Localisation | Dermatome vs Territory | Myotome vs Muscle | EMG/NCS Patterns
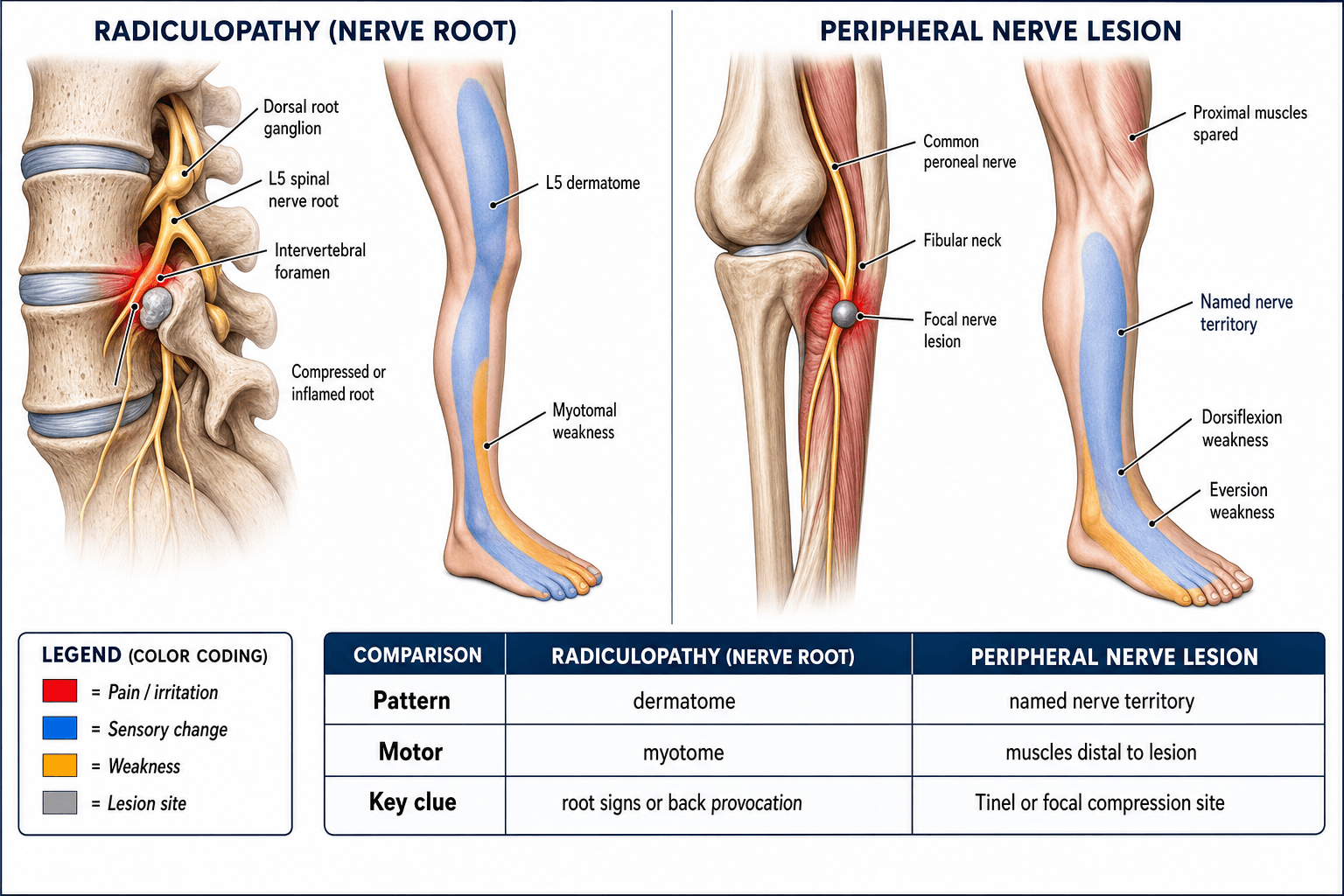
- Radiculopathy causes dermatomal sensory change; peripheral nerve lesions follow the named nerve territory
- Root lesions spare the paraspinal muscles on EMG only if purely peripheral; if paraspinals are involved the lesion is at or proximal to the root level
- Reflex loss is root-specific (biceps = C5/C6, triceps = C7, patellar = L3/L4, Achilles = S1)
- Plexus lesions affect multiple dermatomes and myotomes simultaneously but do not cause spinal pain on extension
- EMG shows fibrillations in paraspinals with radiculopathy (proximal to dorsal root ganglion if preganglionic)
- “If the sensory loss crosses a peripheral nerve boundary, think ROOT or PLEXUS
- “A pure motor deficit without sensory loss suggests a motor-nerve or anterior horn cell lesion
- “In a preganglionic radiculopathy the dorsal root ganglion is spared, so sensory NCS are NORMAL
- “Upper limb: C5 = deltoid/shoulder, C6 = biceps/radial wrist extensors, C7 = triceps/wrist flexors, C8 = finger flexors, T1 = intrinsic hand
Dermatomal sensory loss (band-like). Myotomal weakness (multiple muscles sharing a root). Reflex loss at the specific root level. Pain worse with spinal extension or Valsalva. Paraspinal fibrillation on EMG. Sensory NCS typically normal (dorsal root ganglion spared in preganglionic lesions).
