Pubic Symphysis Stress / Overuse
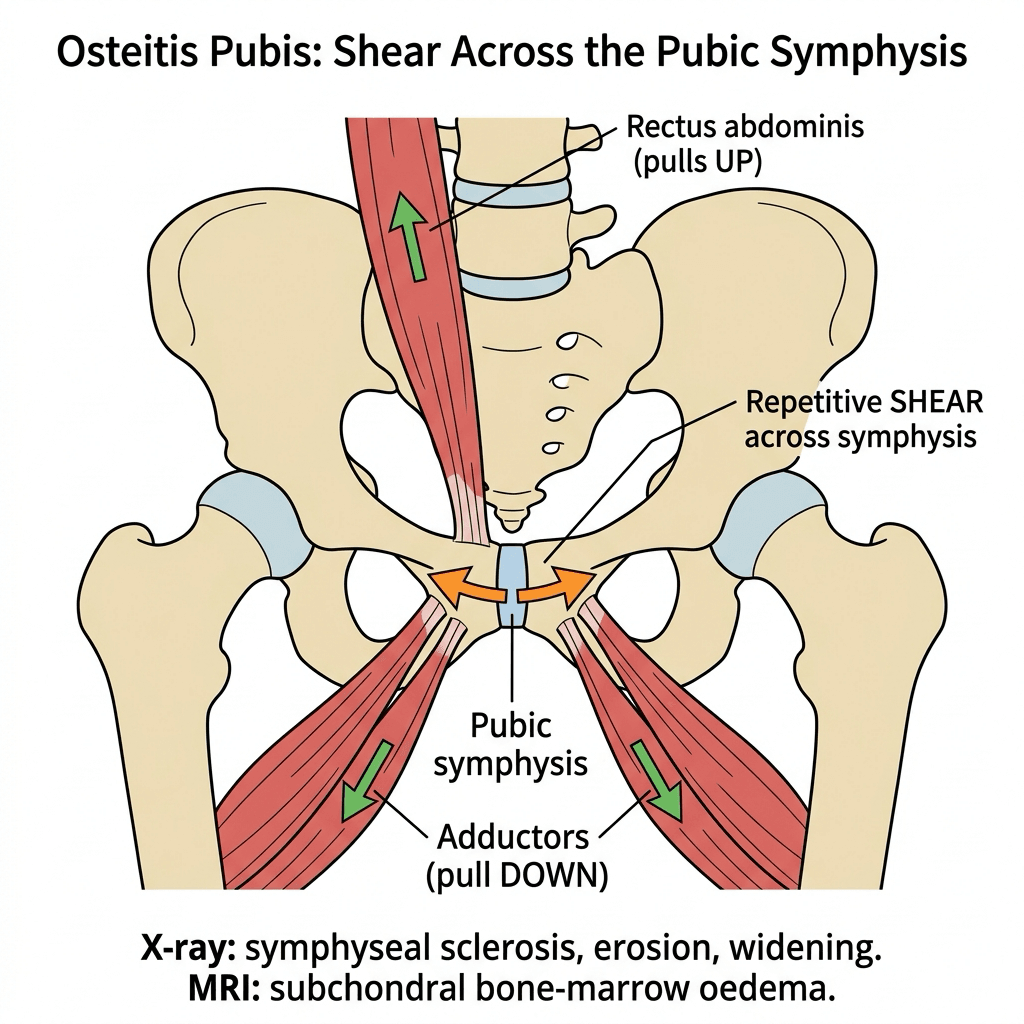
- Osteitis pubis is a chronic OVERUSE inflammatory condition of the PUBIC SYMPHYSIS, produced by repetitive SHEAR and traction across the symphysis from the opposing muscle pulls of the ADDUCTORS arising below and the RECTUS ABDOMINIS inserting above (the two share a common aponeurosis at the pubis); it is seen in athletes who kick, sprint and pivot (soccer/football, Australian football, distance running) and also occurs post-partum and after pelvic or urological surgery.
- It presents with CENTRAL GROIN, suprapubic or symphyseal PAIN, often radiating into the adductors or the lower abdomen, that is worse with kicking, sprinting, pivoting/change of direction, sit-ups and sometimes coughing/sneezing; examination shows TENDERNESS directly over the pubic symphysis and pain on RESISTED ADDUCTION (and sometimes a positive 'squeeze' test).
- It is best understood as part of the ATHLETIC PUBALGIA / chronic GROIN-PAIN spectrum rather than an isolated diagnosis - it overlaps with adductor-related groin pain, rectus-abdominis injury, 'sports hernia' / inguinal disruption (core muscle injury) and even femoroacetabular impingement, where constrained hip motion can transfer stress to the symphysis - so a structured groin-pain assessment is needed and concurrent pathologies sought.
