3-5% of ankle sprains | Deltoid 2-3× stronger than ATFL | 40-60% syndesmotic association | MCS >4 mm diagnostic
- Deep posterior tibiotalar strongest component
- Isolated injury rare (<5%)
- Syndesmotic injury in 40-60%
- Conservative succeeds in 60-70%
- Surgical outcomes 75-90%
- “Medial clear space normal <4mm on mortise view
- “External rotation stress test for deep deltoid
- “Repair deep layer first in surgery
- “Position ankle neutral dorsiflexion + 5° inversion
Medial Ankle Instability
High-yield exam focus: Understanding deltoid anatomy (superficial vs deep components), recognizing associated injuries (syndesmosis, PTTD, fractures), differentiating medial gutter pain from true instability, identifying when surgical intervention is required, and managing concomitant pathology. Examiners expect discussion of why isolated deltoid injury is rare and what forces/injuries cause deltoid disruption.
Viva Overview Summary
Key Points for Viva
- 3-5% of ankle sprains (much less common than lateral)
- Deltoid is 2-3x stronger than ATFL
- Isolated injury is rare
- Syndesmotic injury (40-60% of deltoid injuries)
- Pronation-external rotation ankle fractures
- Stage 4 PTTD with flatfoot
- Key Point
- 3-5% of ankle sprains
- Key Point
- Deltoid + syndesmosis (40-60%)
- Key Point
- 60-70%
Complications Overview
Complication Summary
- Wound healing (5-8%)
- Saphenous nerve injury (10-15%, mostly neurapraxia)
- PTN injury (less than 1%)
- Stiffness (15-20%)
- Persistent instability (10-15%)
- Post-traumatic arthritis (20-30% with fractures)
- Incidence
- 10-15%
- Outcome
- Most resolve 3-6 months
- Incidence
- 15-20%
- Outcome
- May need PT or MUA
- Incidence
- 10-15%
- Outcome
- May need revision
Anatomy and Biomechanics
Deltoid Ligament Complex
The deltoid ligament is the primary medial ankle stabilizer, consisting of superficial and deep layers with distinct anatomic and functional characteristics.
Components: Tibionavicular, tibiocalcaneal (superficial), tibiospring ligaments Origin: Anterior colliculus of medial malleolus Insertion: Navicular tuberosity, sustentaculum tali, spring ligament Orientation: Fan-shaped, broad insertion Primary function: Restraint to hindfoot valgus, secondary restraint to external rotation Clinical note: More commonly injured in isolation, better healing potential Blood supply: Medial tarsal artery branches
Components: Anterior tibiotalar, posterior tibiotalar, tibiocalcaneal (deep) Origin: Intercollicular groove and posterior colliculus of medial malleolus Insertion: Medial talus (tubercle), medial calcaneal wall Orientation: Thick, cord-like bands Primary function: Critical restraint to external rotation and lateral talar shift Clinical significance: Deep component injury indicates severe force, often associated with syndesmotic disruption Strongest component: Posterior tibiotalar (deep) is strongest and most critical for stability
Components: Superomedial, medioplantar oblique, inferoplantar longitudinal bands Connection: Intimately associated with superficial deltoid (tibiospring fibers) Function: Supports talar head, maintains medial longitudinal arch Dual pathology: Spring ligament injury often accompanies deltoid insufficiency Clinical presentation: Combined injury leads to valgus hindfoot and flatfoot deformity Surgical consideration: Both may require reconstruction in chronic cases
Biomechanical Function
The deltoid complex is the principal restraint to lateral talar translation and external rotation of the talus within the mortise, and a major restraint to hindfoot valgus. The deep posterior tibiotalar ligament is the strongest, most consistent band and the key restraint to lateral talar shift; the superficial layer (acting with the spring ligament as the tibiocalcaneonavicular complex) chiefly resists hindfoot valgus and supports the medial longitudinal arch. Band engagement is position-dependent: the tibiospring band tightens in plantarflexion, whereas the tibiocalcaneal and deep posterior tibiotalar bands tighten in dorsiflexion. Deltoid competence is also essential for syndesmotic stability, an incompetent deltoid permits medial clear space widening and lateral talar shift even with an intact syndesmosis, which is why restoring medial stability can normalise the mortise.
Deltoid Anatomy Summary
Two-Layer Structure
- Tibionavicular, tibiocalcaneal, tibiospring
- Origin: Anterior colliculus
- Function: Restraint to hindfoot valgus
- Anterior and posterior tibiotalar
- Origin: Intercollicular groove
- Function: Restraint to external rotation and lateral talar shift
- Components
- Tibionavicular, tibiocalcaneal, tibiospring
- Function
- Hindfoot valgus restraint
- Components
- Anterior/posterior tibiotalar
- Function
- External rotation, lateral shift
Pathophysiology and Injury Mechanisms
Injury Patterns and Associated Pathology
Isolated deltoid ligament injury is rare due to the ligament's substantial strength (2-3 times stronger than ATFL). Most deltoid injuries occur as part of more complex injury patterns.
