Mayo Classification of Olecranon Fractures
Displacement is defined as a greater than 2 mm articular gap or step on the lateral radiograph. Stability is assessed by checking whether the ulnohumeral joint remains congruent when the elbow is flexed to 90 degrees under fluoroscopy. A fracture that appears displaced on the injury film but reduces to a congruent joint with the elbow flexed is Type II (stable), not Type III (unstable). Missing this distinction misclassifies the fracture and the wrong operation is offered in the viva. Also, the tension-band principle converts the tensile force of the triceps into compression at the articular surface — examiners will ask you to explain this and state when TBW fails (comminuted patterns, oblique fractures, or transverse fractures where the distal fragment is too short for two parallel K-wires).
The Mayo Classification System
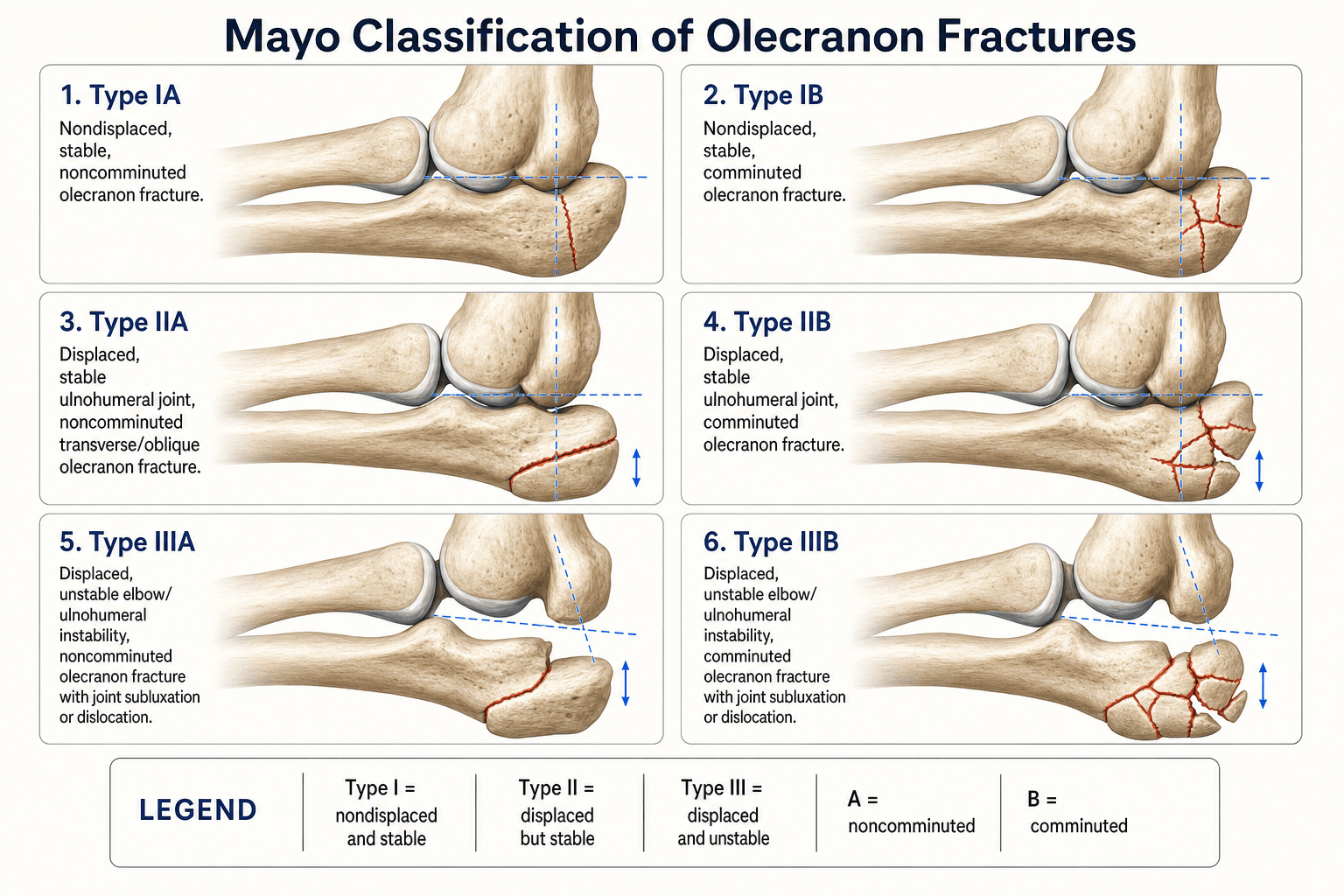

The Mayo (Morrey) classification was described by Bernard Morrey at the Mayo Clinic. It is the most widely used system for olecranon fractures and is built on three clinical assessments performed on the injury radiographs and confirmed on the table: displacement, ulnohumeral joint stability, and comminution.