Named nerve territory sensory loss (e.g., median nerve palmar digits). Weakness in muscles supplied by that nerve only. Reflexes may be normal (most reflexes are polysegmental). Tinel sign over the nerve. Sensory NCS abnormal (lesion is distal to dorsal root ganglion).
Multi-dermatomal sensory loss crossing root boundaries. Weakness across multiple myotomes supplied by different cords/trunk. Often severe pain. History of trauma, tumour, or radiation. EMG shows involvement across multiple peripheral nerves with sparing of paraspinal muscles (lesion is distal to the root).
Paraspinal EMG: Fibrillations in paraspinals = radiculopathy (lesion proximal to the dorsal root ganglion). Normal paraspinals with peripheral nerve EMG changes = plexus or peripheral nerve lesion. Sensory nerve action potentials (SNAPs): Normal in radiculopathy, reduced in peripheral nerve/plexus lesions.
- Radiculopathy
- Dermatomal (band-like)
- Plexus Lesion
- Multi-dermatomal
- Peripheral Nerve
- Single nerve territory
- Radiculopathy
- Myotomal (multiple muscles, one root)
- Plexus Lesion
- Multiple nerves affected
- Peripheral Nerve
- Single nerve muscles only
- Radiculopathy
- Root-specific reflex lost
- Plexus Lesion
- Variable (depends on cords affected)
- Peripheral Nerve
- Usually preserved
- Radiculopathy
- Normal (preganglionic)
- Plexus Lesion
- Abnormal (postganglionic)
- Peripheral Nerve
- Abnormal (postganglionic)
- Radiculopathy
- Abnormal (fibrillations)
- Plexus Lesion
- Normal (sparing)
- Peripheral Nerve
- Normal (sparing)
DAMPRoot vs Peripheral Nerve Localisation
Hook:DAMP the signal — Dermatomal, Anatomy of reflex, Myotomal, Paraspinal EMG to localise any neuropathy!
BALTTUpper Limb Myotome Quick Reference
Hook:BALTT — from proximal to distal: Biceps(C5/6), Abduct(C5), Long extensors(C7), Thumb flex(C8), Thenar(T1)!
HKSFGLower Limb Myotome Quick Reference
Hook:HKSFG — Hip(L2/3), Knee(L3/4), Supination/dorsiflex(L4/5), Foot evert(L5/S1), Gastroc(S1/2)!
Overview and Epidemiology
Distinguishing radiculopathy from peripheral nerve entrapment is one of the most commonly tested localisation problems in orthopaedic and neurology examinations. Misdiagnosis leads to wrong investigations (MRI spine vs nerve conduction studies) and wrong treatment (decompression surgery at the wrong site). A structured approach using dermatomal mapping, reflex examination, and electrodiagnostic correlation is essential.
- Cervical radiculopathy vs carpal tunnel: Both cause hand tingling; wrong site injection or surgery
- Lumbar radiculopathy vs peroneal neuropathy: Both cause foot drop; wrong surgical target
- C5 radiculopathy vs axillary neuropathy: Both cause deltoid weakness; wrong MRI level
- Root avulsion vs brachial plexus injury: Prognosis and surgical planning differ fundamentally
- Cervical radiculopathy: Annual incidence approximately 83 per 100,000; C7 is the most common root affected
- Lumbar radiculopathy: Lifetime prevalence around 1-5 percent; L5 and S1 most commonly affected
- Carpal tunnel syndrome: Most common peripheral nerve entrapment (median nerve at wrist), prevalence approximately 3-6 percent
- Peroneal neuropathy: Most common lower limb mononeuropathy, usually at fibular neck
Pathophysiology
The dorsal root ganglion (DRG) sits within the intervertebral foramen. Its position determines the pattern on sensory nerve conduction studies:
Preganglionic lesion (root compression inside the spinal canal, proximal to the DRG): The sensory cell body in the DRG is intact, so the distal sensory axon survives. Sensory nerve action potentials (SNAPs) remain normal despite clinical sensory loss.
Postganglionic lesion (plexus or peripheral nerve, distal to the DRG): The sensory axon is disconnected from its cell body. Wallerian degeneration occurs. SNAPs are reduced or absent.
This is the single most important electrophysiological discriminator between radiculopathy and peripheral nerve or plexus lesions.