- mechanism
- Direct valgus force with external rotation (rare)
- associatedInjuries
- Usually none, occasionally spring ligament injury
- incidence
- Less than 5% of deltoid injuries
- treatment
- Conservative management, immobilization 4-6 weeks
- prognosis
- Good, 70-80% resolution with conservative care
- mechanism
- Pronation-external rotation force
- associatedInjuries
- AITFL disruption (40-60%), IOL injury, fibular fracture
- incidence
- Most common pattern (40-60% of deltoid injuries)
- treatment
- Syndesmotic fixation priority, deltoid may require repair
- prognosis
- Dependent on syndesmosis treatment, deltoid usually heals
- mechanism
- Valgus force with abduction, oblique medial malleolus fracture
- associatedInjuries
- Medial malleolus fracture, lateral ligament injury or fibula fracture
- incidence
- 20-30% of deltoid pathology presentations
- treatment
- ORIF medial malleolus, deltoid repair if tissue quality poor
- prognosis
- Good with anatomic fracture reduction
- mechanism
- Chronic progressive valgus deformity and arch collapse
- associatedInjuries
- PTT rupture, spring ligament attenuation, subtalar arthritis
- incidence
- 10-15% of deltoid presentations
- treatment
- Reconstruction vs fusion based on arthritis presence
- prognosis
- Complex, depends on deformity correction and arthritic changes
Clinical Imaging
Imaging Atlas



Acute vs Chronic Deltoid Insufficiency
Acute deltoid injuries typically result from high-energy trauma with forced valgus and external rotation. Clinical presentation includes significant medial ankle swelling, ecchymosis extending to hindfoot, inability to weight-bear, and positive external rotation stress test. MRI demonstrates ligament discontinuity with surrounding edema. Treatment prioritizes identifying and addressing associated injuries, particularly syndesmotic disruption.
Chronic deltoid insufficiency develops from untreated acute injury, repetitive microtrauma in athletes (gymnastics, soccer), or progressive deformity in PTTD. Presents with medial ankle pain, subjective instability, and valgus hindfoot alignment. MRI shows ligament thickening, scarring, or complete attenuation. May have widened medial clear space on weight-bearing radiographs. Treatment requires addressing underlying biomechanical abnormalities.
Clinical Evaluation
History and Physical Examination
Patient history should elicit mechanism of injury (valgus force, external rotation), previous ankle injuries or instability, and functional limitations. Pain with cutting or pivoting activities suggests rotational instability. History of flatfoot or PTTD relevant for chronic cases.
Mnemonic
Hook:STAMP
Inspection reveals medial ankle swelling in acute injuries or valgus hindfoot deformity in chronic cases. Observe for pes planus deformity suggesting concurrent PTTD or spring ligament insufficiency. Check for antalgic gait or inability to perform single heel raise.
Palpation should systematically assess medial malleolus, deltoid ligament course (from anterior colliculus inferiorly), spring ligament (plantar-medial to navicular), and PTT course. Tenderness localizes injury and identifies associated pathology.
Special Tests:
- External rotation stress test: With knee flexed 90 degrees and ankle in neutral, apply external rotation force to foot. Pain and increased rotation compared to contralateral side indicates deltoid injury
- Valgus stress test: Apply valgus force to hindfoot with ankle in neutral. Increased medial joint opening suggests deltoid insufficiency
- Kleiger test: External rotation of foot with ankle dorsiflexed and tibia stabilized. Pain at medial ankle indicates deltoid injury; pain at syndesmosis suggests combined pathology
- Single heel raise test: Inability to perform or lack of hindfoot inversion during raise indicates PTT dysfunction or severe deltoid insufficiency
Imaging Protocol
Views required: AP, lateral, mortise of ankle; AP and lateral foot Key measurements: Medial clear space (normal less than 4mm), talonavicular coverage angle, lateral talar station Stress views: External rotation stress radiograph may demonstrate medial clear space widening Fracture assessment: Medial malleolus, fibula, posterior malleolus Chronic findings: Valgus tilt, talar subluxation, arthritic changes
Indications: Suspected deltoid injury, chronic instability, pre-operative planning Protocol: T1, T2, STIR sequences in coronal, sagittal, and axial planes Deltoid assessment: Grade 1 (intact fibers with edema), Grade 2 (partial tear), Grade 3 (complete disruption) Associated pathology: Syndesmosis, spring ligament, PTT, osteochondral lesions, bone bruising Chronic changes: Ligament thickening, scarring, attenuation without discrete tear
Indications: Fracture characterization, pre-operative planning, arthritic assessment Advantages: Superior bony detail, assessment of subtalar joint Weight-bearing CT: Emerging technology for dynamic assessment of hindfoot alignment 3D reconstruction: Helpful for complex fracture patterns Limitations: Poor soft tissue resolution, radiation exposure
Medial clear space measurement on mortise radiograph is critical diagnostic parameter. Normal is less than 4mm and should equal superior clear space. Widening greater than 4mm or asymmetry compared to contralateral ankle indicates deltoid insufficiency or syndesmotic injury. Weight-bearing radiographs essential for accurate assessment.
Injury Classification
Classification by Pattern
- Isolated deltoid (less than 5%): Direct valgus force
- With syndesmosis (40-60%): Pronation-external rotation
- With fracture (20-30%): Pronation-abduction
- Stage 4 PTTD (10-15%): Chronic progressive
- Grade 1: Intact fibers with edema
- Grade 2: Partial tear
- Grade 3: Complete disruption
- Incidence
- Less than 5%
- Prognosis
- Good (70-80% conservative)
- Incidence
- 40-60%
- Prognosis
- Depends on syndesmosis treatment
- Incidence
- 10-15%
- Prognosis
- Complex, multi-procedure needed
Clinical Examination Summary
Key Clinical Tests
- Knee flexed 90°, ankle neutral
- Externally rotate foot
- Pain and increased rotation = positive
- Apply valgus force to hindfoot
- Compare to contralateral side
- Increased opening = deltoid insufficiency
- Tests PTT function
- Inability or lack of inversion = dysfunction
- What It Tests
- Deep deltoid
- Positive Finding
- Pain, increased rotation
- What It Tests
- Both layers
- Positive Finding
- Increased medial opening
- What It Tests
- PTT function
- Positive Finding
- Unable or no inversion
Viva Imaging Review
Key Imaging Findings
- Medial clear space: Normal less than 4mm
- Greater than 4mm = deltoid insufficiency
- Must compare to contralateral
- Grade 1: Intact fibers with edema
- Grade 2: Partial tear (some fibers intact)
- Grade 3: Complete disruption
- Syndesmosis injury
- Spring ligament attenuation
- Osteochondral lesions
- Key Finding
- Medial clear space greater than 4mm
- Significance
- Deltoid/syndesmosis injury
- Key Finding
- Grade 3 disruption
- Significance
- Complete tear, may need surgery
- Key Finding
- Widening with stress
- Significance
- Confirms instability
Differential Diagnosis
Medial ankle pain with a sense of "giving way" has several mimics. The key task is separating true medial instability (deltoid/spring incompetence with talar tilt or shift) from medial gutter pathology and tendon disorders that cause pain without instability.
