Resistance to PTH - and the Short Metacarpal
- Pseudohypoparathyroidism (PHP) is END-ORGAN RESISTANCE to PARATHYROID HORMONE: the parathyroid glands work and secrete PTH, but the kidney and bone do not respond, so the biochemical hallmark is HYPOCALCAEMIA and HYPERPHOSPHATAEMIA with a HIGH (not low) PTH - the opposite of true hypoparathyroidism (where PTH is low).
- The defect is in GNAS, which encodes the alpha subunit of the stimulatory G protein (Gs-alpha) that couples the PTH receptor to adenylate cyclase/cAMP; because GNAS is an IMPRINTED gene, the PARENT OF ORIGIN of the mutation determines the phenotype.
- PHP type 1a (MATERNALLY inherited Gs-alpha loss) gives the ALBRIGHT HEREDITARY OSTEODYSTROPHY (AHO) phenotype PLUS resistance to multiple hormones (PTH, and also TSH causing hypothyroidism, and gonadotropins); PSEUDO-PSEUDOHYPOPARATHYROIDISM (PPHP, PATERNALLY inherited) gives the same AHO physical phenotype but WITHOUT hormone resistance (normal calcium and PTH).
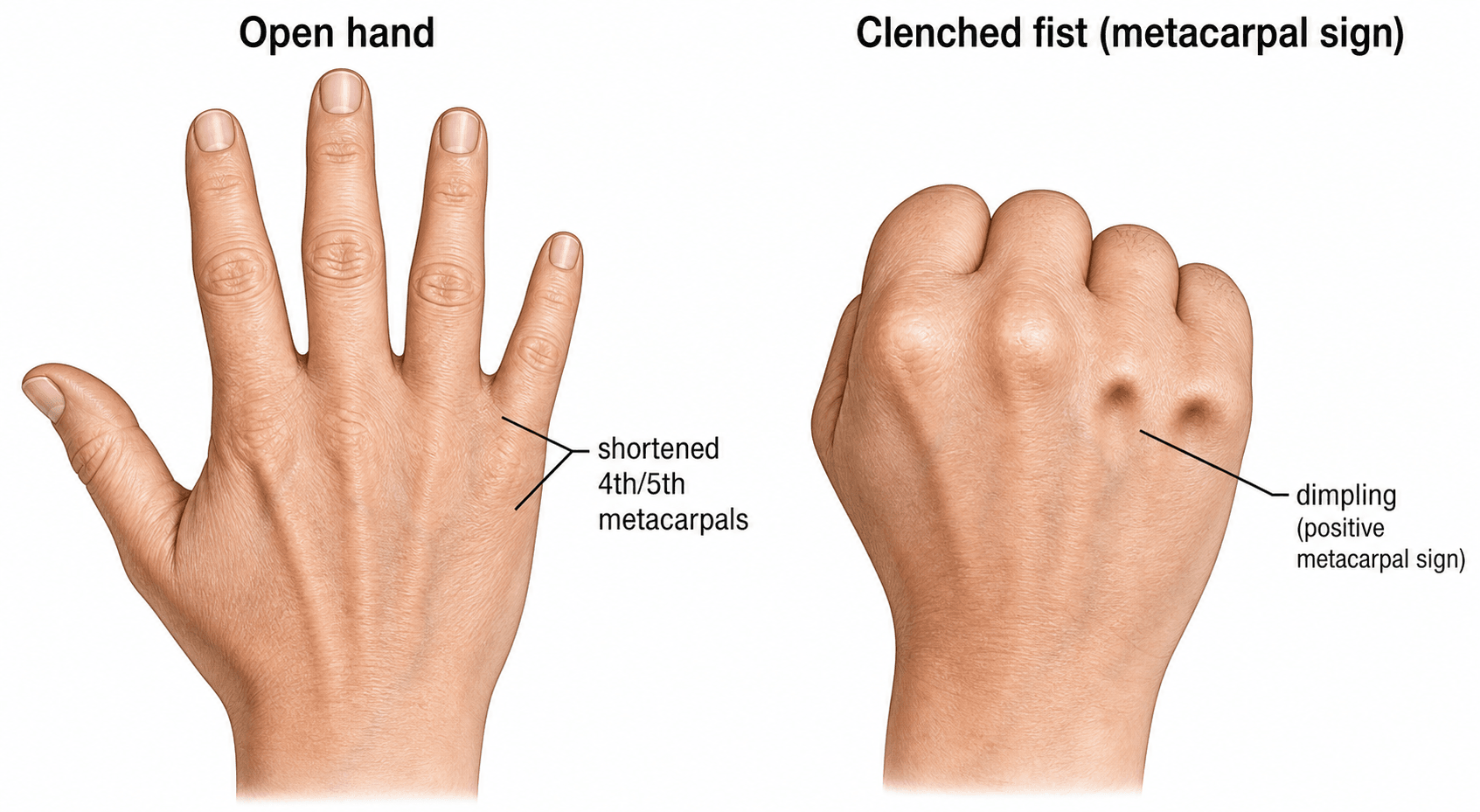
- The AHO phenotype is high-yield: SHORT STATURE, a ROUND ('moon') FACE, OBESITY, BRACHYDACTYLY - characteristically SHORTENED 4th and 5th METACARPALS (and metatarsals) - SUBCUTANEOUS OSSIFICATIONS/calcifications, and variable developmental delay; on clenching a fist the short 4th/5th metacarpals form DIMPLES rather than knuckles (the positive 'metacarpal sign', 'knuckle-knuckle-dimple-dimple').