- IMAGING: plain radiographs (including a flamingo/single-leg-stance view for instability) show pubic-symphysis SCLEROSIS, marginal irregularity and EROSION, widening, and sometimes vertical instability; MRI is the most sensitive, showing subchondral BONE-MARROW OEDEMA on either side of the symphysis (the earliest finding) and associated soft-tissue/secondary cleft changes; bone scan or FDG-PET shows increased symphyseal uptake. Sensitivity is not specificity: asymptomatic athletes carry the same MRI findings, so imaging localises a structure rather than proving it is the pain source, and a mixed picture is resolved by an image-guided local-anaesthetic block.
- Because the differential of groin pain includes serious conditions, it is important to EXCLUDE infection (septic arthritis of the symphysis), inflammatory arthropathy and, in the older patient, malignancy - osteitis pubis is an inflammatory/overuse process and should not be assumed if there are systemic features (fever, raised inflammatory markers) suggesting infection.
- MANAGEMENT is predominantly CONSERVATIVE and prolonged: relative rest and activity modification, NSAIDs/analgesia, and a graduated rehabilitation programme that restores ADDUCTOR and CORE (rectus/abdominal) strength and balance and corrects the underlying load, with a slow, criteria-based return to sport; corticosteroid or other symphyseal injections (and addressing any associated adductor/FAI pathology) are used in refractory cases, and surgery (e.g. symphyseal curettage/arthrodesis or treatment of associated pubalgia) is reserved for the few who fail prolonged non-operative care.
- “Osteitis pubis = chronic OVERUSE inflammation of the pubic symphysis from adductor/rectus-abdominis SHEAR (kicking/pivoting athletes); central groin/symphyseal pain, worse on kicking/sit-ups.
- “In the DOHA classification this is PUBIC-RELATED groin pain, alongside adductor-, iliopsoas- and inguinal-related entities (plus hip-related and other causes) - and the entities COEXIST. X-ray: symphyseal sclerosis/erosion/widening; MRI: bone-marrow OEDEMA is sensitive but NOT specific, since asymptomatic athletes show it too. Exclude infection/malignancy.
- “Management CONSERVATIVE and prolonged (rest, NSAIDs, adductor/core rehab, graded return); injections/surgery for refractory cases.
Central groin / symphyseal pain in a kicking/pivoting athlete, worse with kicking/sprinting/sit-ups; tenderness over the symphysis and pain on resisted adduction.
Part of athletic pubalgia (adductor, rectus, sports hernia, FAI). X-ray: symphyseal sclerosis/ erosion; MRI: bone-marrow oedema. Exclude infection/malignancy.
The Pubic Symphysis: Anatomy, the Secondary Cleft Sign and Instability
- The joint. The pubic symphysis is a secondary cartilaginous joint (amphiarthrosis): the two pubic bones are joined by a fibrocartilaginous interpubic disc and reinforced by the superior pubic and arcuate (inferior) pubic ligaments, allowing only small movement. The rectus abdominis and adductor longus share a common aponeurosis at the anterior symphysis - so their opposing pulls load this small joint directly, which is the mechanical basis of the disease.
- The secondary cleft sign. Normally there is a single central (primary) cleft. On MRI or symphysography, a secondary cleft is a fluid/contrast-filled cleft extending inferolaterally from the primary cleft - it represents a microtear/detachment of the common adductor-rectus aponeurosis at its bony attachment, and it typically lies on the symptomatic side.
- Instability on the flamingo view. The flamingo (single-leg-stance) view is taken weight-bearing on each leg in turn; a vertical step-off (translation) of one pubic body relative to the other indicates symphyseal instability - commonly regarded as abnormal beyond around 2 millimetres.
The symphysis is an amphiarthrosis (fibrocartilaginous disc + superior/arcuate ligaments) loaded by the shared rectus-adductor aponeurosis. Two named signs: the secondary cleft (inferolateral cleft on MR/ symphysography = aponeurotic microtear, on the painful side) and the flamingo-view vertical step-off (instability, abnormal beyond about 2 mm).
Mechanism, Spectrum & Imaging
Osteitis pubis is a chronic overuse inflammatory condition of the pubic symphysis, driven by repetitive shear from the opposing pulls of the adductors (below) and rectus abdominis (above), which share a common aponeurosis at the pubis; it is seen in kicking/pivoting/running athletes and also occurs post-partum or after pelvic surgery. It presents with central groin / suprapubic / symphyseal pain worse with kicking, sprinting, pivoting and sit-ups, with tenderness over the symphysis and pain on resisted adduction. It is part of the athletic pubalgia / groin-pain spectrum (overlapping adductor, rectus, sports hernia and FAI), so a structured groin assessment is needed. Radiographs show symphyseal sclerosis, erosion and widening (with a flamingo view for instability); MRI is the most sensitive test, showing subchondral bone-marrow oedema - though not specific, because asymptomatic athletes show it too. Always exclude infection and malignancy.