- keyFeatures
- Giving way on valgus or external rotation; medial clear space widening on stress or weight-bearing
- examination
- Positive external rotation and valgus stress tests; pain over deltoid course
- imaging
- Medial clear space over 4mm; deltoid discontinuity or attenuation on MRI
- discriminator
- Demonstrable talar tilt or shift is the defining feature
- keyFeatures
- Progressive flatfoot, medial arch pain, fatigue with walking
- examination
- Too-many-toes sign; unable to perform single-heel-raise or no hindfoot inversion
- imaging
- PTT tenosynovitis, split or rupture on MRI; hindfoot valgus on weight-bearing CT
- discriminator
- Tendon, not ligament, is the primary lesion; deltoid stress may be secondary
- keyFeatures
- Activity-related medial pain in runners; no instability
- examination
- Focal bony tenderness at medial malleolus; negative ligament stress tests
- imaging
- Vertical lucency or marrow oedema on MRI; line on radiograph
- discriminator
- Bony tenderness without talar tilt; stress tests negative
- keyFeatures
- Burning, tingling on plantar foot; night symptoms
- examination
- Positive Tinel over tarsal tunnel; sensory disturbance, no mechanical instability
- imaging
- Mass or varix on MRI; nerve conduction abnormalities
- discriminator
- Neuropathic, not mechanical; no ligament laxity
- keyFeatures
- Pain at end-range dorsiflexion, no giving way
- examination
- Tenderness anteromedial joint line; impingement on forced dorsiflexion
- imaging
- Anteromedial osteophytes or soft-tissue thickening; stable mortise
- discriminator
- Positional pain without instability; mortise reduced
- keyFeatures
- Talar head uncoverage, peritalar instability, arch collapse
- examination
- Plantar-medial tenderness to navicular; talar head prominence
- imaging
- Superomedial spring ligament tear on MRI; talonavicular uncoverage
- discriminator
- Often coexists with deltoid injury (TCNL complex) rather than isolated
Conservative Management
Treatment Protocol for Acute Injuries
Non-operative management is first-line treatment for isolated deltoid sprains without fracture or syndesmotic injury, successful in 60-70% of cases.
Phase 1 (0-3 weeks): Protection and Immobilization
- CAM boot or short leg cast, non-weight-bearing for grade 2-3 injuries
- Protected weight-bearing for grade 1 injuries after first week
- Ice, elevation, compression for edema control
- NSAIDs for pain management (if no contraindications)
Phase 2 (3-6 weeks): Progressive Weight-Bearing
- Transition to weight-bearing as tolerated in CAM boot
- Begin gentle ankle range of motion exercises (avoid forced eversion)
- Initiate isometric strengthening (tibialis posterior, gastrocnemius)
- Continue until pain-free with daily activities
Phase 3 (6-12 weeks): Strengthening and Return to Activity
- Progress to lace-up ankle brace or taping
- Progressive resistance exercises focusing on tibialis posterior and invertor muscles
- Proprioceptive training (single leg balance, wobble board)
- Sport-specific training with gradual progression
- May require 3-4 months for return to high-level athletics
Critical assessment for syndesmotic injury required in all deltoid injuries. Failure to identify and treat concurrent syndesmosis disruption leads to chronic pain, instability, and post-traumatic arthritis. Perform syndesmotic squeeze test, external rotation stress test, and consider MRI if clinical suspicion despite negative radiographs.
Indications for Surgical Intervention
Conservative management fails in 30-40% of cases, requiring surgical consideration. Indications for surgery include:
Absolute indications:
- Acute deltoid disruption with syndesmotic instability requiring fixation
- Deltoid disruption with widened medial clear space (greater than 4mm) despite syndesmotic fixation
- Chronic symptomatic instability with functional limitation despite 4-6 months therapy
- Stage 4 PTTD with deltoid insufficiency and progressive deformity
Relative indications:
- High-demand athletes with persistent symptoms after 3 months conservative care
- Deltoid injury associated with medial malleolus fracture with comminution preventing stable fixation
- MRI-confirmed complete deltoid rupture with poor tissue quality in acute setting
Viva Treatment Review
Management Approach
- CAM boot/cast 4-6 weeks
- Progressive weight-bearing
- Strengthening and proprioception
- Success rate: 60-70%
- Deltoid + syndesmosis requiring fixation
- Widened MCS despite syndesmosis reduction
- Chronic instability failed 4-6 months therapy
- Stage 4 PTTD
- Treatment
- Conservative
- Expected Outcome
- 70-80% success
- Treatment
- Fix syndesmosis, assess MCS
- Expected Outcome
- MCS may normalise
- Treatment
- Reconstruction
- Expected Outcome
- 75-85% success
Surgical Management
Direct Deltoid Ligament Repair
Primary repair of acute deltoid injuries is performed when good tissue quality exists and injury is part of operative ankle fracture or syndesmotic fixation.