- Mechanism
- Disc herniation, foraminal stenosis, tumour compressing root
- Structures Affected
- Ventral and/or dorsal root, proximal to DRG
- Electrodiagnostic Signature
- Normal SNAPs, abnormal needle EMG in myotomal distribution including paraspinals
- Mechanism
- Trauma, tumour infiltration, radiation plexopathy, neuralgic amyotrophy
- Structures Affected
- Trunks, divisions, or cords distal to DRG
- Electrodiagnostic Signature
- Abnormal SNAPs in affected dermatomes, abnormal EMG in multiple peripheral nerves, paraspinals spared
- Mechanism
- Entrapment, compression, laceration, metabolic neuropathy
- Structures Affected
- Single named nerve distal to DRG
- Electrodiagnostic Signature
- Abnormal SNAP in nerve territory, abnormal motor NCS in that nerve, EMG changes limited to that nerve's muscles
Dorsal root: Carries sensory information. Compression causes dermatomal pain, paraesthesia, and numbness in a band distribution.
Ventral root: Carries motor fibres. Compression causes myotomal weakness, fasciculations, and eventually atrophy.
Clinical radiculopathy usually involves both roots (mixed sensorimotor), but isolated motor or sensory radiculopathy can occur.
Day 0-3: Axon discontinuity but distal segment still conducts (NCS may be normal early)
Day 7-10: Distal axon begins to degenerate; fibrillation potentials appear on EMG
Day 14-21: Full Wallerian degeneration; CMAP and SNAP amplitudes drop in peripheral nerve lesions
Clinical implication: EMG/NCS performed too early (under 3 weeks) may be falsely reassuring
Classification and Types


Cervical Root vs Peripheral Nerve Patterns
- If Root Lesion
- C5 radiculopathy (deltoid + supraspinatus + biceps)
- If Peripheral Nerve
- Axillary neuropathy (deltoid only, supraspinatus spared)
- Key Discriminator
- Supraspinatus innervated by suprascapular nerve (C5/6 root) but not by axillary nerve — if supraspinatus is weak, think root not axillary nerve
- If Root Lesion
- C5/C6 radiculopathy (biceps + brachioradialis + supinator)
- If Peripheral Nerve
- Musculocutaneous neuropathy (biceps + brachialis only)
- Key Discriminator
- Brachioradialis (radial nerve) weakness = root, not musculocutaneous
- If Root Lesion
- C7 radiculopathy (triceps + wrist extensors + finger extensors)
- If Peripheral Nerve
- Radial neuropathy (posterior interosseous nerve or radial nerve at spiral groove)
- Key Discriminator
- Triceps involvement and sensory loss over dorsum of hand = C7 root; PIN spares triceps and has no sensory loss
- If Root Lesion
- C6 radiculopathy (lateral forearm + thumb + index)
- If Peripheral Nerve
- Median neuropathy (palmar thumb, index, middle; spares dorsal thumb)
- Key Discriminator
- Dorsal thumb numbness = C6 root (lateral cutaneous nerve of forearm, a sensory branch of radial nerve territory)
- If Root Lesion
- C8/T1 radiculopathy (all intrinsics + finger flexors)
- If Peripheral Nerve
- Ulnar neuropathy (interossei + hypothenar; thenar spared)
- Key Discriminator
- Thenar eminence weakness (median/thenar branch) plus interossei weakness = C8/T1 root, not ulnar nerve alone
Clinical Assessment
- Root: Neck or back pain radiating to limb, worse with extension or Valsalva, dermatomal pattern of tingling
- Peripheral nerve: Numbness in a specific nerve territory, positional provocation (e.g., elbow flexion for ulnar nerve), nocturnal symptoms (carpal tunnel)
- Plexus: Severe limb pain, history of trauma, radiation exposure, mass in supraclavicular or axillary region, multi-territory symptoms
- Map sensory loss: Is it dermatomal (band) or peripheral nerve (named territory)?
- Test individual muscles: Does weakness cross nerve boundaries? (Myotomal = root)
- Check reflexes: Biceps (C5/C6), brachioradialis (C6), triceps (C7), patellar (L3/L4), Achilles (S1)
- Provocative tests: Spurling (root), Tinel/Phalen (peripheral nerve), Adson (thoracic outlet)
Reflexes are the fastest bedside localisation tool because they are root-specific:
Upper limb:
- Biceps reflex = C5/C6 (musculocutaneous nerve)
- Brachioradialis reflex = C5/C6 (radial nerve)
- Triceps reflex = C7 (radial nerve)
- Finger jerk = C8 (median and ulnar nerves)
Lower limb:
- Patellar reflex = L3/L4 (femoral nerve)
- Posterior tibial reflex = L5 (tibial nerve) — often difficult to elicit
- Achilles reflex = S1 (tibial nerve)
A lost reflex narrows the root level. If the reflex is intact, the root is likely not severely compressed (though mild radiculopathy can spare reflexes).
