LTIL Injury | VISI Deformity | LT Arthrodesis
INSTABILITY PATTERNS
Critical Must-Knows
- LTIL (Lunotriquetral Interosseous Ligament) injury causes ulnar wrist pain and VISI (Volar Intercalated Segment Instability) deformity
- VISI deformity: Lunate flexes volarly, triquetrum extends dorsally - opposite of DISI (scapholunate)
- LT arthrodesis is gold standard for chronic instability - high union rate (85-90%), minimal motion loss (LT contributes little to wrist motion)
- LT ballottement test (Reagan's test) is key clinical test - stabilise lunate, translate triquetrum dorsally/palmarly
- Acute injuries: Direct repair with suture anchors if less than 6 weeks, better outcomes than chronic
Clinical Pearls
- "VISI = Volar Intercalated Segment Instability - lunate flexes volarly (opposite of DISI from SL injury)
- "LT arthrodesis preferred over reconstruction - high union rate, minimal motion loss, reliable pain relief
- "LT contributes less than 5% to wrist motion - fusion well-tolerated functionally
- "LT ballottement test: stabilise lunate, translate triquetrum - pain/crepitus = positive
Critical Lunotriquetral Instability Exam Points
VISI Deformity
VISI (Volar Intercalated Segment Instability) = lunate flexes volarly, triquetrum extends dorsally. Opposite of DISI (scapholunate injury). Lateral X-ray shows lunate tilted volarly (less than 0 degrees capitolunate angle).
LT Arthrodesis Gold Standard
LT arthrodesis is treatment of choice for chronic instability - High union rate (85-90%), minimal motion loss (LT contributes less than 5% to wrist motion), reliable pain relief. Preferred over ligament reconstruction.
LT Ballottement Test
Reagan's test (LT ballottement): Stabilise lunate with one hand, translate triquetrum dorsally and palmarly with other. Positive = pain, crepitus, or increased motion. Compare to contralateral side.
Acute vs Chronic
Acute injuries (less than 6 weeks): Direct repair with suture anchors - better outcomes than chronic. Chronic injuries: LT arthrodesis preferred - reconstruction less predictable.
Lunotriquetral Instability - Quick Decision Guide
| Pattern | Clinical Features | Treatment | Outcome |
|---|---|---|---|
| Dynamic | Pain, clicking, no deformity | LT repair or reconstruction | 70-80% good results |
| Static VISI | Fixed VISI deformity | LT arthrodesis | 85-90% good results |
| With arthritis | LT joint arthritis | LT fusion or salvage | 80-85% good results |
VDVISI vs DISI
| V | VISI Volar Intercalated - Lunate flexes VOLARLY (LT injury) |
| D | DISI Dorsal Intercalated - Lunate extends DORSALLY (SL injury) |
| V | VISI Volar Intercalated - Lunate flexes VOLARLY (LT injury) |
| D | DISI Dorsal Intercalated - Lunate extends DORSALLY (SL injury) |
Hook:VD: VISI = Volar (LT injury), DISI = Dorsal (SL injury)!
VISILT Instability Features
| V | Volar Lunate tilts volarly |
| I | Intercalated Intercalated segment instability |
| S | Segment Lunate is intercalated segment |
| I | Instability LTIL injury causes instability |
| V | Volar Lunate tilts volarly | S | Segment Lunate is intercalated segment |
| I | Intercalated Intercalated segment instability | I | Instability LTIL injury causes instability |
Hook:VISI: Volar Intercalated Segment Instability - lunate flexes volarly!
HIGHLT Arthrodesis Advantages
| H | High union 85-90% union rate |
| I | Insignificant motion loss LT contributes less than 5% |
| G | Gold standard Treatment of choice for chronic |
| H | High success Reliable pain relief |
| H | High union 85-90% union rate | G | Gold standard Treatment of choice for chronic |
| I | Insignificant motion loss LT contributes less than 5% | H | High success Reliable pain relief |
Hook:HIGH: High union, Insignificant motion loss, Gold standard, High success!