- Displacement
- Less than 2 mm
- Joint Stability
- Stable
- Comminution
- Non-comminuted
- Typical Mechanism
- Direct fall on elbow, low energy
- Displacement
- Less than 2 mm
- Joint Stability
- Stable
- Comminution
- Comminuted
- Typical Mechanism
- Direct fall with impaction
- Displacement
- Greater than 2 mm
- Joint Stability
- Stable
- Comminution
- Non-comminuted
- Typical Mechanism
- Fall onto flexed elbow
- Displacement
- Greater than 2 mm
- Joint Stability
- Stable
- Comminution
- Comminuted
- Typical Mechanism
- High-energy direct blow
- Displacement
- Greater than 2 mm
- Joint Stability
- Unstable
- Comminution
- Non-comminuted
- Typical Mechanism
- Fall with varus or valgus force
- Displacement
- Greater than 2 mm
- Joint Stability
- Unstable
- Comminution
- Comminuted
- Typical Mechanism
- High-energy, polytrauma
DSUThe three assessment axes
Hook:Three binary answers (DSU) place the fracture in one of six Mayo types, IA to IIIB.
Stability is a clinical and fluoroscopic assessment, not a reading of the static film alone. A displaced fracture with an incongruent joint on the injury radiograph may reduce when the elbow is brought to 90 degrees — that is a Type II (stable), not Type III. Assess stability on the operating table under image intensifier before committing to a classification. The distinction between Type II and Type III determines whether plate fixation alone suffices (Type II) or whether you must also address collateral ligament injury, an associated coronoid fracture, or a more complex instability pattern (Type III).
The Mayo system does not capture the complex injuries a Type III olecranon fracture is often part of — examiners expect you to name and separate them:
- Trans-olecranon fracture-dislocation: a high-energy injury in which the ulnohumeral joint dislocates THROUGH a (usually comminuted) proximal-ulna fracture, but the proximal radioulnar joint and the radiocapitellar relationship are PRESERVED — the radius tracks with the distal/coronoid fragment. That preserved PRUJ is the key distinction from a Monteggia lesion, where the radial head dislocates. Restore the trochlear-notch (greater sigmoid notch) contour with a strong dorsal plate; the coronoid is usually involved and must be fixed, after which the elbow is generally stable.
- The coronoid is the critical anterior buttress against posterior subluxation — classify it two ways: Regan-Morrey by height (I tip, II up to half, III over half of the coronoid) and O'Driscoll by location (tip, anteromedial facet, base) — the anteromedial facet fracture is the one that causes varus posteromedial rotatory instability and usually needs a buttress plate.
- Terrible triad = elbow dislocation + radial head fracture + coronoid fracture. Repair it in a systematic order — coronoid/anterior capsule, then radial head (fix or replace, do not excise), then the lateral collateral ligament, adding the medial collateral ligament or a hinged external fixator if still unstable.
Treatment by Classification Type
The classification guides treatment through a decision ladder from non-operative care to tension-band wiring, plate fixation, and fragment excision — each matched to the fracture morphology.
- Management
- Non-operative
- Preferred Fixation
- None — cast or brace
- Key Considerations
- Above-elbow backslab in 90 degrees flexion for 3 weeks, then hinged brace with progressive ROM. Repeat radiographs at 1 and 3 weeks to exclude delayed displacement. Long-arm cast if patient unreliable or bone very poor
- Management
- ORIF
- Preferred Fixation
- Tension-band wiring (TBW)
- Key Considerations
- Simple transverse or short oblique pattern with an adequate distal fragment for two parallel K-wires at least 1 cm distal to the fracture. Check articular reduction and triceps tension before tightening the figure-of-eight wire
- Management
- ORIF
- Preferred Fixation
- Plate fixation
- Key Considerations
- Comminution precludes reliable TBW biomechanics. Contour a pre-contoured olecranon plate to the proximal ulna; supplement with lag screws for articular fragments. Protect the ulnar nerve throughout
- Management
- ORIF
- Preferred Fixation
- Plate fixation
- Key Considerations
- Displaced with an unstable joint — anatomic articular reduction is mandatory. Plate long enough to bridge the fracture by at least three cortices proximal and distal. Check and address collateral ligament integrity and associated coronoid fractures
- Management
- ORIF or excision
- Preferred Fixation
- Plate (young/active); excision plus triceps advancement (elderly/low demand)
- Key Considerations
- Severe comminution may make anatomic fixation impossible. In frail or low-demand patients, excision of the proximal fragment with triceps advancement gives reliable pain relief and acceptable function. Reserve excision for older adults; generally avoid in younger patients
Tension-band wiring requires a technically adequate distal fragment. If the distal pole is too short to accept two parallel K-wires with a minimum of 1 cm of purchase distal to the fracture, TBW will fail — plate fixation is the correct choice. Do not force TBW onto a fracture pattern that does not suit it. Symptomatic hardware prominence requiring removal is the most common complication of TBW, reported in a significant proportion of cases across multiple series.