- Key Muscle (Myotome)
- Deltoid (shoulder abduction)
- Reflex
- No specific reflex (biceps is C5/C6)
- Sensory (Dermatome)
- Lateral upper arm (regimental badge area)
- Key Muscle (Myotome)
- Biceps, brachioradialis (elbow flexion, wrist extension)
- Reflex
- Biceps and brachioradialis reflex
- Sensory (Dermatome)
- Lateral forearm, thumb, index finger
- Key Muscle (Myotome)
- Triceps, wrist extensors, wrist flexors (elbow extension, wrist movement)
- Reflex
- Triceps reflex
- Sensory (Dermatome)
- Middle finger, dorsal hand
- Key Muscle (Myotome)
- Finger flexors, extensors (grip)
- Reflex
- Finger jerk
- Sensory (Dermatome)
- Medial forearm, ring and little finger
- Key Muscle (Myotome)
- Interossei, thenar muscles (intrinsics)
- Reflex
- No specific reflex
- Sensory (Dermatome)
- Medial arm (above elbow)
- Key Muscle (Myotome)
- Tibialis anterior (ankle dorsiflexion, inversion)
- Reflex
- Patellar reflex
- Sensory (Dermatome)
- Medial leg and ankle
- Key Muscle (Myotome)
- Extensor hallucis longus (great toe extension), hip abduction
- Reflex
- Posterior tibial (often absent normally)
- Sensory (Dermatome)
- Lateral leg, dorsum of foot
- Key Muscle (Myotome)
- Gastrocnemius/soleus (plantarflexion), peronei (eversion)
- Reflex
- Achilles reflex
- Sensory (Dermatome)
- Lateral foot, lateral sole
C6 radiculopathy vs carpal tunnel syndrome: Both cause thumb and index finger tingling. In carpal tunnel, the dorsal thumb is spared (palmar digital branch affected, dorsal digital branch from radial nerve enters distal to tunnel). In C6 radiculopathy, the dorsal thumb is also affected. Check thenar eminence strength (abductor pollicis brevis = median = affected in both) versus brachioradialis strength (radial nerve, C5/C6 = affected only in radiculopathy).
L5 radiculopathy vs peroneal neuropathy: Both cause foot drop. In peroneal neuropathy, hip abduction (gluteus medius) and foot inversion (tibialis posterior) are spared (tibial nerve, L4/L5 root). In L5 radiculopathy, these are weak because the L5 root supplies the superior gluteal nerve (gluteus medius) and contributes to the tibial nerve (tibialis posterior).
The topic names the Adson manoeuvre but the lower-plexus mimic it screens for deserves a full answer, because true neurogenic thoracic outlet syndrome (TOS) is the classic trap for "C8/T1 radiculopathy or ulnar neuropathy" that is really a lower-trunk plexus lesion:
- Mechanism: a cervical rib or a fibrous band from an elongated C7 transverse process tents and angulates the lower trunk (C8 more than T1) of the brachial plexus.
- The Gilliatt-Sumner hand: the hallmark pattern of wasting is thenar (abductor pollicis brevis) greater than hypothenar, because the lesion preferentially affects the T1-to-C8 fibres destined for the median-innervated thenar muscles - this is the opposite of what an ulnar neuropathy would give and a key discriminator.
- Sensory: numbness along the medial forearm and hand in the C8/T1 / lower-trunk territory; the medial antebrachial cutaneous (MABC) nerve SNAP is abnormal (postganglionic, distal to the DRG) - a useful electrodiagnostic clue that distinguishes it from a preganglionic C8/T1 root lesion (where SNAPs would be normal).
- Confirm: chest/cervical radiograph and CT/MRI for a cervical rib or band; nerve conduction showing a low median CMAP/ulnar SNAP with the abnormal MABC SNAP. Treat by resecting the rib/band and decompressing the plexus.
- Caution: true neurogenic TOS is rare; the far commoner "disputed/non-specific" TOS has no objective neurological or electrodiagnostic findings and provocative tests (Adson, Roos) are non-specific - do not over-diagnose structural TOS on a positive Adson alone.
Exam point: thenar-predominant wasting (Gilliatt-Sumner hand) + an abnormal MABC SNAP + a cervical rib localises to the lower trunk of the brachial plexus, not to a C8/T1 root or the ulnar nerve.
Investigations
Investigation Protocol
Map sensory loss: Draw the area of numbness on the patient — compare to dermatome maps and peripheral nerve territory maps
Test individual muscles: Identify which muscles are weak and which are strong — does the pattern cross nerve boundaries?