Overview and Epidemiology
Lunotriquetral instability results from injury to the lunotriquetral interosseous ligament (LTIL), causing ulnar wrist pain and VISI (Volar Intercalated Segment Instability) deformity. Treatment depends on acuity and severity, with LT arthrodesis being the gold standard for chronic instability.
Definition
Lunotriquetral instability: Loss of stability between lunate and triquetrum due to LTIL injury, causing:
- Ulnar wrist pain: Pain on ulnar side of wrist
- VISI deformity: Lunate flexes volarly, triquetrum extends dorsally
- Functional impairment: Weakness, clicking, instability
LTIL (Lunotriquetral Interosseous Ligament):
- Connects lunate and triquetrum
- Stabilises ulnar carpus
- Injury causes VISI deformity
Epidemiology
- Incidence: 5-10% of carpal ligament injuries
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: Fall on outstretched hand with ulnar deviation, or direct trauma
- Associated injuries: Perilunate dislocations, other carpal injuries
VISI vs DISI
VISI (Volar Intercalated Segment Instability) = lunate flexes volarly (LT injury). DISI (Dorsal Intercalated Segment Instability) = lunate extends dorsally (SL injury). Remember: VISI = Volar (LT), DISI = Dorsal (SL).
Anatomy and Pathophysiology
LTIL Anatomy
Lunotriquetral Interosseous Ligament (LTIL):
- Location: Between lunate and triquetrum
- Structure: Dorsal, volar, and interosseous components
- Function: Stabilises ulnar carpus, prevents VISI deformity
- Blood supply: Dorsal and volar carpal arches
Carpal kinematics:
- Proximal row: Scaphoid, lunate, triquetrum move together
- LT joint: Contributes less than 5% to wrist motion
- VISI: Lunate flexes volarly when LTIL disrupted
Pathophysiology
Injury mechanism:
- Fall on outstretched hand: With ulnar deviation
- Direct trauma: To ulnar side of wrist
- Perilunate dislocation: Often associated with LTIL injury
VISI deformity:
- Lunate: Flexes volarly (opposite of DISI)
- Triquetrum: Extends dorsally
- Capitolunate angle: Less than 0 degrees (normal 0-15 degrees)
- Scapholunate angle: Normal (SL intact)
Why VISI occurs:
- LTIL disruption: Loss of stabilisation between lunate and triquetrum
- Lunate unopposed: Flexes volarly (volar ligaments intact)
- Triquetrum: Extends dorsally (dorsal ligaments intact)
Classification Systems
Severity-Based Classification
Dynamic instability:
- Pain, clicking, no fixed deformity
- LTIL partially torn
- Treatment: LT repair or reconstruction
Static VISI:
- Fixed VISI deformity on X-ray
- LTIL completely torn
- Treatment: LT arthrodesis (preferred)
With arthritis:
- LT joint arthritis present
- Chronic instability
- Treatment: LT fusion or salvage procedures
Severity guides treatment approach.
Clinical Assessment
History
Symptoms:
- Ulnar wrist pain: Pain on ulnar side of wrist
- Clicking or clunking: With wrist movement
- Weakness: Grip strength reduced
- Instability: Feeling of wrist giving way
Mechanism:
- Fall on outstretched hand with ulnar deviation
- Direct trauma to ulnar side of wrist
- High-energy trauma (perilunate dislocation)
Physical Examination
Inspection:
- Swelling on ulnar side of wrist
- VISI deformity (if static)
- Prominence of ulnar head (if VISI)
Palpation:
- LT interval tenderness (ulnar to lunate)
- Ulnar wrist pain
- Crepitus at LT joint
Range of Motion:
- Wrist ROM may be limited
- Pain with ulnar deviation
- Clicking with motion
Special Tests
LT Ballottement Test (Reagan's Test):
- Stabilise lunate with one hand
- Translate triquetrum dorsally and palmarly with other hand
- Positive: Pain, crepitus, or increased motion
- Compare to contralateral side
LT Compression Test:
- Ulnar deviation of wrist
- Apply axial load through ring/small finger metacarpals
- Positive: Pain at LT interval
Ulnar Snuffbox Test:
- Palpate ulnar snuffbox (between triquetrum and ulnar styloid)
- Positive: Tenderness indicates LT injury
Clinical Examination Key Point
LT ballottement test (Reagan's test) is the key clinical test - Stabilise lunate, translate triquetrum dorsally and palmarly. Positive = pain, crepitus, or increased motion. Compare to contralateral side.