TPEThe three operative options
Hook:TPE maps directly onto rising fracture complexity: tension-band → plate → excision.
Tension-Band Wiring versus Plate Fixation
Understanding why one fixation method is chosen over another is tested in the viva and in the written examination.


- Tension-Band Wiring
- Simple transverse, short oblique
- Plate Fixation
- Comminuted, long oblique, transverse with distal fragment too short, unstable patterns
- Tension-Band Wiring
- Converts triceps tension into articular compression
- Plate Fixation
- Provides rigid stability; resists bending and shear from all directions
- Tension-Band Wiring
- Common — K-wires and wire often prominent subcutaneously
- Plate Fixation
- Less common with modern low-profile plates; still possible over the olecranon tip
- Tension-Band Wiring
- Higher (mainly for hardware removal)
- Plate Fixation
- Lower
- Tension-Band Wiring
- High in simple patterns
- Plate Fixation
- High in all patterns, including comminuted
- Tension-Band Wiring
- Lower (K-wires and stainless-steel wire)
- Plate Fixation
- Higher (pre-contoured plate and screws)
- Tension-Band Wiring
- Type IIA, young patient, good bone quality
- Plate Fixation
- Types IIB, IIIA, IIIB; osteoporotic bone; patients needing early mobilisation
The tension-band principle relies on the triceps pulling the olecranon proximally while the figure-of-eight wire resists that pull and converts it into compression at the articular surface. This only works when the olecranon fragment is large enough for the K-wires to engage anterior cortex and the distal fragment is substantial. If either pole is inadequate, the construct fails. Plate fixation does not depend on this principle — it resists load through bending stiffness of the plate itself.
ARUThree structures at risk during olecranon fixation
Hook:ARU: restore the Articular surface, Repair the triceps, protect the Ulnar nerve.
Three practical layers the topic implies but never sets out:
- Complications (in order of frequency): symptomatic hardware needing removal — the commonest, especially after TBW (around half of cases); K-wire migration/backout — the dangerous one, avoided by engaging the anterior ulnar cortex and bending and burying the proximal wire ends deep to the triceps; elbow stiffness / loss of terminal extension — the elbow is unforgiving of immobilisation, so mobilise early; ulnar neuritis; post-traumatic arthritis from a residual articular step or gap; and the less common nonunion, infection and heterotopic ossification.
- The proximal-ulna plating pitfall (PUDA): the proximal ulna is not straight — it has a normal proximal ulnar dorsal angulation (roughly 5 to 7 degrees) a few centimetres distal to the tip, plus a slight varus/rotational alignment. Applying a straight or over-bent plate can malreduce and narrow the trochlear notch and alter forearm rotation and the carrying angle, so use a pre-contoured olecranon plate and template against the contralateral uninjured limb. (Note the non-articular transverse "bare area" at the midpoint of the trochlear notch — a normal landmark, not a fracture step.)
- Outcome scores you should name: elbow results are reported with the Mayo Elbow Performance Score (MEPS) — pain, motion, stability and function out of 100 — together with the Broberg-Morrey score and the DASH (disabilities of the arm, shoulder and hand) the evidence base quotes.
Limitations and Clinical Decision Points
- The 2 mm displacement threshold is arbitrary. Many surgeons use 2 mm as the boundary between non-operative and operative treatment, but there is no high-level evidence that exactly 2 mm (rather than 1 mm or 3 mm) is the definitive cut-off. Use clinical judgement alongside the number: a young manual worker with 2 mm of articular step may benefit from fixation, whereas a frail elderly patient with 3 mm and a stable joint might reasonably be managed non-operatively.
- Stability assessment is operator-dependent. The distinction between Type II and Type III requires the elbow to be examined under anaesthesia or fluoroscopy, which is not always documented in retrospective series. Inter-observer agreement for the stable versus unstable distinction is moderate at best.
- The classification does not account for associated injuries. Coronoid fractures, radial head fractures, collateral ligament injuries, and Monteggia-equivalent patterns all affect prognosis and treatment but are not captured by the Mayo system. A Type III olecranon fracture is frequently part of a more complex elbow instability pattern that the classification alone does not describe.
- The comminution subcategory (A versus B) is inconsistently applied. There is no formal definition of how many fragments constitute comminution. Surgeons use it as a guide to fixation strategy rather than as a strict binary divider.