Check reflexes: Lost reflex = root level localisation
Provocative tests: Spurling (cervical root), straight leg raise (lumbar root), Tinel (peripheral nerve)
Timing: Wait at least 3-4 weeks after onset for reliable EMG findings (fibrillations take time to develop)
Sensory NCS: Normal SNAP in radiculopathy (preganglionic), abnormal in peripheral nerve/plexus (postganglionic)
Motor NCS: May show reduced CMAP in peripheral nerve lesions; often normal in radiculopathy unless severe
Needle EMG: Fibrillations and positive sharp waves in affected muscles. Paraspinal involvement = radiculopathy. Distribution across root vs peripheral nerve pattern clinches the diagnosis
Cervical/lumbar spine MRI: For suspected radiculopathy — look for disc herniation, foraminal stenosis, root compression
Brachial plexus MRI: For suspected plexus lesion — look for tumour, traumatic injury, inflammation
Peripheral nerve ultrasound or MRI: For suspected entrapment — structural cause (ganglion, lipoma, fibrous band)
The most common exam trap is ordering EMG too early (under 3 weeks). Before Wallerian degeneration is complete, the EMG may be normal or show only reduced recruitment without fibrillation potentials. Fibrillations appear at 10-21 days. The exam answer is always to wait 3-4 weeks before EMG for radiculopathy.
- Radiculopathy
- Normal (DRG spared)
- Plexus Lesion
- Reduced or absent (postganglionic)
- Peripheral Nerve
- Reduced or absent in affected nerve
- Radiculopathy
- Usually normal (may be reduced in severe cases)
- Plexus Lesion
- Reduced in affected peripheral nerves
- Peripheral Nerve
- Reduced in the affected nerve only
- Radiculopathy
- Fibrillations present
- Plexus Lesion
- Normal (sparing)
- Peripheral Nerve
- Normal (sparing)
- Radiculopathy
- Myotomal (e.g., C5 muscles: deltoid, biceps, brachioradialis)
- Plexus Lesion
- Multi-nerve (e.g., upper trunk: muscles from both median and radial in C5/C6 distribution)
- Peripheral Nerve
- Single nerve (e.g., median nerve muscles only)
The standard EMG/NCS battery above interrogates the distal nerve and the muscle, but the late responses are the part of the study that samples the proximal segment and the root - the very region a radiculopathy lives in - and they are frequently asked about:
- F-wave: a late muscle response produced when the stimulus travels antidromically up the motor axon to the anterior horn cell and back down. It tests the whole motor pathway including the proximal root. In radiculopathy the F-wave latency may be prolonged or the F-wave may show reduced persistence/chronodispersion, but F-waves are non-specific (they sample many roots, so a single-root lesion is often diluted) and are most useful for diffuse processes such as Guillain-Barre.
- H-reflex: the electrophysiological equivalent of the ankle (Achilles) reflex - a true monosynaptic reflex (Ia afferent to alpha motor neuron) recorded from soleus/gastrocnemius after tibial nerve stimulation. It is the single best NCS for the S1 root: a prolonged or absent H-reflex (compared side to side) is an early, sensitive sign of S1 radiculopathy, and unlike needle EMG it is abnormal immediately (it does not wait the three weeks for fibrillations). Its limitations are that it is non-localising (an S1 lesion anywhere along the arc abolishes it), it cannot be repeated reliably once abolished, and it normally disappears with age/peripheral neuropathy.
Exam point: when an S1 radiculopathy is suspected acutely (before fibrillations appear), the H-reflex is the test that can already be abnormal; the F-wave assesses proximal conduction but is too non-specific to localise a single root.
Management Algorithm
Management of Nerve Root Compression
Treatment Protocol
Analgesia: NSAIDs, neuropathic agents (gabapentin, pregabalin, duloxetine)
Physical therapy: Core stabilisation, postural correction, neural glide exercises
Activity modification: Avoid provocative postures, heavy lifting
Corticosteroid injection: Selective nerve root block or epidural for refractory pain (evidence supports short-term relief)
Progressive neurological deficit: Worsening weakness, developing myelopathy signs
Cauda equina syndrome: Emergency — saddle anaesthesia, bladder/bowel dysfunction
Severe refractory pain: Pain unresponsive to 6-12 weeks of conservative treatment with concordant imaging
Disc herniation with concordant radiculopathy: When clinical level matches imaging level
Cervical: Anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty, posterior foraminotomy
Lumbar: Microdiscectomy (disc herniation), decompressive laminectomy (stenosis), foraminotomy (foraminal stenosis)
Outcomes: 80-95 percent good-to-excellent results when clinical and imaging levels correlate
Emergency decompression is indicated for cauda equina syndrome (saddle anaesthesia, urinary retention) or progressive myelopathy. Otherwise, 6-12 weeks of conservative treatment is appropriate before considering surgery, as many radiculopathies resolve spontaneously.