Investigations
Standard X-ray Protocol
PA view:
- Assess LT interval (may be widened)
- Carpal height (may be reduced in VISI)
- Ulnar variance
Lateral view (critical):
- VISI deformity: Lunate flexed volarly
- Capitolunate angle: Less than 0 degrees (normal 0-15 degrees)
- Scapholunate angle: Normal (SL intact)
- Lunate position: Volar tilt
Clenched fist view:
- May show dynamic instability
- LT interval widening
Lateral X-ray is essential for VISI diagnosis.
Imaging Gallery
Diagnostic Imaging for LT Instability


Management Algorithm
Management Pathway
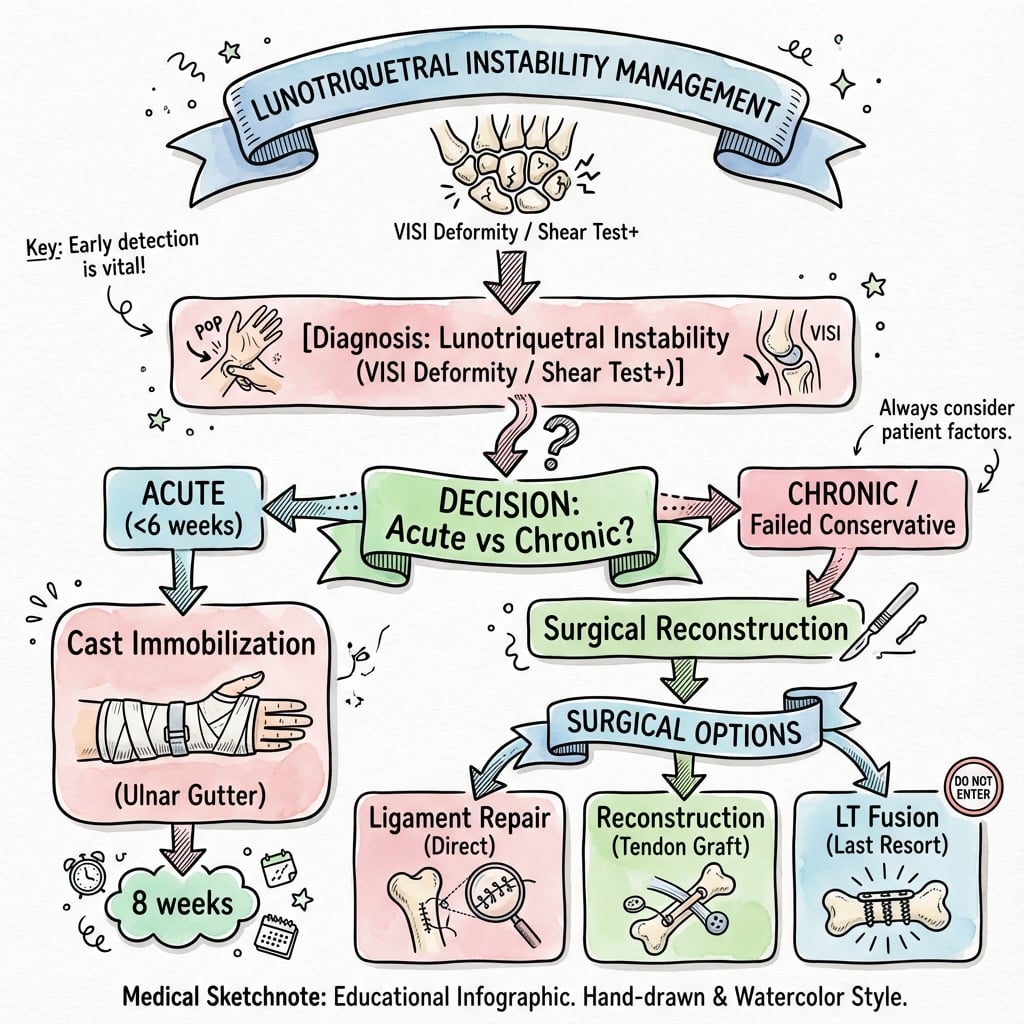
Lunotriquetral Instability Management
Clinical examination (LT ballottement test), lateral X-ray (VISI deformity), classify as dynamic or static, acute or chronic.