- TBW versus plate remains debated in practice. Biomechanical and clinical studies show plate fixation is stronger and has a lower reoperation rate, but TBW remains a valid, low-cost option for the right fracture pattern (simple transverse, good bone quality, adequate distal fragment). Choice depends on surgeon experience, patient factors, and fracture morphology rather than a rigid rule.
- Excision outcomes are patient-dependent. Triceps strength and elbow extension power decline measurably after olecranon excision. Reserve this option for patients who can tolerate some loss of extension strength — elderly, sedentary, or those with low upper-limb demands.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman falls onto her left elbow. Radiographs show a transverse fracture of the olecranon with approximately 4 mm of displacement. The ulnohumeral joint appears congruent on the anteroposterior view. How would you classify this fracture and what would you do?”
“An 84-year-old woman with osteoporosis presents after a fall. Radiographs show a severely comminuted olecranon fracture with over 15 mm of displacement. The ulnohumeral joint is incongruent, and the proximal fragment consists of multiple small pieces with no single fragment suitable for plate fixation. She lives independently and uses a walking stick. What are her options?”
The three axes: D-S-U
- Displacement: less than 2 mm (Type I) versus greater than 2 mm (Types II and III)
- Stability: ulnohumeral joint congruent (Types I and II) versus incongruent (Type III)
- Comminution: A = non-comminuted, B = comminuted
- Six patterns total: IA, IB, IIA, IIB, IIIA, IIIB
Treatment by type
- Type I: non-operative — backslab in 90 degrees for 3 weeks, then hinged brace with progressive ROM
- Type IIA: tension-band wiring (simple transverse, adequate distal fragment)
- Type IIB: plate fixation (comminuted, TBW biomechanically insufficient)
- Type IIIA: plate fixation (unstable joint, anatomic reduction mandatory)
- Type IIIB: plate fixation (young/active) or excision plus triceps advancement (elderly/low demand)
Tension-band wiring essentials
- Two parallel K-wires from the olecranon tip across the fracture into the anterior ulna cortex
- Figure-of-eight 18-gauge wire through a distal drill hole, tightened to compress the articular surface
- Distal fragment must be long enough for at least 1 cm of K-wire purchase below the fracture
- Most common complication: symptomatic hardware prominence requiring removal
Excision criteria and technique
- Reserved for elderly, low-demand patients with irreparable comminution (selected Type IIIB)
- Triceps advanced into bone tunnels or transosseous sutures in the remaining proximal ulna
- Accept loss of extension power; expect reliable pain relief and acceptable ROM for daily living
- Avoid in young or high-demand patients who need a competent extensor mechanism
Associated injuries to check in Type III
- Coronoid process fracture — especially in Type III, suggests a more complex instability pattern
- Radial head fracture — combined olecranon and radial head fracture is a terrible triad variant
- Medial collateral ligament injury — valgus instability in Type III patterns
- Monteggia-equivalent — check the radial head and proximal radioulnar joint alignment
Evidence Base
Every citation below has been checked against its source record in PubMed. The take-home pattern across the modern evidence is that, for the right simple fracture, plate fixation and tension-band wiring give similar function — but TBW carries more hardware-related problems — and that in the elderly, operative fixation can carry an unexpectedly high complication burden, which is why non-operative management is reasonable in that group.
Olecranon fractures: treatment options
- Review of olecranon fracture management: non-displaced fractures are immobilised then mobilised; displaced intra-articular fractures undergo ORIF
- Figure-of-eight tension-band wiring (using two knots for symmetric tension) is described for simple transverse fractures, allowing early motion
- Plate fixation is recommended for severely comminuted fractures, fractures involving the coronoid, oblique fractures distal to the trochlear-notch midpoint, Monteggia fracture-dislocations and nonunions; fragment excision with triceps advancement is reserved for selected osteoporotic elderly patients
Surgical Management for Olecranon Fractures in Adults: A Systematic Review and Meta-analysis
- Systematic review of 24 studies; meta-analysis of 10 comparing tension-band wiring (n=270) with plate fixation (n=369)
- Plate fixation had a significantly lower overall complication rate (relative risk 0.48, 95% CI 0.36-0.64)
- Plate fixation also had significantly less hardware removal than TBW (relative risk 0.36, 95% CI 0.25-0.50)
Prospective randomised trial of non-operative versus operative management of olecranon fractures in the elderly
- Randomised trial in patients aged 75 and over (only 19 randomised: 8 non-operative, 11 operative); primary outcome was the DASH score
- The trial was STOPPED EARLY because the operative group had an unacceptable complication rate (9 of 11, 81.8%)
- There was no significant difference in DASH (mean 23 vs 22 at one year), Broberg-Morrey or Mayo Elbow Score between groups