Ottawa Ankle and Foot Rules
- Missing the Maisonneuve. The rules do NOT screen the proximal fibula — always palpate it separately in any medial-sided ankle injury, or you will miss a syndesmotic Maisonneuve fracture.
- Applying them to a stale injury. The rules are for acute injury (within ~48–72 h) — and not at all with deformity, open wound, or altered sensorium (intoxication/head injury).
- Mis-scoring weight-bearing. It is 4 steps (2 per foot), failed at BOTH time points (right after injury AND in the department); limping a few steps = able = negative.
- Wrong palpation site. Palpate the posterior edge AND tip of each malleolus (the ~6 cm posterior ridge), the navicular, and the base of the 5th metatarsal — not the shaft.
- Reading a negative rule as 'no injury'. It excludes a clinically important fracture (rule-out / SnNout), not a soft-tissue injury — still examine, treat and safety-net.
- 5th-MT base vs Jones. The foot-rule site is the tuberosity base; don't conflate it with the Jones fracture at the metaphyseal-diaphyseal junction.
The Ottawa Ankle and Foot Rules — criteria
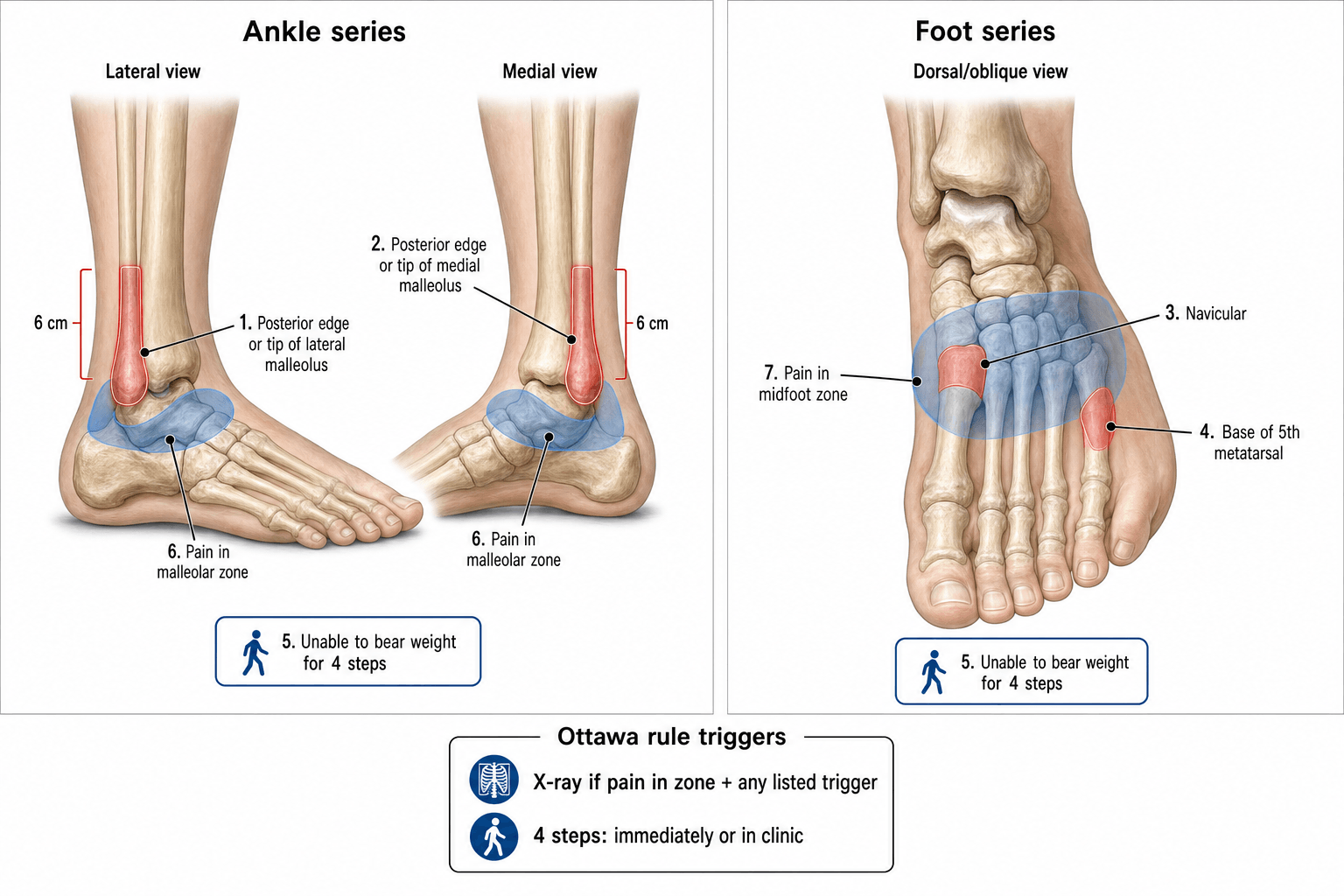
The rules are applied to two separate anatomical zones; a positive finding in either zone mandates radiography of that zone.