If acute (less than 6 weeks), direct repair with suture anchors via dorsal or palmar approach. Better outcomes than chronic repair. Success rate 70-80%.
If chronic (over 6 weeks) or static VISI, LT arthrodesis is gold standard. High union rate (85-90%), minimal motion loss (LT contributes less than 5%), reliable pain relief. Success rate 85-90%.
If LT joint arthritis present, LT fusion addresses instability and pain. If severe arthritis or failed fusion, consider salvage procedures (PRC, wrist fusion). Success rate 80-85%.
Surgical Technique
LT Arthrodesis Technique (Gold Standard)
Indications:
- Chronic LT instability (over 6 weeks)
- Static VISI deformity
- Failed repair or reconstruction
Approach:
- Dorsal ulnar incision between 4th and 5th extensor compartments
- Identify and protect DRUJ and ECU tendon
- Expose LT joint through dorsal capsulotomy
Technique:
- Exposure: Dorsal approach, expose LT joint
- Preparation: Remove articular cartilage from lunate and triquetrum using curettes or burr
- Graft: Pack autograft or allograft bone graft
- Fixation: Compression screw (headless cannulated) or plate/screws
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- High union rate (85-90%)
- Minimal motion loss (LT contributes less than 5%)
- Reliable pain relief
- Predictable outcomes
LT arthrodesis is gold standard for chronic instability.
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Nonunion | 10-15% | Smoking, poor fixation, inadequate graft | Rigid fixation, bone graft, smoking cessation |
| Persistent pain | 10-15% | Incomplete fusion, arthritis | Complete cartilage removal, adequate graft |
| Hardware issues | 5-10% | Prominent screws | Countersink screws, remove if symptomatic |
| Loss of correction | 5-10% | Inadequate fixation | Rigid fixation, compression |
Nonunion
10-15% incidence:
- Cause: Inadequate graft, poor fixation, smoking
- Prevention: Rigid fixation, bone graft, smoking cessation
- Management: Revision fusion with bone graft
Persistent Pain
10-15% incidence:
- Cause: Incomplete fusion, arthritis, other pathology
- Prevention: Complete cartilage removal, adequate graft
- Management: Assess for other causes, consider revision
Postoperative Care
Immediate Postoperative
- Immobilisation: Short arm cast (6-8 weeks)
- Weight bearing: Non-weight bearing on hand
- ROM: Finger ROM immediately
- PT: Wrist ROM after cast removal
Rehabilitation Protocol
Weeks 0-6:
- Short arm cast
- Finger ROM exercises
- Elevation to reduce swelling
Weeks 6-8:
- Cast removal
- Begin wrist ROM exercises
- Progressive strengthening
Weeks 8-12:
- Full ROM
- Progressive activity
- Return to sport/activity
Union and Hardware Removal
Union timeline: Typically 8-12 weeks postoperatively.
Hardware removal: Consider if prominent or symptomatic, usually after union confirmed (3-6 months).