- DIAGNOSIS combines the biochemistry (low calcium, high phosphate, HIGH PTH, with low/normal vitamin D), the AHO physical features and hand/foot radiographs (short 4th/5th metacarpals/metatarsals, the positive metacarpal sign), and GNAS molecular/methylation testing; associated hormone resistance (e.g. high TSH/hypothyroidism) should be sought.
- MANAGEMENT of the hypocalcaemia is ORAL CALCIUM and ACTIVE VITAMIN D (calcitriol/alfacalcidol) to normalise calcium and lower PTH (PTH resistance means standard vitamin D alone is insufficient), plus treatment of any associated hormone deficiencies (e.g. levothyroxine for hypothyroidism), monitoring for hypercalciuria, and genetic counselling; the skeletal/brachydactyly features themselves rarely need surgery.
- “PHP = PTH RESISTANCE: low calcium + high phosphate + HIGH PTH (vs hypoparathyroidism = low PTH).
- “GNAS/Gs-alpha, IMPRINTED: maternal = PHP1a (AHO + hormone resistance); paternal = PPHP (AHO only, normal biochemistry).
- “AHO: short stature, round face, obesity, SHORT 4th/5th metacarpals (metacarpal sign), subcutaneous ossifications. Treat hypocalcaemia with calcium + active vitamin D.
Low calcium, high phosphate, HIGH PTH (target-organ resistance). GNAS/Gs-alpha defect. AHO features in PHP1a.
Low calcium, high phosphate, LOW PTH (gland failure). No AHO phenotype. (Pseudo-PHP = AHO look with NORMAL biochemistry.)
Mechanism & Imprinting
PTH normally binds its receptor and, via Gs-alpha (encoded by GNAS), activates adenylate cyclase and cAMP to raise calcium and excrete phosphate. In PHP, a Gs-alpha defect means the kidney and bone are resistant to PTH, so calcium falls and phosphate rises, and the parathyroids respond by secreting more PTH - hence the paradoxical high PTH with low calcium. Because GNAS is imprinted (expressed differently from the maternal and paternal alleles in some tissues), the parent of origin of the mutation shapes the phenotype: a MATERNAL defect (PHP type 1a) causes both AHO and hormone resistance, whereas a PATERNAL defect (PPHP) causes the AHO physical phenotype without hormone resistance.
Phenotype, Biochemistry & Diagnosis
- AHO phenotype: short stature, round/moon face, obesity, brachydactyly with short 4th/5th metacarpals/metatarsals (the metacarpal sign), subcutaneous ossifications/calcifications, and variable developmental delay/intellectual impairment; basal-ganglia calcification may be seen.
- Biochemistry (PHP 1a/1b): LOW calcium, HIGH phosphate, HIGH PTH, with low/normal 1,25-vitamin D - the high PTH distinguishing it from hypoparathyroidism (low PTH). PPHP has the AHO look but NORMAL calcium and PTH.