- Positive finding
- Present
- Action
- Ankle X-ray (AP, lateral, mortise)
- Positive finding
- Present
- Action
- Ankle X-ray (AP, lateral, mortise)
- Positive finding
- Present
- Action
- Ankle X-ray (AP, lateral, mortise)
- Positive finding
- None of the criteria met
- Action
- No radiograph required
- Positive finding
- Present
- Action
- Foot X-ray (AP, lateral, oblique)
- Positive finding
- Present
- Action
- Foot X-ray (AP, lateral, oblique)
- Positive finding
- Present
- Action
- Foot X-ray (AP, lateral, oblique)
- Positive finding
- None of the criteria met
- Action
- No radiograph required
MAPSAnkle rule palpation
Hook:MAPS — map the malleoli (posterior edge + tip), then check the 4-step weight-bearing.

Nav-5Foot rule palpation
Hook:Nav-5: Navicular and the 5th metatarsal base are the two foot-rule sites (don't confuse the base with the Jones-fracture zone at the metaphyseal-diaphyseal junction).
The patient must be unable to take 4 steps (2 on each foot) at BOTH time points — immediately after the injury AND in the department. Partial weight-bearing through pain still counts as a step; they must be completely unable. A patient who limped off the field but could take steps was weight-bearing at that time point, so this criterion is negative. It applies identically to the ankle and foot rules.
Performance & diagnostic accuracy
The Ottawa rules have been validated in over 30 studies and several meta-analyses. Their key strength is the very high sensitivity — a negative rule effectively excludes a clinically important fracture.
- Ankle rule
- ~98–100% across studies
- Foot rule
- ~98–100%
- Clinical significance
- A negative rule is a highly reliable exclusion test
- Ankle rule
- Modest (roughly 30–50%)
- Foot rule
- Modest
- Clinical significance
- Many positive rules have no fracture — but you won't miss one
- Ankle rule
- ≈ 0.08 (meta-analysis)
- Foot rule
- ≈ 0.08
- Clinical significance
- Drives post-test fracture probability under ~1.4% at 15% prevalence
- Ankle rule
- ~30–40% fewer X-rays
- Foot rule
- ~30–40% fewer X-rays
- Clinical significance
- Major cost and time saving in the ED
The way to explain the Ottawa rules in a viva is as a rule-out test — SnNout: a highly Snsitive test, when Negative, rules out the disease. The trade-off is modest specificity (some patients meeting the criteria have normal X-rays), which is acceptable because the cost of a missed ankle or foot fracture is high.
The Ottawa rules are the textbook example of a clinical decision rule (CDR), and the examiner often turns the topic into a basic-science question: how is a decision rule developed, and why does this one work?
- The three stages of a CDR — (1) Derivation: identify reproducible clinical predictors associated with the outcome (Stiell 1992, recursive partitioning of 32 variables in 750 patients). (2) Validation: prospectively confirm the rule performs in new patients — first narrowly, then broadly across multiple sites and countries (Stiell 1993, then the Bachmann meta-analysis). (3) Impact analysis: prove that using the rule actually changes practice safely (fewer radiographs, no extra missed fractures).