Outcomes and Prognosis
Overall Outcomes
LT arthrodesis:
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Motion loss: Minimal (LT contributes less than 5% to wrist motion)
Direct repair (acute):
- Success rate: 70-80% (if acute, less than 6 weeks)
- Functional outcomes: 70-75% return to pre-injury level
- Motion: Full motion preserved
Functional Outcomes
Return to activity:
- Timeline: 3-6 months postoperatively
- Rate: 80-85% return to pre-injury level
- Factors: Treatment method, timing, rehabilitation compliance
Pain relief:
- LT arthrodesis: 85-90% pain relief
- Direct repair: 70-80% pain relief (if acute)
Long-Term Prognosis
Arthritis progression:
- With arthrodesis: 5-10% develop adjacent joint arthritis
- Without treatment: 20-30% develop arthritis
- Risk factors: Chronic instability, associated injuries
Differential Diagnosis of Ulnar-Sided Wrist Pain
Ulnar-sided wrist pain has many causes - LT instability is one of the harder diagnoses because radiographs are often normal. The following are the key mimics to exclude.
Differential Diagnosis - Ulnar Wrist Pain
| Condition | Key Distinguishing Feature | Best Test |
|---|---|---|
| LT instability | Positive ballottement; VISI on lateral (if static) | Arthroscopy / dynamic stress views |
| TFCC tear | Pain on ulnocarpal stress/grind; foveal tenderness | MRI / arthroscopy |
| Ulnar impaction syndrome | Positive ulnar variance; lunate/triquetrum chondral lesions | PA grip radiograph + MRI |
| DRUJ instability | Piano-key sign; pain on forearm rotation | Clinical + CT in pro/supination |
| Pisotriquetral arthritis | Pain over pisiform; positive grind | 30-degree supinated oblique X-ray |
| ECU tendinopathy / subluxation | Snapping ECU with supination/ulnar deviation | Dynamic ultrasound / MRI |
| Hamate hook fracture | Point tenderness over hook; grip pain | Carpal tunnel view / CT |
Controversies and Areas of Uncertainty
Arthrodesis vs Reconstruction
The traditional teaching that LT arthrodesis is the "gold standard" is challenged by series reporting nonunion rates up to ~45% (Vandesande 2001). Soft-tissue reconstruction (e.g. ECU strip, Pillukat 2015) and capsulodesis are increasingly favoured in some centres to preserve motion and proprioception. No randomised data exist.
Role of Ulnar Variance
Many "LT tears" are actually degenerative, driven by positive ulnar variance and ulnocarpal impaction. In these patients ulnar-shortening osteotomy - not LT surgery - may be the definitive treatment. Failing to assess variance is a classic error.
Static VISI - Is It Always LT?
Isolated LT injury alone does not always produce a fixed VISI. A static VISI usually requires additional disruption of the dorsal radiocarpal / palmar extrinsic ligaments. This nuance matters when planning whether soft-tissue surgery can succeed.
Diagnostic Gold Standard
Arthroscopy is the most reliable test, but central LTIL perforations (Palmer 1B type, degenerative) may be incidental and asymptomatic. Correlating arthroscopic findings with clinical instability - not treating every tear seen - is essential.
Evidence Base
Lunotriquetral Sprains - Original Description (Reagan)
- Defined LT sprain as discrete cause of ulnar wrist pain
- Described the LT ballottement manipulation (crepitus, laxity)
- Progression to VISI = LT dissociation
- Treatment depends on chronicity and severity
VISI / DISI - Carpal Instability Classification (Linscheid)
- Defined VISI and DISI patterns
- VISI = volar lunate tilt; DISI = dorsal lunate tilt
- Established lateral radiograph and intercalated-segment concept
LT Instability - Diagnosis and Treatment (Shin/AAOS review)
- Spectrum: partial tear to dislocation, dynamic to static
- Positive ulnar variance and attrition are key associations
- Ulnar shortening is a recognised option when ulna is positive
- Treatment matched to instability degree and chronicity
Lunotriquetral Arthrodesis - Technique and Union (Nelson)
- Herbert screw + K-wire superior to K-wires alone
- Immobilise over 6 weeks until union documented (at least 8 weeks)
- Union in all when both conditions met
- Plain films under-read the fusion - use fluoro/CT
LT Arthrodesis - High Failure Rate (Cautionary Series)
- Union in only 16/29 (45% nonunion)
- 17/29 remained painful; many needed reoperation
- Only 5/29 fully satisfied
- Challenges arthrodesis as automatic gold standard
Normal Carpal Kinematics (Kobayashi)
- Lunate rotates least of the proximal row; scaphoid most
- Lunate and triquetrum move closely together
- Translation minimal across all carpal bones
- Biomechanical basis for tolerability of LT fusion
Intercarpal Arthrodesis - Systematic Review
- Limited fusions predictable but reduce wrist ROM
- Nonunion is the principal complication
- Surface prep + bone graft + rigid fixation are critical
- LT fusion is a lesser-used, lesion-specific arthrodesis
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Chronic LT Instability with VISI
"A 35-year-old woman presents with 3 months of ulnar wrist pain and clicking. Clinical examination shows positive LT ballottement test. Lateral X-ray shows VISI deformity with lunate flexed volarly. The capitolunate angle is negative 10 degrees."