Patient Positioning: Supine, bump under ipsilateral hip, thigh tourniquet, foot over end of table or on folded towel for access to medial ankle.
Incision: Curvilinear incision centered over medial malleolus, extending from just proximal to tip distally along deltoid course (6-7cm length). Alternative: use medial malleolar fracture fixation incision if present.
Approach: Full-thickness skin flaps to expose medial malleolus, deltoid ligament, and tibialis posterior tendon. Identify and protect saphenous vein and nerve (anterior to incision). Great saphenous nerve at risk with anterior extension.
Deltoid Assessment:
- Identify level of disruption (most commonly at tibial origin or midsubstance)
- Differentiate superficial from deep components
- Assess tissue quality for primary repair vs augmentation requirement
- Inspect for associated injuries (spring ligament, PTT, medial talar osteochondral lesion)
Repair Technique:
- Debride devitalized tissue conservatively
- Place suture anchors (3.0-3.5mm) at anatomic deltoid origin on medial malleolus
- Anterior colliculus for superficial layer
- Intercollicular groove for deep components
- Use high-strength sutures (2-0 or 0 nonabsorbable)
- Repair deep layer first (critical for rotational stability)
- Superficial layer repaired separately with slight overlap
- Ankle positioned in neutral dorsiflexion and 5 degrees hindfoot inversion during tie-down
- Consider suture augmentation with internal brace for high-demand athletes
Spring Ligament Assessment: If spring ligament injury identified (palpable defect plantar-medial to navicular, talar head uncoverage on radiograph), address concurrently with suture anchor repair or reconstruction.
Closure: Deep layer with absorbable suture, skin with nonabsorbable suture or staples. Well-padded posterior splint with ankle in neutral position, hindfoot slight inversion.
Ankle positioning during deltoid repair is critical: neutral dorsiflexion and 5 degrees hindfoot inversion (not eversion or valgus). This prevents overtightening causing stiffness while ensuring adequate tension for stability. Compare to contralateral ankle for appropriate positioning.
Postoperative Management
Rehabilitation Protocol
Immobilization: Posterior splint or CAM boot, strict non-weight-bearing Activity: Toe wiggling, ankle pumps (plantarflexion/dorsiflexion only) Precautions: No eversion, no forced dorsiflexion Wound care: Suture removal 10-14 days, monitor for infection Pain control: Multimodal analgesia, ice, elevation
Weight-bearing: Progress from non-weight-bearing to 50% by week 6 Immobilization: CAM boot with gradual increase in time out for exercises ROM exercises: Active ankle pumps, gentle inversion-eversion (no forced eversion) Strengthening: Isometric tibialis posterior, gastrocnemius contractions PT initiation: Week 3-4 for edema control and supervised ROM
Weight-bearing: Progress to full weight-bearing in boot, then transition to brace Immobilization: Lace-up ankle brace or Arizona brace for support Strengthening: Progressive resistance with theraband, focus on tibialis posterior Proprioception: Single leg balance, wobble board exercises Functional activities: Pool walking, stationary bike, elliptical Return to work: Sedentary 8-10 weeks, manual labor 12-14 weeks
Criteria: Full strength, normal ROM, negative stress tests, functional testing passed Progression: Walk-jog program, straight-line running, cutting drills, sport-specific Bracing: External ankle brace recommended for sports for 12 months Success rate: 80-90% return to pre-injury activity level Long-term: Permanent brace may be needed for high-level athletics
Mnemonic
Hook:PIER Deltoid Recovery
Stress Radiographs for Medial Instability
The imaging protocol and the vivas repeatedly rely on "external rotation stress" and "gravity-stress" views (and the controversies flag that their technique varies), and normal plain films famously do not exclude the injury - but how the views are taken is never described.
- Why they are needed. Static non-weight-bearing films can look normal because the talus reduces at rest. A stress or weight-bearing view loads the medial side to unmask a widened medial clear space or talar tilt.
- Manual external-rotation stress view. A mortise radiograph is taken while an external-rotation force is applied to the plantigrade foot with the tibia held. A medial clear space over 4 mm, side-to-side asymmetry over 1 mm versus the contralateral ankle, or a medial clear space exceeding the superior clear space indicates deltoid incompetence - the same test that decides whether a supination-external-rotation (SER) fibular fracture is "stable" (deltoid intact) or "unstable" (deltoid torn, needs fixation).
- Gravity stress view. The patient lies with the injured leg dependent (lateral decubitus, ankle unsupported) and gravity supplies the external-rotation/eversion load, giving a mortise view without the examiner's hand in the field. It is about as reliable as the manual test for detecting deltoid incompetence in SER fractures and avoids irradiating the examiner.
- Weight-bearing views. For chronic instability, standing AP/mortise views (and weight-bearing CT) reproduce physiological load and reveal valgus talar tilt and peritalar subluxation better than a supine film.
- The caveat. The 4 mm cut-off and side-to-side comparison are pragmatic rather than rigorously validated and stress technique varies between centres - so interpret the number alongside the clinical stress examination rather than in isolation.
Q: How do you use stress radiographs to diagnose medial ankle instability (and to judge an SER fracture)? A: Because the talus reduces at rest, static films can look normal - so apply a load. A manual external-rotation stress mortise view (or a gravity stress view, leg dependent so gravity supplies the load) unmasks a medial clear space over 4 mm, side-to-side asymmetry over 1 mm, or a medial clear space exceeding the superior clear space - deltoid incompetence. This same test decides whether an SER fibular fracture is stable (deltoid intact) or unstable (deltoid torn to fixation). Weight-bearing views / weight-bearing CT are better for chronic valgus tilt.