- Imaging: hand/foot radiographs show short 4th/5th metacarpals/metatarsals and the positive metacarpal sign; subcutaneous ossifications and intracranial (basal ganglia) calcification may be present.
- Genetics: GNAS sequencing and methylation analysis (for PHP1b imprinting defects) confirm the diagnosis and clarify the subtype; screen for associated hormone resistance (e.g. TSH/hypothyroidism).
- Clinical signs of hypocalcaemia (Chvostek/Trousseau, tetany, seizures, cataracts) may be the presentation.
Placing PHP in the Hypocalcaemia Differential
PHP is most often contrasted with hypoparathyroidism, but the examinable skill is the biochemical-pattern differential that places it among the causes of hypocalcaemia.
- Calcium / Phosphate / PTH
- Low Ca / HIGH phosphate / HIGH PTH
- The discriminator
- Normal renal function plus AHO features; resistance, not gland failure
- The test to send
- GNAS analysis, with creatinine and vitamin D normal
- Calcium / Phosphate / PTH
- Low Ca / HIGH phosphate / LOW PTH
- The discriminator
- Gland failure (post-surgical, autoimmune, DiGeorge); no AHO phenotype
- The test to send
- The PTH level itself - low rather than high is the whole distinction
- Calcium / Phosphate / PTH
- Low Ca / LOW phosphate / HIGH PTH
- The discriminator
- The LOW phosphate of secondary hyperparathyroidism separates it from PHP
- The test to send
- 25-hydroxyvitamin D
- Calcium / Phosphate / PTH
- Low Ca / HIGH phosphate / HIGH PTH
- The discriminator
- Renal failure drives it - the biochemistry otherwise mimics PHP exactly
- The test to send
- Creatinine and eGFR - check these BEFORE diagnosing PTH resistance
- Calcium / Phosphate / PTH
- Low Ca / variable phosphate / LOW or inappropriately normal PTH
- The discriminator
- Magnesium is needed for PTH secretion AND action
- The test to send
- Serum magnesium - cheap, forgotten, and correcting it fixes the calcium
- Calcium / Phosphate / PTH
- NORMAL Ca / NORMAL phosphate / NORMAL PTH
- The discriminator
- AHO phenotype only (paternal GNAS), no hormone resistance
- The test to send
- Normal biochemistry in someone who looks like AHO; parent-of-origin on GNAS testing
Each of these is developed separately in hypoparathyroidism, vitamin D deficiency, osteomalacia and renal osteodystrophy.
Read the pattern: high PTH + high phosphate + low calcium with normal renal function and normal vitamin D = PHP (resistance). High PTH + LOW phosphate = vitamin D deficiency; high PTH + high phosphate + renal failure = CKD-MBD; low/inappropriately-normal PTH with low Ca + high phosphate = true hypoparathyroidism; and check magnesium in any unexplained hypocalcaemia with a low/normal PTH.
Management
- Correct the hypocalcaemia: oral calcium plus ACTIVE vitamin D (calcitriol or alfacalcidol), because PTH resistance impairs renal 1-alpha-hydroxylation, so ordinary vitamin D is insufficient; titrate to a low-normal calcium and a falling PTH, monitoring for hypercalciuria/nephrocalcinosis.
- Manage associated hormone resistance: levothyroxine for TSH resistance/hypothyroidism, and address gonadotropin resistance/growth as needed.
- Genetic counselling: explain the GNAS imprinting and parent-of-origin risk to offspring.
- Orthopaedic: the brachydactyly and short stature seldom require surgery; manage symptomatic subcutaneous ossifications and address any functional issues; coordinate care with endocrinology.
The pitfall is treating PHP as ordinary hypoparathyroidism or as vitamin-D-deficiency hypocalcaemia. The high PTH with low calcium and high phosphate is the giveaway that this is resistance, not gland failure, and it requires active vitamin D (calcitriol) rather than plain vitamin D. Recognise the AHO phenotype (short stature, round face, short 4th/5th metacarpals) and screen for other hormone resistances (especially hypothyroidism), and remember that a relative with the AHO look but normal biochemistry has pseudo-pseudohypoparathyroidism.
The Ellsworth-Howard Test: PHP Type 1 vs Type 2
- The test. In the Ellsworth-Howard test, exogenous PTH is infused and the urinary cAMP and urinary phosphate (phosphaturic) responses are measured.
