrow is replaced by edema or necrotic tissue. T2 signal may be variable depending on the stage.
Kienbock's Staging
Q: What distinguishes Stage IIIA from Stage IIIB Kienbock's disease? A: Stage IIIA has lunate collapse but maintained carpal height and no fixed scaphoid rotation. Stage IIIB shows scaphoid rotation (ring sign on X-ray) and proximal capitate migration, indicating more advanced carpal collapse.
Understanding these key concepts will help with exam success.
Guidelines, Registries & Global Practice
Global Epidemiology
Isolated lunate fractures are rare, reported as under 3% of carpal fractures, and acute lunate injury most often occurs within a high-energy perilunate pattern. In a 65-case European perilunate series, 62 of 65 injuries displaced dorsally, lunate osteonecrosis occurred in 7.7% and post-traumatic arthritis in 58.5% at a mean 8-year follow-up (Israel 2016). Kienbock's disease, the related lunate avascular necrosis, classically affects manual workers aged 20-40 and is associated with negative ulnar variance.
Guidance & Consensus on Lunate Injury and Kienbock's Disease
| Body / Source | Position | Evidence Level |
|---|---|---|
| AO Foundation (Surgery Reference) | Acute displaced body fractures and perilunate injuries treated by anatomic reduction and stable fixation; preserve dorsal/volar blood supply | Expert consensus / Level V |
| BSSH / EFORT hand consensus | MRI is the key investigation for occult fracture and lunate viability; isolated chip/pole fractures usually non-operative | Level IV-V |
| Lichtman algorithm (AAOS/JWS) | Stage- and viability-based pathway: protect intact lunate, unload, reconstruct, then salvage | Level V review |
| Biomechanical evidence (Horii 1990) | Radial shortening / ulnar lengthening preferred for unloading - 45% radio-lunate load reduction | Level V model |
Practice Variation
- Diagnosis: high-resource settings use early MRI and CT routinely; in limited-resource settings diagnosis relies on radiographs and clinical follow-up, raising the rate of missed occult fractures.
- Kienbock's unloading: radial shortening osteotomy is the most widely adopted joint-levelling procedure internationally because it is technically reliable and avoids a separate graft site; ulnar lengthening is used less often.
- Reconstruction: vascularised bone grafting (including medial femoral condyle flaps) for the compromised but reconstructable lunate is concentrated in specialist hand-surgery and microsurgery centres.
- Registries: there is no dedicated carpal-fracture joint registry (the major arthroplasty registries such as the NJR, AJRR and AOANJRR do not capture lunate fracture or Kienbock's outcomes), so evidence rests on case series and biomechanical studies rather than registry data.
Rehabilitation through specialist hand therapy and long-term avascular-necrosis surveillance with delayed MRI are recommended internationally after body fractures and perilunate injuries.
Lunate Fractures - Rapid Recall
Clinical summary
Definition & Key Concepts
- •Keystone of proximal carpal row
- •Under 3% of all carpal fractures
- •I-pattern lunate lacks intraosseous anastomosis (Gelberman)
- •About one third of radio-ulno-carpal load via radio-lunate joint
- •Negative ulnar variance increases risk
Teisen Classification
- •Type I: Volar pole fracture
- •Type II: Chip fracture (dorsal/volar)
- •Type III: Dorsal pole fracture
- •Type IV: Sagittal body fracture
- •Type V: Transverse body - highest AVN risk
Imaging Strategy
- •X-ray: May miss fracture, assess ulnar variance
- •CT: Characterize fracture pattern
- •MRI: Essential for vascularity assessment
- •Decreased T1 signal = early AVN
Treatment Algorithm
- •Type I-III: Often non-operative (cast 6-8 weeks)
- •Type IV/V: ORIF with headless screws
- •Dorsal approach for most fractures
- •Gentle technique to preserve blood supply
AVN & Kienbock's Management
- •Stage I-II: Core decompression, revascularization
- •Stage IIIA: Radial shortening, limited fusion
- •Stage IIIB: PRC or limited fusion
- •Stage IV: Salvage fusion or arthroplasty
Complications & Outcomes
- •AVN: highest with Type V transverse body fractures
- •Nonunion: Related to AVN in many cases
- •Long-term MRI surveillance essential
- •Prognosis depends on AVN development