Scenario 2: Acute LT Injury
"A 28-year-old athlete presents 2 weeks after fall on outstretched hand with ulnar deviation. He has ulnar wrist pain and clicking. Clinical examination shows positive LT ballottement test. X-rays show no fixed deformity (dynamic instability)."
Scenario 3: Degenerative LT Tear with Positive Ulnar Variance
"A 52-year-old manual worker has 8 months of activity-related ulnar wrist pain, worse with gripping and forearm pronation. Ballottement is mildly positive and the ulnocarpal stress test reproduces pain. Radiographs show no VISI but a positive ulnar variance of plus 3 mm with subchondral changes in the lunate and triquetrum. MRI shows a central LTIL perforation and lunate chondromalacia."
MCQ Practice Points
VISI Deformity
Q: What is VISI and how does it differ from DISI? A: VISI (Volar Intercalated Segment Instability) = lunate flexes volarly (LT injury) - Opposite of DISI (Dorsal Intercalated Segment Instability) = lunate extends dorsally (SL injury). Capitolunate angle less than 0 degrees in VISI (normal 0-15 degrees).
LT Arthrodesis
Q: Why is LT arthrodesis the gold standard for chronic LT instability? A: High union rate (85-90%), minimal motion loss (LT contributes less than 5% to wrist motion), reliable pain relief, predictable outcomes - Preferred over ligament reconstruction for chronic instability. LT arthrodesis is treatment of choice.
LT Ballottement Test
Q: How do you perform the LT ballottement test? A: Stabilise lunate with one hand, translate triquetrum dorsally and palmarly with other hand - Positive = pain, crepitus, or increased motion. Compare to contralateral side. Also known as Reagan's test.
Acute vs Chronic
Q: When is direct repair preferred over LT arthrodesis? A: Acute injuries (less than 6 weeks) with good tissue quality - Direct repair achieves 70-80% good results if acute, but only 50-60% if chronic. LT arthrodesis preferred for chronic injuries (over 6 weeks).
Motion Loss
Q: Why does LT arthrodesis cause minimal functional impairment? A: LT joint contributes less than 5% to total wrist motion - Fusion of LT joint causes minimal motion loss functionally. This supports LT arthrodesis as treatment of choice for chronic instability.
Guidelines, Registries & Global Practice
LT instability is a relatively uncommon, often under-diagnosed cause of ulnar-sided wrist pain worldwide. There are no large dedicated registries or formal society guideline statements specific to LT instability - management is guided by hand-surgery consensus and case-series evidence. The cross-cutting controversy globally is whether chronic LT instability is best treated by LT arthrodesis, soft-tissue/tendon-graft reconstruction, or by addressing an underlying positive ulnar variance with ulnar-shortening osteotomy.
Global Epidemiology
- Relative frequency: Far less common than scapholunate injury; estimated at a minority of intrinsic carpal-ligament injuries presenting with ulnar wrist pain.