Complications
- When It Occurs
- Following any nerve injury; radiculopathy or peripheral nerve
- Risk Factors
- Severe initial pain, psychological comorbidity, delayed treatment
- Management
- Multimodal analgesia (gabapentinoids, SNRIs, CBT, pain clinic referral)
- When It Occurs
- After 12-18 months of denervation without reinnervation
- Risk Factors
- Complete axonal loss, proximal lesions, long distance to target muscle
- Management
- Prevention via early decompression; tendon transfers for established cases
- When It Occurs
- After peripheral nerve injury or surgery
- Risk Factors
- Immobilisation, female sex, upper limb injuries
- Management
- Early mobilisation, bisphosphonates, sympathetic blocks
- When It Occurs
- Following carpal tunnel or cubital tunnel release
- Risk Factors
- Severe pre-operative denervation, prolonged symptoms, older age
- Management
- Set expectations pre-operatively; tendon transfer if functional deficit persists
- When It Occurs
- Compression at two sites along one nerve (e.g., cervical root + carpal tunnel)
- Risk Factors
- Metabolic neuropathy (diabetes), multiple entrapment points
- Management
- Address both sites; treat the more accessible one first
A nerve compressed at one site becomes more susceptible to compression at a second site along its course due to impaired axoplasmic transport. Clinically, a patient may have both a C6/C7 radiculopathy AND carpal tunnel syndrome. Both may need treatment. Always consider proximal and distal compression sites when the clinical picture does not fit a single localisation.
Outcomes and Prognosis
- Treatment
- Conservative (6-12 weeks) or microdiscectomy
- Expected Outcome
- 80-90 percent improve with conservative care; surgery faster relief at 1 year equivalent
- Long-term Function
- Good return to activity; recurrence 5-10 percent
- Treatment
- Conservative or ACDF
- Expected Outcome
- 70-90 percent improve with conservative care; surgery 80-95 percent good results
- Long-term Function
- Good long-term; adjacent segment disease 2-3 percent per year post-fusion
- Treatment
- Splinting, injection, or surgical release
- Expected Outcome
- Surgical release: 90 percent good-to-excellent; conservative: 50-70 percent improve
- Long-term Function
- Excellent long-term after surgery; grip strength returns 3-6 months
- Treatment
- Nerve graft or transfer
- Expected Outcome
- 60-80 percent achieve useful shoulder and elbow function
- Long-term Function
- Hand function often incomplete; long rehabilitation 2-3 years
- Treatment
- Nerve transfers (accessory to suprascapular, ulnar fascicle to biceps)
- Expected Outcome
- 40-60 percent achieve useful function with nerve transfer
- Long-term Function
- Full recovery rare; focus on shoulder stability and elbow flexion
Best prognosis: Acute presentation, short duration of symptoms, partial (not complete) lesion, distal entrapment site, younger age, no comorbid neuropathy
Poor prognosis: Root avulsion (preganglionic), complete axonal loss on EMG, duration over 12 months before intervention, proximal lesions (longer regeneration distance), diabetes or other neuropathy
Key threshold: Muscles must be reinnervated within 12-18 months. After this window, motor end plates degenerate irreversibly and tendon transfers become the only option.
Guidelines, Registries & Global Practice
- Cervical radiculopathy: Annual incidence approximately 83 per 100,000 population globally, peaking in the 5th decade
- Lumbar radiculopathy: Lifetime prevalence approximately 1-5 percent; L5 and S1 account for the majority
- Carpal tunnel syndrome: Most common entrapment neuropathy worldwide; prevalence approximately 3-6 percent; higher in occupations with repetitive wrist loading
- Peroneal neuropathy: Most common lower limb mononeuropathy; often related to prolonged bed rest, leg crossing, or lithotomy positioning
- High-resource: EMG/NCS readily available; MRI first-line imaging; early surgical decompression for refractory cases
- Limited-resource: Clinical localisation paramount (imaging may not be available); bedside examination carries the diagnosis; ultrasound-guided nerve blocks where available
- Universal principle: Accurate clinical localisation through structured sensory mapping, individual muscle testing, and reflex examination is the foundation regardless of available technology
- Electrodiagnostic access: EMG/NCS is the gold standard but is not universally available; in its absence, careful clinical examination remains diagnostic
- Diagnosis emphasis
- EMG/NCS gold standard for localisation; SNAPs and paraspinal EMG are key discriminators
- Imaging
- MRI for structural correlation; CT myelography for root avulsion
- Treatment approach
- Electrodiagnostic localisation guides whether to operate on spine, plexus, or peripheral nerve
- Diagnosis emphasis
- Clinical assessment first; imaging for refractory or progressive cases
- Imaging
- MRI spine for radiculopathy not responding to 6 weeks conservative care
- Treatment approach
- Conservative first; surgery for progressive deficit, cauda equina, or refractory pain
- Diagnosis emphasis
- Structured clinical examination with validated outcome measures
- Imaging
- MRI when surgery contemplated; EMG when diagnosis uncertain
- Treatment approach
- Shared decision-making for disc herniation; evidence supports both conservative and surgical outcomes
- Diagnosis emphasis
- Clear imaging-based classification of disc herniation and stenosis patterns
- Imaging
- CT for bony anatomy; MRI for soft tissue and neural element assessment
- Treatment approach
- Standardised surgical technique for microdiscectomy and decompression
There is no single global registry for radiculopathy or peripheral nerve entrapment outcomes. SPORT (Spine Patient Outcomes Research Trial) provides the highest-quality comparative data for lumbar radiculopathy management. For carpal tunnel syndrome, multiple national hand surgery audit datasets (including the British Society for Surgery of the Hand) demonstrate consistently good outcomes after surgical release. The evidence base for plexus injury management relies heavily on specialist centre case series rather than randomised trials.