Suture-Tape (Internal Brace) Augmentation
The repair technique, the combined-procedures tab, the controversies and a viva followUp all mention "suture-tape / internal brace augmentation", and the management algorithm says to "consider internal brace if high-demand" - but the construct and its role are never described.
- What it is. A suture-tape (e.g. FiberTape) internal brace is a strong, non-absorbable tape secured with anchors that spans the repaired or reconstructed deltoid as an independent load-sharing "check-rein" - typically a medial malleolar anchor to a talar (and/or calcaneal/sustentacular) anchor recreating the deep and superficial vectors.
- Why it is used. It is not the primary repair; it protects the biological repair/graft while it heals, restrains external rotation and valgus, and is intended to permit earlier, safer rehabilitation - the same rationale as internal bracing of the lateral ligament.
- When it is offered. In poor-quality tissue (chronic, diabetic, revision), in high-demand athletes, and to reinforce a repair that would otherwise be marginal - hence the algorithm's "consider internal brace if high-demand".
- The caveat. Evidence is largely biomechanical and short-term small series; it supplements rather than replaces anatomic repair, and over-tensioning the tape risks stiffness or over-constraint - so routine use is not established.
Q: What is suture-tape (internal brace) augmentation of a deltoid repair and when is it used? A: A strong non-absorbable suture tape anchored across the repair (medial malleolus to talus/calcaneus) as a load-sharing check-rein that restrains external rotation and valgus and protects the biological repair so rehabilitation can start earlier. It is a supplement, not a replacement for anatomic repair, offered in poor-quality tissue (chronic/diabetic/revision) or high-demand athletes; evidence is limited (biomechanical/short-term), so routine use is not established and over-tensioning risks stiffness.
Surgical Technique Essentials
Operative Approach
- Medial incision over malleolus
- Protect saphenous nerve (anterior)
- Suture anchors at anatomic origins
- Repair deep layer first
- Autograft (hamstring) preferred
- Bone tunnels in malleolus
- Anatomic recreation of superficial and deep
- Neutral dorsiflexion
- 5° hindfoot inversion (NOT valgus)
- Indication
- Acute, good tissue
- Technique
- Suture anchors to malleolus
- Indication
- Chronic, poor tissue
- Technique
- Autograft through tunnels
Complications
Early Complications
Wound healing problems occur in 5-8% due to thin soft tissue envelope over medial malleolus. Risk factors include diabetes, smoking, peripheral vascular disease, and steroid use. Prevention requires careful handling of skin flaps, avoiding excessive tension on closure, and appropriate patient selection. Management ranges from local wound care to debridement and delayed closure for deeper dehiscence.
Saphenous nerve injury presents as numbness or dysesthesia along medial ankle and foot (10-15% incidence). Usually iatrogenic from surgical dissection or retractor placement. Majority are neurapraxia resolving within 3-6 months. Permanent injury occurs in less than 2% but can be debilitating. Prevention requires identification and protection of nerve during approach.
Posterior tibial neurovascular injury is rare (less than 1%) but catastrophic. Bundle lies approximately 1.5cm posterior to medial malleolus. At risk during deep dissection for deltoid reconstruction or bone tunnel creation. Presents with numbness on plantar foot, weakness of toe flexion, or vascular compromise. Prevention through careful dissection and knowledge of anatomy.
Late Complications
Stiffness and loss of motion affects 15-20% of patients following deltoid reconstruction, higher than lateral ligament procedures. Typically involves loss of dorsiflexion (average 8-12 degrees) and subtalar motion. Caused by immobilization duration, adhesion formation, or overtightening during repair. Prevention includes early motion protocols (after 2 weeks protection) and avoiding excessive tension during reconstruction. Treatment with aggressive physical therapy, occasionally manipulation under anesthesia.
Persistent instability occurs in 10-15% following reconstruction. Causes include technical failure (inadequate graft tension, tunnel malposition), unaddressed hindfoot valgus deformity, progression of PTTD, or syndesmotic insufficiency. Requires thorough re-evaluation with imaging to identify specific failure mechanism. Management may require revision reconstruction, calcaneal osteotomy, or salvage fusion procedures.
Post-traumatic arthritis develops in 20-30% of patients with deltoid injuries associated with ankle fractures or syndesmotic disruption. Risk factors include initial fracture displacement, quality of fracture reduction, articular cartilage damage, and age greater than 50 years. Presents with progressive pain and stiffness over 2-5 years. Treatment ranges from conservative measures (bracing, activity modification, injections) to ankle arthroplasty or arthrodesis in severe cases.