- Two distinct populations: (1) younger patients with a traumatic hyperextension/twisting mechanism or perilunate-spectrum injury; (2) older patients with degenerative tears related to ulnar-positive variance and ulnocarpal impaction (Shin AY et al, JAAOS 2000).
- Frequent comorbidity: TFCC tears and positive ulnar variance commonly coexist and must be assessed - they change the operation.
Side-by-Side Practice (no single society guideline)
| Body / School | Diagnostic Emphasis | Preferred Surgical Strategy |
|---|---|---|
| Mayo / North American (AAOS-aligned) | Ballottement + arthroscopy; assess ulnar variance | Acute repair; chronic = reconstruction or LT fusion; ulnar shortening if ulna positive |
| European (EFORT / IFSSH schools) | MRI + arthroscopy staging; proprioceptive focus | Capsulodesis / tendon reconstruction favoured; fusion reserved for failures |
| UK / BSSH practice | Arthroscopic grading, exclude TFCC pathology | Address ulnar impaction first; selective reconstruction or fusion |
Registry and Evidence Notes
- No implant registry captures LT-specific procedures (these are bone-and-soft-tissue, not arthroplasty), so evidence rests on small retrospective series and systematic reviews (Athlani L et al, Hand Surg Rehabil 2023).
- Arthrodesis outcomes are not uniform: union/failure rates vary widely between centres - from union in all patients with rigid Herbert-screw + K-wire fixation (Nelson DL et al, 1993) to ~45% nonunion in another series (Vandesande W et al, 2001). This heterogeneity is itself an exam discussion point.
High- vs Limited-Resource Settings
- High-resource: Wrist arthroscopy for diagnosis and staging, MRI, intra-operative fluoroscopy, and CT to confirm union are routine.
- Limited-resource: Diagnosis relies on clinical ballottement testing, plain radiographs (including stress/clenched-fist views) and, where available, arthrography. Immobilisation and ulnar-shortening or fusion with simpler fixation are pragmatic; advanced arthroscopic reconstruction may be unavailable.
Orthopaedic Exam Relevance
LT instability is a common viva topic globally (FRCS, FRACS, EBOT, ABOS, DNB). Know that VISI = Volar Intercalated Segment Instability (lunate flexes volarly, LT-side injury), that the LT ballottement (Reagan) test is the key bedside test, and that treatment is matched to chronicity. Be ready to argue BOTH sides of the arthrodesis-versus-reconstruction debate, to mention ulnar-shortening when the ulna is positive, and to quote that arthrodesis nonunion rates can reach ~40% in published series.
LUNOTRIQUETRAL INSTABILITY
Clinical summary
Key Concepts
- •VISI = Volar Intercalated Segment Instability (lunate flexes volarly, LT injury)
- •DISI = Dorsal Intercalated Segment Instability (lunate extends dorsally, SL injury)
- •LTIL = Lunotriquetral Interosseous Ligament
- •LT contributes less than 5% to wrist motion
Clinical Features
- •Ulnar wrist pain
- •Clicking or clunking with movement
- •VISI deformity (if static)
- •LT ballottement test positive (Reagan's test)
Treatment
- •Acute (less than 6 weeks): Direct repair with suture anchors (70-80% good results)
- •Chronic (over 6 weeks): LT arthrodesis (85-90% good results, gold standard)
- •Static VISI: LT arthrodesis (preferred)
- •With arthritis: LT fusion or salvage procedures
LT Arthrodesis Technique
- •Dorsal ulnar approach between 4th and 5th extensor compartments
- •Remove articular cartilage from lunate and triquetrum
- •Pack bone graft (autograft or allograft)
- •Fix with compression screw (headless cannulated) or plate/screws
- •Cast 6-8 weeks, then ROM exercises
Complications
- •Nonunion: 10-15% (prevent with rigid fixation, bone graft)
- •Persistent pain: 10-15% (assess for other causes)
- •Hardware issues: 5-10% (remove if symptomatic)
- •Loss of correction: 5-10% (prevent with rigid fixation)