Differential of the Painful Pubic Symphysis (Don't Miss These)
Symphyseal sclerosis and erosion are the appearance of a bone under stress, and several very different processes stress it. The decisive triggers for stopping and investigating rather than diagnosing overuse are systemic features - fever, night pain, weight loss, raised inflammatory markers. (The broader classification of athletic groin pain sits in Athletic Groin Pain and Athletic Pubalgia.)
- Discriminating features
- Athlete, gradual central groin pain, NORMAL/near-normal markers, symmetrical symphyseal oedema on MRI, no systemic features
- Discriminating features
- FEVER, severe pain, raised CRP/ESR; risk factors = pelvic/urological/gynaecological surgery, IV drug use, athletes; classic organisms Staphylococcus aureus and Pseudomonas aeruginosa; needs aspiration/culture and antibiotics +/- drainage
- Discriminating features
- Inflammatory back/SI symptoms, HLA-B27, symphyseal erosion/sclerosis as part of an enthesitis-driven arthropathy
- Discriminating features
- Distance runners/military (stress) or osteoporotic elderly (insufficiency); focal ramus rather than symphyseal oedema/line on MRI
- Discriminating features
- Symphyseal/ramus resorption or widening mimicking erosion; abnormal calcium/phosphate/PTH/ALP
- Discriminating features
- Older or systemically unwell patient, night pain, destructive lesion - investigate before labelling overuse
The one not to miss is septic arthritis/osteomyelitis of the symphysis - think of it with fever and raised markers, especially after pelvic/urological surgery, in IV drug users and athletes, where Staphylococcus aureus and Pseudomonas aeruginosa are the classic organisms; aspirate and culture before calling sclerosis/erosion "overuse". Also keep spondyloarthropathy, a ramus stress/insufficiency fracture, metabolic bone disease and malignancy on the list.
Management
- Conservative is the mainstay (and prolonged): relative rest and activity modification, NSAIDs/analgesia, and a graduated rehabilitation programme restoring adductor and core (rectus/abdominal) strength and balance and correcting load.
- Treat the whole groin-pain spectrum: identify and address concurrent adductor-related pain, rectus pathology, sports hernia/inguinal disruption and FAI.
- Injections for refractory cases: corticosteroid (or other) symphyseal injection can help selected recalcitrant cases.
- Surgery is last-line: for the few who fail prolonged non-operative care - e.g. symphyseal curettage or arthrodesis, or treatment of the associated pubalgia/adductor pathology.
- Return to sport is slow and criteria-based (pain-free, restored strength) to limit recurrence.
The adductor squeeze test, done properly, is both a diagnostic sign and a monitoring tool. With the patient supine, the examiner's fist or a sphygmomanometer cuff is placed between the knees and the patient squeezes maximally. It is performed at three positions - hips and knees at 0 degrees (legs straight), at 45 degrees of hip flexion, and at 90 degrees - because the position that reproduces pain helps localise the problem, and because using a cuff gives a pressure in millimetres of mercury that can be recorded and compared at each review. That converts "getting better" into a measurement, and it is what a criteria-based return to sport needs: a squeeze pressure that has returned towards the athlete's baseline and is pain-free, rather than an impression. (The adductor-specific interpretation and the Copenhagen protocol are in Adductor and Groin Strain.)
Curettage, wedge resection and arthrodesis of the symphysis are offered for pain, and the complication that follows is mechanical. The symphysis is the anterior strut of the pelvic ring: it resists the forces that would otherwise open the ring anteriorly, and those forces are then carried by the sacroiliac joints. Resecting or widely curetting it can produce anterior instability, and secondary posterior pelvic-ring and sacroiliac pain that is considerably harder to treat than the original symphyseal pain - a patient trading a painful symphysis for an unstable pelvis.
Three practical consequences. Document instability before operating rather than after - flamingo views, looking for vertical translation beyond about 2 mm. If the symphysis is already unstable, resection alone is the wrong operation, and stabilisation or arthrodesis is the relevant discussion. And because the failure mode of the operation is instability, exhaust non-operative treatment properly first - months of structured loading rehabilitation, not weeks - since prolonged conservative care resolves the great majority.