Rehabilitation Summary
Post-Op Protocol
Phase 1 (0-2 weeks): NWB, splint, wound care Phase 2 (2-6 weeks): Progress to 50% WB, gentle ROM Phase 3 (6-12 weeks): Full WB, strengthening, proprioception Phase 4 (3-6 months): Return to sport with brace
- Weight-Bearing
- Non-weight-bearing
- Activity
- Splint protection
- Weight-Bearing
- Progress to 50%
- Activity
- Gentle ROM in boot
- Weight-Bearing
- Full weight-bearing
- Activity
- Strengthening, proprioception
- Weight-Bearing
- Sport-specific
- Activity
- Return to play with brace
Outcomes Summary
Expected Results
- 60-70% success for isolated injuries
- 14-week average return to sport
- Higher failure with Grade 3 tears
- Primary repair: 85-90% success
- Reconstruction: 75-85% success
- Combined with PTTD: 70-80% success
- Success Rate
- 60-70%
- Notes
- Isolated injuries only
- Success Rate
- 85-90%
- Notes
- Acute, good tissue
- Success Rate
- 75-85%
- Notes
- Chronic insufficiency
Guidelines, Registries & Global Practice
Global Epidemiology
- Medial-side (deltoid) injury accounts for roughly 3-5% of ankle sprains; isolated deltoid rupture is rare (under 5% of deltoid injuries)
- Deltoid injury commonly accompanies pronation-external rotation and bimalleolar-equivalent (Weber B/C) fractures, with occult deltoid injury found in up to 72% of chronic lateral-instability surgical cohorts
- Adult acquired flatfoot (PTTD) prevalence is approximately 3-10% in adults over 40, the main driver of chronic medial peritalar instability
Side-by-Side Guidance
- Emphasis
- Restore lateral column first; intraoperative stress test of mortise/syndesmosis
- Position on Deltoid Repair
- Selective repair if medial clear space stays widened
- Emphasis
- Stability-driven fixation; recognise occult medial injury
- Position on Deltoid Repair
- Not routine; repair for persistent medial widening
- Emphasis
- Anatomic mortise reduction, early stability assessment
- Position on Deltoid Repair
- Deltoid healing via reduction; repair selectively
- Emphasis
- Increasing interest in direct repair to cut hardware burden
- Position on Deltoid Repair
- Repair a valid alternative to syndesmotic screws
Controversies and Areas of Uncertainty
Medial ankle instability is an area of low-level evidence (mostly cadaveric studies and Level III-IV series). Examiners reward a candidate who can state what is genuinely debated rather than overclaiming.
- Routine vs selective deltoid repair in ankle fractures. Whether to repair the deltoid during fracture fixation remains contested. Comparative series (Woo et al; Whitlock et al) show repair restores a smaller medial clear space and reduces reoperation, but most authorities still favour a stability-driven, selective approach, restore the lateral column and syndesmosis, then repair only if the medial clear space stays widened. No adequately powered randomised trial exists.
- Deltoid repair vs trans-syndesmotic fixation. Some evidence suggests direct deltoid repair gives equivalent function with fewer hardware-removal reoperations than syndesmotic screws, but selection bias limits conclusions and suture-button fixation has changed the comparison.
- Significance of an isolated superficial deltoid tear. Cadaveric band-specific work (Gregersen et al) indicates the deep posterior tibiotalar band is often spared in SER injuries, so a superficial tear does not necessarily mean global deltoid incompetence. Dynamic stress assessment, not static MRI signal, should drive treatment.
- Reconstruction technique and graft choice. No consensus exists on autograft vs allograft, single- vs double-bundle reconstruction, or the role of suture-tape (internal brace) augmentation; recommendations are extrapolated from anatomic and small clinical series.
- Role of weight-bearing CT. Weight-bearing CT is increasingly used to quantify hindfoot valgus and subtle peritalar subluxation, but thresholds defining pathological medial instability are not yet standardised.
- Optimal medial clear space threshold. The widely quoted 4mm cut-off and side-to-side comparison are pragmatic rather than rigorously validated, and gravity/external-rotation stress views vary in technique between centres.
MCQ Practice Points
Q: What are the components of the deltoid ligament complex?
A: Superficial deltoid: Tibionavicular, tibiospring (tibiocalcaneonavicular), tibiocalcaneal. Deep deltoid: Anterior and posterior tibiotalar ligaments. Deep deltoid is primary restraint to lateral talar shift; superficial deltoid resists eversion. Injury often associated with lateral malleolus fracture or syndesmotic injury.
Q: What is the relationship between posterior tibial tendon dysfunction and medial ankle instability?
A: Stage II-IV PTTD often involves spring ligament attenuation and medial ankle instability. The spring ligament (calcaneonavicular) is part of medial support complex. PTTD progression leads to hindfoot valgus, forefoot abduction, and increased deltoid ligament stress. Reconstruction must address both tendon and ligament insufficiency.
Q: How is medial ankle instability assessed clinically?
A: Medial talar tilt test: Eversion stress - increased tilt indicates deltoid insufficiency. External rotation stress test: Tests deep deltoid. Compare to contralateral side. Medial clear space on mortise radiograph: greater than 4-5mm indicates deltoid incompetence. Often associated with valgus ankle deformity and lateral ankle impingement.
Q: What is the role of the spring ligament in medial ankle stability?
A: Spring ligament (calcaneonavicular) supports talar head and maintains longitudinal arch. Attenuation allows talar head plantar/lateral subluxation and contributes to flatfoot deformity. Works in conjunction with deltoid ligament and PTTD. Spring ligament reconstruction often required in adult-acquired flatfoot surgery.
Q: What are the surgical options for chronic medial ankle instability?
A: Direct repair: Rarely possible due to attenuated tissue. Reconstruction: Autograft (FHL, peroneus longus) or allograft recreating deltoid anatomy. Medializing calcaneal osteotomy reduces medial ligament stress. Concurrent procedures: Lateral lengthening, spring ligament reconstruction, FDL transfer if PTTD present. Address underlying alignment.