- What makes a good CDR (Stiell/Wells standards) — a clearly defined, clinically important outcome; clinically sensible, reproducible predictors (good inter-observer agreement — the rule's interpretation kappa was ~0.56–0.69); a defined, accepted course of action; and demonstrated accuracy on prospective validation.
- Why high SENSITIVITY, not specificity — for a rule-out instrument where a missed fracture is costly, you deliberately accept many false positives (low specificity → some normal X-rays) to drive false negatives toward zero. With a fracture prevalence of ~15% and a negative likelihood ratio of ~0.08, a negative rule gives a post-test fracture probability under ~1.4%.
- Level of evidence for a CDR — the highest tier (a rule validated in multiple diverse populations with a demonstrated impact on practice); the Ottawa rules sit at this top level, which is why they are recommended as standard practice.
Clinical application — step by step
- 1History & inspectionMechanism, time of injury, ability to walk immediately afterwards, prior problems; inspect for swelling, deformity, open wounds and neurovascular status.
- 2Palpate systematicallyPosterior edge + tip of the lateral malleolus, posterior edge + tip of the medial malleolus, navicular, base of the 5th metatarsal — AND the proximal fibula (Maisonneuve screen).
- 3Test weight-bearingAsk for 4 steps (2 per foot); each must bear weight even if painful. Record whether they could do this immediately after injury AND now.
- 4Apply the ruleAny criterion positive → the appropriate X-ray series (ankle or foot). All negative → no radiograph; diagnose soft-tissue injury, RICE, and safety-net follow-up if symptoms worsen.
Always palpate the proximal fibula in any patient with medial-sided ankle tenderness or a medial malleolar injury. A Maisonneuve fracture is a syndesmotic disruption with a proximal fibular fracture — it will be missed if you only image the ankle. The Ottawa rules do not screen for proximal fibular tenderness, so make this a separate mandatory check.
Guidelines, registries & global practice
- Recommendation
- Recommends the Ottawa Ankle Rules as the clinical decision tool for the need for ankle radiography in adults.
- Recommendation
- Endorses the Ottawa Ankle Rules as a validated, high-sensitivity decision instrument for standard ED practice.
- Recommendation
- Supports validated clinical decision rules (Ottawa) to reduce unnecessary imaging in acute ankle and foot injuries.
- Recommendation
- Includes the Ottawa rules in resource-stewardship initiatives to reduce low-value imaging.
Global practice variation: in many high-income EDs the rules are embedded in triage protocols and electronic decision support. In lower-resource settings, where radiography is limited or costly, they are especially valuable for directing imaging to those who truly need it. Uptake is high in many European and Asian centres; the main cited barrier is medicolegal concern about missing a rare fracture, despite strong evidence. The overall trend is toward broader adoption.
Limitations & special populations
- Developed for acute injuries — apply within ~48–72 h; later, tenderness and weight-bearing findings are less reliable, so keep a low imaging threshold.
- Altered sensorium (intoxication, head injury, dementia) — cannot reliably localise tenderness or report weight-bearing; image liberally.
- Obvious deformity, open wounds or neurovascular compromise — absolute indications for imaging; do not apply the rules.
- Children: a meta-analysis (Dowling 2009) found the rules reliable in children older than 5 years (pooled sensitivity ~98.5%), with lower specificity than adults; applicability in younger/pre-verbal children is less certain — use clinical judgement.
- Pregnancy: apply as normal — the instrument is radiation-free, and avoiding unnecessary X-rays is especially valuable.
- Pre-existing ankle pathology (prior fracture, arthritis, hardware) — baseline tenderness confounds the assessment; interpret with caution and a lower imaging threshold.