The important safety point in osteitis pubis is that 'inflammatory symphyseal changes' on imaging are not specific: the differential of symphyseal/groin pain with sclerosis and erosion includes SEPTIC arthritis of the pubic symphysis and inflammatory arthropathy, and in the older or systemically unwell patient, malignancy. So before attributing the picture to overuse osteitis pubis, check for systemic features (fever, raised inflammatory markers, night pain, weight loss) and investigate accordingly, because treating an infected or neoplastic symphysis as overuse would be dangerous. Once those are excluded, manage osteitis pubis as the overuse condition it is - with prolonged conservative care addressing the whole groin-pain spectrum - and accept that recovery and return to sport are slow.
Mnemonics & Memory Aids
PUBIS
Hook:PUBIS: Pubic symphysis overuse, Use (kicking athletes), Bone-marrow oedema, Infection/malignancy excluded, Spectrum + Slow conservative recovery.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A footballer has chronic central groin pain worse with kicking. What is osteitis pubis and how would you assess it?”
“How would you manage osteitis pubis?”
What & who
- Chronic overuse inflammation of the pubic symphysis
- Adductor/rectus-abdominis shear across the symphysis
- Kicking/pivoting/running athletes; also post-partum/post-pelvic surgery
Presentation
- Central groin/suprapubic/symphyseal pain, worse with kicking/sprinting/sit-ups
- Tenderness over the symphysis; pain on resisted adduction
- Part of the athletic pubalgia / groin-pain spectrum (adductor, rectus, sports hernia, FAI)
Imaging & differential
- X-ray: symphyseal sclerosis, erosion, widening (flamingo view: vertical translation over ~2 mm = instability)
- MRI: subchondral bone-marrow oedema - SENSITIVE but NOT specific; asymptomatic athletes show it too, so it localises a structure rather than proving the pain source
- Mixed picture: image-guided local-anaesthetic block identifies the dominant pain generator
- Exclude septic arthritis of the symphysis, inflammatory arthropathy, malignancy
Doha terminology
- Formerly 'osteitis pubis' = PUBIC-RELATED groin pain
- Defined entities: adductor-, iliopsoas-, inguinal-, pubic-related; plus hip-related; plus other causes
- Defined by palpation and resisted testing, NOT by MRI - and the entities coexist
Management
- Conservative and prolonged: relative rest, NSAIDs, adductor/core rehab, load correction
- Address concurrent groin-pain spectrum pathology (adductor/FAI/hernia)
- Injections for refractory; surgery (curettage/arthrodesis) last-line; slow criteria-based return
Evidence & Key Studies
Athletic osteitis pubis: inflammatory symphyseal condition with cortical erosions and intense uptake
- Osteitis pubis is an inflammatory condition of the pubic symphysis commonly seen in athletes, here presenting with debilitating groin pain and raised inflammatory markers.
- Imaging (FDG-PET/CT) showed intense uptake at the pubic symphysis with cortical erosions of the pubic bones, while excluding malignancy/lymphoma.
- Anti-inflammatory treatment reduced the pain and normalised inflammatory markers within weeks.
Athletic pubalgia spectrum: pubic symphysis, adductors, rectus abdominis and the link with FAI
- Athletic pubalgia comprises a myriad of conditions involving the pubic symphysis, adductors, rectus abdominis, posterior inguinal wall and related nerves.
- Growing evidence links femoroacetabular impingement (FAI) to pubalgic conditions, where constrained hip motion transfers stress to the pubic symphysis (and SI joint, lumbar spine, hamstrings).
- Management ranges from non-operative care to targeted surgery (mesh hernia repair, adductor tenotomy, rectus repair, or surgery for osteitis pubis), sometimes combined with FAI treatment.
The characterisation of osteitis pubis as an inflammatory symphyseal condition common in athletes, its imaging (cortical erosions and intense symphyseal uptake) with exclusion of malignancy, and its response to anti-inflammatory treatment come from the cited Broos report; the framing of osteitis pubis within the athletic-pubalgia/groin-pain spectrum (adductors, rectus abdominis, inguinal wall) and the link with FAI, and the spectrum of treatments, from the cited Matsuda commentary. The adductor/rectus-shear mechanism, the radiographic sclerosis/erosion/widening, the bone-marrow-oedema MRI finding, and the prolonged conservative rehabilitation pathway are standard, well-established teaching. The Doha classification and the finding that asymptomatic control athletes carry the same MRI appearances as symptomatic ones - with the image-guided diagnostic block as the way through a mixed picture - follow Athletic Groin Pain, so the two carry the same position. (See also Adductor and Groin Strain, Athletic Pubalgia and Femoroacetabular Impingement.)