- Normal / true hypoparathyroidism. Both the urinary cAMP and the phosphaturic responses rise (the target responds normally).
- PHP type 1 (the GNAS/Gs-alpha group - 1a, 1b and 1c). Both responses are BLUNTED, because the lesion is at or proximal to cAMP generation (the receptor-Gs-alpha-adenylate-cyclase step).
- PHP type 2 (rare; NOT a GNAS-imprinting disorder). The urinary cAMP response is NORMAL but the phosphaturic response is blunted - the defect lies distal to cAMP generation.
- So the AHO/GNAS subtypes (1a/1b/1c) are all "type 1" (blunted cAMP), whereas type 2 is a separate, functionally-defined entity with a preserved cAMP response.
Ellsworth-Howard test = infuse PTH, measure urinary cAMP and phosphate. Type 1 (the GNAS group, blunted both cAMP and phosphaturia) vs type 2 (cAMP normal, phosphaturia blunted - defect distal to cAMP). True hypoparathyroidism: both rise. The 1a/1b/1c subtypes are all type 1.
Mnemonics & Memory Aids
RESIST
Hook:PHP = RESIST: the target resists PTH, so PTH is high.
PHP vs PPHP
Hook:Maternal = PHP (resistant); Paternal = Pseudo-PHP (look only).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A short patient with a round face and short ring and little knuckles has low calcium, high phosphate and a HIGH PTH. What is the diagnosis and the underlying mechanism?”
“How would you confirm and manage pseudohypoparathyroidism?”
Mechanism & biochemistry
- End-organ RESISTANCE to PTH (GNAS/Gs-alpha defect)
- Low calcium + high phosphate + HIGH PTH (vs hypoPTH = low PTH)
- Imprinted GNAS: maternal = PHP1a; paternal = PPHP
Subtypes
- PHP1a: AHO + multi-hormone resistance (PTH, TSH, gonadotropins)
- PHP1b: PTH (+/- TSH) resistance, minimal/no AHO (methylation defect)
- PPHP: AHO phenotype WITHOUT hormone resistance (normal Ca/PTH)
AHO phenotype
- Short stature, round/moon face, obesity, developmental delay
- Brachydactyly - short 4th/5th metacarpals/metatarsals (metacarpal sign)
- Subcutaneous ossifications; basal-ganglia calcification
Diagnosis & management
- Biochemistry + AHO features + hand/foot radiographs + GNAS sequencing/methylation
- Treat hypocalcaemia: oral calcium + ACTIVE vitamin D (calcitriol)
- Treat associated resistance (levothyroxine); monitor hypercalciuria; genetic counselling
Evidence & Key Studies
Three-generation familial transmission of a GNAS variant: evolving PHP/PPHP phenotype
- GNAS variants cause pseudohypoparathyroidism (types 1a/1b/1c) and pseudo-pseudohypoparathyroidism, with complex imprinting and parent-of-origin phenotypic variability.
- Affected family members showed Albright hereditary osteodystrophy features (short stature, brachydactyly, round face, obesity); the neonate with the maternally transmitted variant developed PHP1a features (AHO, high PTH, transient hypothyroidism).
- The mother's phenotype resembled PPHP (normocalcaemia, elevated PTH), illustrating how the same GNAS variant produces resistant (PHP) versus non-resistant (PPHP) phenotypes by parent of origin.
Novel variants and clinical heterogeneity in paediatric calcium metabolism disorders (tiered genetic testing)
- In a paediatric calcium-metabolism cohort, PTH resistance (pseudohypoparathyroidism) was among the diagnoses, with GNAS implicated.
- A stepwise (tiered) genetic-testing strategy gave a high diagnostic yield and expanded the mutational spectrum.
- Precise molecular diagnosis is important for management and genetic counselling in these rare disorders.
The GNAS imprinting basis, the PHP-subtype/PPHP distinction by parent of origin and the AHO features come from the cited Demertzidou family report, and the role of genetic testing (GNAS) in diagnosing PTH resistance from the cited Kang cohort. The PTH-resistance biochemistry (high PTH with hypocalcaemia/hyperphosphataemia), the brachydactyly/metacarpal sign and the calcium/active-vitamin-D treatment are standard, well-established teaching. (See also our Calcium Homeostasis / Metabolic Bone and Hypophosphatasia topics.)