Record in every nerve localisation assessment:
- Sensory map drawn and described (dermatomal vs peripheral nerve territory)
- Individual muscle strength testing (Medical Research Council grading) for key discriminator muscles
- Reflexes documented (present, absent, or diminished — compared to contralateral)
- Clinical localisation stated with reasoning (root level or specific peripheral nerve)
- EMG/NCS findings correlated with clinical examination when available
Mislocalisation leading to wrong-site surgery is a significant medico-legal risk worldwide. Always document your clinical reasoning and ensure electrodiagnostic correlation before operative intervention.
Controversies & Areas of Uncertainty
The concept that proximal nerve compression predisposes to distal entrapment via impaired axoplasmic transport is clinically appealing and experimentally supported, but its prevalence and clinical significance remain debated. Some argue most apparent double crush cases represent two independent entrapments in a susceptible nerve. Treatment should address both sites when clinically indicated.
While the standard recommendation is to wait 3-4 weeks for fibrillation potentials to develop, early EMG (within 1-2 weeks) may still show reduced recruitment patterns that suggest the diagnosis. Some electromyographers advocate early study for baseline, with repeat at 3-4 weeks if the initial study is non-diagnostic. No consensus guideline mandates a minimum waiting period.
Long-term outcomes (2-4 years) of SPORT show convergence between surgical and conservative groups, suggesting that surgery accelerates recovery but may not change the final outcome. However, patient selection, severity of compression, and duration of symptoms all influence this balance. Shared decision-making based on individual patient factors is the current standard.
Nerve transfers (neurotisation) have increasingly replaced nerve grafts for root avulsions, with growing evidence of superior outcomes for shoulder and elbow function when performed within 6 months. However, long-term comparative data remain limited, and the choice between transfers, grafts, and combined approaches varies by surgeon experience and the specific injury pattern.
MCQ Practice Points
Q: A patient has weakness of deltoid, biceps, and brachioradialis with normal triceps. Sensory loss is over the lateral arm and forearm. Biceps reflex is absent. What is the localisation? A: C5/C6 radiculopathy. The weakness crosses peripheral nerve boundaries (deltoid = axillary nerve, biceps = musculocutaneous nerve, brachioradialis = radial nerve) but shares the C5/C6 myotome. The absent biceps reflex (C5/C6) confirms the root level. A single peripheral nerve cannot explain weakness across three different nerves.
Q: A patient has weakness and sensory loss in an L5 distribution. EMG shows fibrillation in the tibialis anterior, EHL, and gluteus medius. The superficial peroneal SNAP is normal. Paraspinal EMG at L5 shows fibrillation. What is the diagnosis? A: L5 radiculopathy. The normal SNAP (preganglionic — DRG spared) combined with paraspinal fibrillation confirms a root lesion. If this were a peroneal neuropathy, the superficial peroneal SNAP would be abnormal and the paraspinals would be normal.
Q: A patient has weakness of shoulder abduction, elbow flexion, and external rotation. Sensory loss covers the lateral arm and forearm. SNAPs are reduced in the lateral cutaneous nerve of the forearm. Paraspinal EMG is normal. What is the localisation? A: Upper trunk brachial plexus lesion. The weakness involves C5/C6 muscles but crosses multiple peripheral nerves. The abnormal SNAPs indicate a postganglionic lesion (distal to DRG). The normal paraspinal EMG excludes radiculopathy. This combination — C5/C6 myotomal distribution with abnormal SNAPs and normal paraspinals — localises to the upper trunk of the brachial plexus.
Q: A patient has foot drop with weak tibialis anterior and EHL but normal ankle inversion, normal hip abduction, and normal sensation over the lateral leg. What is the most likely diagnosis? A: Common peroneal neuropathy at the fibular neck. The weakness is limited to dorsiflexion and toe extension (deep peroneal nerve) without involvement of tibial nerve muscles (inversion) or superior gluteal nerve muscles (hip abduction). Sensation over the lateral leg is normal (superficial peroneal sensory may or may not be affected depending on the exact level).