At a Glance
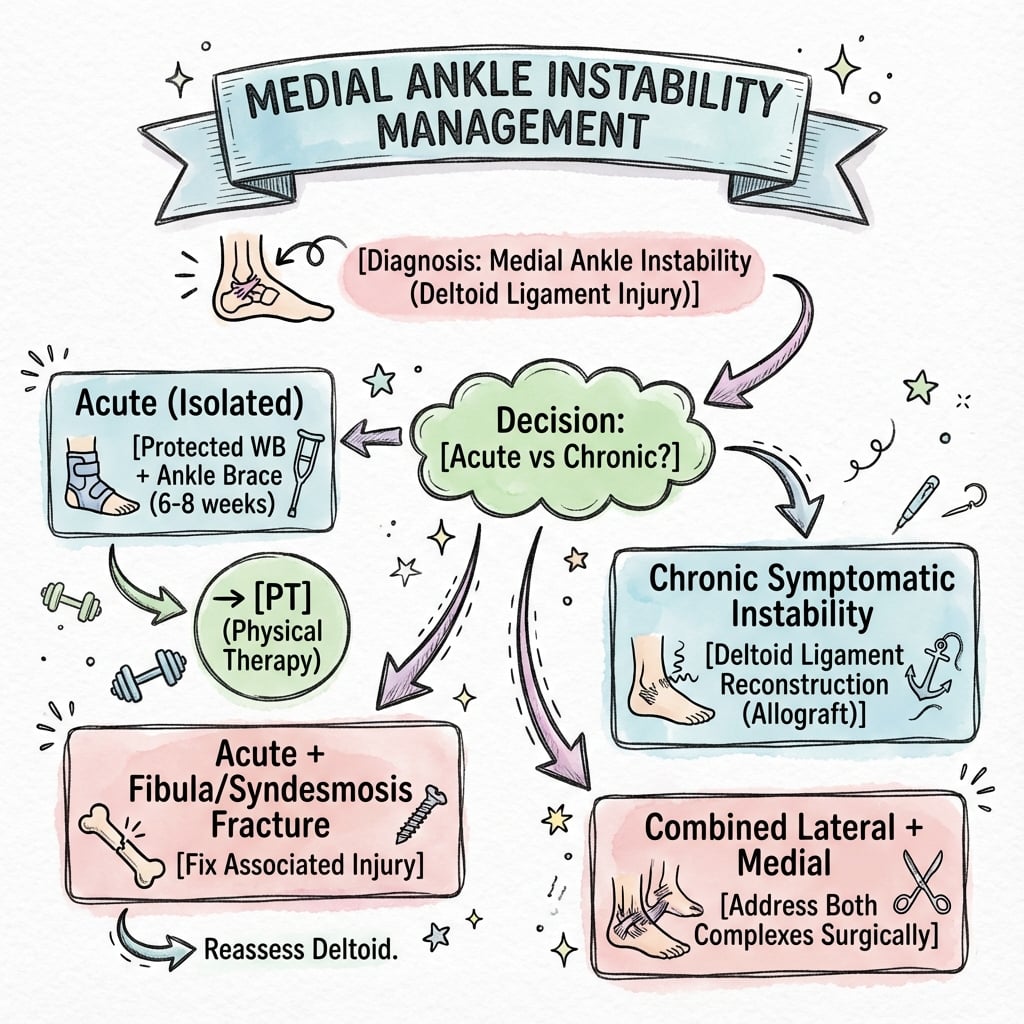
Medial ankle instability from deltoid ligament insufficiency represents only 3-5% of ankle sprains due to the ligament's significant strength (2-3x ATFL). The deltoid has superficial (hindfoot valgus restraint) and deep (external rotation and lateral talar shift restraint) components. Isolated deltoid injury is rare; most occur with syndesmotic injuries (40-60%), pronation-external rotation fractures, or stage 4 PTTD. Diagnosis requires stress radiographs showing medial clear space widening greater than 4mm or MRI demonstrating ligament discontinuity. Conservative management succeeds in 60-70%; surgical reconstruction is indicated for persistent symptomatic instability.
Mnemonic
Hook:EVEL Deltoid
The deltoid ligament resists 40% of valgus stress and is primary restraint to external rotation of the talus within the mortise. The deep posterior tibiotalar ligament prevents lateral translation of the talus, maintaining medial clear space (normal less than 4mm). Deltoid competency is essential for syndesmotic stability; deltoid insufficiency allows widening of ankle mortise even with intact syndesmosis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old rugby player sustained an ankle injury during a tackle. Radiographs show a Weber B fibular fracture and widened medial clear space (6mm). Tibiofibular clear space is 7mm. MRI confirms complete deltoid disruption and syndesmotic injury. How would you manage this patient?”
“A 58-year-old female presents with progressive flatfoot deformity and medial ankle pain over 5 years. She has valgus hindfoot, forefoot abduction, and failed conservative management including orthotics and bracing. Weight-bearing radiographs show valgus tilt of talus with medial clear space widening to 6mm. MRI shows complete PTT rupture, spring ligament attenuation, and deltoid insufficiency. No ankle arthritis present. What is your treatment approach?”
“A 26-year-old recreational soccer player reports 8 months of medial ankle pain and a sense of the ankle 'rolling inward' on planting and cutting, following a valgus injury treated as a simple sprain. Plain radiographs are reported as normal. He has failed physiotherapy. How do you evaluate and manage this patient?”
Immediate Answer Opener
- Medial ankle instability from deltoid ligament insufficiency is uncommon (3-5% of ankle sprains) but clinically significant
- Deltoid complex has superficial and deep components; deep layer critical for rotational stability and preventing lateral talar shift
- Isolated injuries are rare; most occur with syndesmotic disruption, ankle fractures, or stage 4 PTTD
- Diagnosis requires medial clear space assessment (pathologic if greater than 4mm), external rotation stress testing, and MRI
- Conservative management succeeds in 60-70% of acute isolated injuries
- Surgical treatment: primary repair for acute injuries with good tissue, or reconstruction using autograft for chronic insufficiency
Anatomy - Superficial vs Deep Deltoid
- Superficial layer: Tibionavicular, tibiocalcaneal superficial, tibiospring ligaments from anterior colliculus - restrains hindfoot valgus
- Deep layer: Anterior tibiotalar, posterior tibiotalar, tibiocalcaneal deep from intercollicular groove
- Deep layer is critical restraint to external rotation and lateral talar translation
- Deep posterior tibiotalar is strongest component and most important for stability
- Spring ligament intimately associated with superficial deltoid, often injured concurrently
Associated Injury Patterns
- Isolated deltoid (less than 5%): Rare, direct valgus force
- Deltoid plus syndesmosis (40-60%): Pronation-external rotation mechanism, most common pattern
- Ankle fractures (20-30%): Pronation-abduction with medial malleolus fracture or deltoid rupture
- Stage 4 PTTD (10-15%): Chronic valgus deformity with progressive deltoid attenuation
- Always assess for associated injuries before treating deltoid in isolation
Clinical Tests and Imaging
- External rotation stress test: Foot externally rotated with tibia stabilized, pain and increased rotation indicates deltoid injury
- Valgus stress test: Medial joint opening compared to contralateral
- Kleiger test: External rotation with ankle dorsiflexed
- Medial clear space on mortise radiograph: normal less than 4mm, pathologic if greater than 4mm or asymmetric
- Weight-bearing radiographs essential
- MRI shows grade 1 (intact with edema), grade 2 (partial tear), grade 3 (complete disruption)
Conservative vs Surgical Management
- Conservative for isolated grade 1-2 injuries: CAM boot immobilization 4-6 weeks, protected weight-bearing, strengthening and proprioception training (60-70% success)
- Surgical indications: Acute deltoid with syndesmotic injury requiring fixation, widened medial clear space despite syndesmotic reduction
- Also surgical: Chronic symptomatic instability failed 4-6 months therapy, stage 4 PTTD with progressive deformity
- Primary repair if acute with good tissue; reconstruction with autograft (hamstring) if chronic or poor quality tissue
Surgical Technique Pearls
- Medial incision protecting saphenous nerve anteriorly, PTN bundle 1.5cm posterior to malleolus
- Suture anchors at anatomic origins: anterior colliculus (superficial), intercollicular groove (deep)
- Repair deep layer first for rotational stability
- Ankle positioned in neutral dorsiflexion and 5 degrees hindfoot inversion during tie-down, NOT eversion or valgus
- Assess medial clear space after syndesmotic fixation before deciding on deltoid repair
- Spring ligament addressed if concurrent injury identified
Postoperative Protocol
- 0-2 weeks: Non-weight-bearing in splint/boot, suture removal 10-14 days
- 2-6 weeks: Progress to 50% weight-bearing in boot, begin gentle ROM avoiding forced eversion
- 6-12 weeks: Full weight-bearing in brace, progressive strengthening of tibialis posterior, proprioceptive training
- 3-6 months: Return to sport with functional testing, external bracing recommended for 12 months
- Timeline longer than lateral ligament reconstruction due to weight-bearing role
Complications and Outcomes
- Early: Saphenous nerve injury (10-15%, usually neurapraxia), wound healing problems (5-8%), PTN injury (less than 1% but catastrophic)
- Late: Stiffness and loss of motion (15-20%), persistent instability (10-15%), post-traumatic arthritis (20-30% with fractures/syndesmotic injuries)
- Outcomes: Primary repair 85-90% success, reconstruction 75-85% success
- Combined procedures with PTTD reconstruction 70-80% success
- Success rates lower than lateral ligament procedures with longer recovery
Evidence Base
Deltoid Repair vs Conservative Management During Ankle Fracture Fixation
Deltoid Repair vs Trans-syndesmotic Fixation for Bimalleolar-Equivalent Fractures
Combined Medial and Lateral Ligament Reconstruction for Chronic Rotational Instability
Prevalence of Deltoid Injury in Chronic Lateral Ankle Instability
Radiographic and Anatomic Definition of the Deltoid Ligament Complex
Deltoid-Spring (Tibiocalcaneonavicular) Reconstruction in Advanced Flatfoot
Band-Specific Anatomy and Tensioning of the Deltoid Ligament in SER Injury
AO Foundation / AAOS Principles for Medial-Side Ankle Injury
Evidence Summary
Key Evidence (this topic's cited studies)
- 78 ankle fractures with deltoid rupture; direct repair gave a smaller final medial clear space than conservative care
- With a concomitant syndesmotic injury, both medial clear space and clinical outcomes were better after repair
- 108 unstable distal fibula fractures; deltoid repair vs trans-syndesmotic vs combined fixation
- Equivalent AAOS-FAM scores; no reoperations after deltoid repair vs 26% (trans-syndesmotic) and 23% (combined), mostly hardware removal
- 81 patients with chronic rotational instability treated with combined medial (deltoid/tibiocalcaneal) and lateral anchor reconstruction
- A deep-deltoid (tibiocalcaneal) lesion accompanied the lateral injury in 67; AOFAS rose and VAS fell significantly, sustained at 12 months
- Key Finding
- Deltoid repair restores a smaller medial clear space, especially with syndesmotic injury
- Level
- Level 3
- Key Finding
- Deltoid repair gives equivalent function with far fewer reoperations than syndesmotic screws
- Level
- Level 3
- Key Finding
- Occult deltoid injury in 72% of chronic lateral instability
- Level
- Level 4
- Key Finding
- Deep posterior tibiotalar band often spared in SER fractures
- Level
- Level 5