Q: A patient develops acute C7 radiculopathy. When is the optimal time to perform EMG for diagnostic purposes? A: 3-4 weeks after symptom onset. Fibrillation potentials (the hallmark of active denervation) take 10-21 days to develop. EMG performed too early may be falsely normal. Motor NCS and SNAP changes may also be absent in the first few weeks.
Q: A trauma patient has a flail arm with loss of all limb sensation and weakness. Horner syndrome is present. SNAPs are normal. What is the localisation? A: C8/T1 root avulsion (preganglionic). Horner syndrome indicates disruption of the cervical sympathetic chain, which lies adjacent to the C8/T1 roots. Normal SNAPs confirm a preganglionic lesion. Root avulsion is the most severe form of preganglionic injury and requires nerve transfer rather than grafting.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with a 3-week history of right foot drop. He reports lower back pain radiating to the lateral aspect of his right leg. Examination reveals weakness of ankle dorsiflexion (3/5), great toe extension (2/5), ankle eversion (3/5), ankle inversion (4+/5), and hip abduction (4/5). There is reduced sensation over the lateral leg and dorsum of the foot. The Achilles reflex is diminished on the right. How do you localise this lesion and what investigations would you order?”
“A 40-year-old woman presents with a 2-month history of numbness and tingling in her right thumb, index, and middle fingers, worse at night. She also reports neck pain on the right side. Examination shows weak thumb abduction (4/5), weak opposition (4/5), with normal brachioradialis, triceps, and deltoid strength. Sensory loss is confined to the palmar aspect of the thumb, index, and middle fingers. Tinel sign is positive at the wrist. The biceps and triceps reflexes are normal. What is your diagnosis and how would you manage this?”
Localisation Hierarchy
- Root = dermatomal sensory loss, myotomal weakness, root-specific reflex loss, normal SNAPs, paraspinal EMG abnormal
- Plexus = multi-dermatomal, multi-nerve involvement, abnormal SNAPs, paraspinal EMG normal
- Peripheral nerve = single nerve territory sensory loss, single nerve muscle weakness, abnormal SNAPs, paraspinal EMG normal
Key Discriminators
- Hip abduction weakness (gluteus medius) with foot drop = L5 root, not peroneal nerve
- Dorsal thumb numbness with hand tingling = C6 root, not carpal tunnel
- Supraspinatus weakness with deltoid weakness = C5 root, not axillary nerve
- Brachioradialis weakness with biceps weakness = C5/C6 root, not musculocutaneous nerve
EMG/NCS Rules
- SNAPs normal in radiculopathy (preganglionic), abnormal in plexus and peripheral nerve (postganglionic)
- Paraspinal fibrillations = root lesion; normal paraspinals = plexus or peripheral nerve
- Wait 3-4 weeks after onset for reliable EMG (fibrillations take 10-21 days to appear)
- Myotomal EMG pattern across different nerves confirms radiculopathy
Upper Limb Myotomes
- C5 = deltoid, supraspinatus (shoulder abduction), biceps reflex (C5/C6)
- C6 = biceps, brachioradialis, wrist extensors (elbow flexion, wrist extension)
- C7 = triceps, wrist flexors, wrist extensors (elbow extension, triceps reflex)
- C8 = finger flexors, extensors (grip, finger jerk)
- T1 = interossei, thenar muscles (intrinsic hand function)
Lower Limb Myotomes
- L2/L3 = iliopsoas (hip flexion)
- L3/L4 = quadriceps (knee extension, patellar reflex)
- L4/L5 = tibialis anterior (ankle dorsiflexion, inversion)
- L5 = EHL (great toe extension), gluteus medius (hip abduction)
- S1 = gastrocnemius/soleus (plantarflexion, Achilles reflex), peronei (eversion)
Red Flags and Pitfalls
- Horner syndrome with upper limb palsy = C8/T1 root avulsion (preganglionic)
- Cauda equina syndrome = emergency decompression (saddle anaesthesia, urinary retention)
- Double crush: always check both proximal and distal when one localisation does not explain all findings
- Normal MRI does not exclude radiculopathy — EMG is more sensitive for nerve root involvement
Evidence Base and Key Trials
Cervical radiculopathies: comparison of surgical and EMG localization of single-root lesions
- 50 surgically proven single-root cervical lesions correlated with needle-EMG patterns (study graded abnormal only by fibrillation potentials)
- Each root produced a relatively stereotyped myotomal EMG pattern (C7 commonest at 56 percent); C6 was the most variable
- Needle EMG with paraspinal sampling localised the lesion to the root level
Identifying lumbosacral radiculopathies: an optimal electromyographic screen
- Prospective multicentre study of 102 electrodiagnostically confirmed lumbosacral radiculopathies
- A six-muscle screen that INCLUDES paraspinal muscles identified 98-100 percent of radiculopathies
- Without paraspinals, eight distal muscles were needed to reach only ~90 percent identification