Examiners like to ask whether you know any alternatives to the Ottawa rules; a few exist, but none has displaced it:
- Low Risk Ankle Rule (LRAR) — a paediatric refinement: a radiograph is needed only when there is tenderness or swelling outside the "low-risk zone" (the distal fibula and the adjacent lateral ligaments). Most childhood lateral-ankle injuries are low-risk Salter-Harris I or small avulsions that do not change management, so confining imaging to higher-risk sites (distal tibia, medial malleolus, midfoot) stays highly sensitive for clinically significant fractures while cutting imaging further than the Ottawa rules in children.
- Bernese ankle rules — a European alternative based on mechanical stress/compression tests (indirect and direct loading of the malleoli) rather than palpation and weight-bearing; reported to be more specific (fewer unnecessary X-rays) but far less externally validated.
- Bottom line — the Ottawa rules remain the best-validated and default instrument for the acute ankle/midfoot in adults; the LRAR is a useful paediatric option, and the Bernese rules are worth naming as a more-specific alternative. Whichever you cite, the same safety nets apply: acute injury only, palpate the proximal fibula, and a negative rule excludes a fracture, not a soft-tissue injury.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 28-year-old man presents to the emergency department 2 hours after an inversion injury to his right ankle while playing basketball. He was unable to walk off the court. On examination there is swelling over the lateral ankle, tenderness at the posterior edge of the lateral malleolus, and he cannot take 4 steps in the department. How do you apply the Ottawa Ankle Rules?”
“A 45-year-old woman twists her foot on uneven ground. She can walk but with a limp. There is no tenderness at either malleolus, but there is marked tenderness over the navicular on the medial midfoot and at the base of the fifth metatarsal laterally. She can manage 4 steps in the department. How do you apply the Ottawa Foot Rules?”
Exam cheat sheet
- State the two separate rules with exact sites: ankle = posterior edge/tip of either malleolus; foot = navicular or base of the 5th metatarsal.
- Weight-bearing = 4 steps, failed at BOTH time points (immediately after injury AND in the ED) — same criterion for both rules.
- Rule-out test (SnNout): ~100% sensitivity, modest specificity; ~30–40% fewer radiographs.
- Always palpate the proximal fibula — the rules do NOT screen for a Maisonneuve fracture.
- Don't apply if injury over ~48–72 h, deformity, open wound, or altered sensorium.
- Children: reliable over age 5 (Dowling); use judgement in the very young.
Ankle rule (malleolar zone)
- X-ray if: bone tenderness at the posterior edge or tip of the lateral malleolus
- X-ray if: bone tenderness at the posterior edge or tip of the medial malleolus
- X-ray if: unable to weight-bear 4 steps both immediately after injury AND in the ED
- All negative: no radiograph — diagnose a soft-tissue injury
Foot rule (midfoot zone)
- X-ray if: bone tenderness at the navicular
- X-ray if: bone tenderness at the base of the fifth metatarsal
- X-ray if: unable to weight-bear 4 steps (both time points)
- All negative: no radiograph needed
Performance & caveats
- Sensitivity ~98–100% — a negative rule effectively excludes fracture (negative LR ≈ 0.08)
- Reduces radiographs by ~30–40% when correctly applied
- Do NOT apply: delayed presentation (over 48–72 h), altered sensorium, deformity, open fracture
- Always palpate the proximal fibula separately — the rules don't screen for a Maisonneuve fracture
- Validated in adults and in children over age 5 across many countries
Evidence Base
A study to develop clinical decision rules for the use of radiography in acute ankle injuries
- Derived the rules from a prospective cohort (750 adults) presenting to two university EDs with acute ankle injuries.
- Malleolar bone tenderness and inability to weight-bear 4 steps were the key predictors; the malleolar rule was 100% sensitive and 40.1% specific.
- Estimated a 36% reduction in ankle radiographic series; the midfoot rule keyed on navicular / base-of-fifth-metatarsal tenderness.
Decision rules for the use of radiography in acute ankle injuries: refinement and prospective validation
- Refined and prospectively validated the rules in two stages (1032 then 453 patients) at two university EDs.
- Sensitivity 100% for both malleolar and midfoot fractures; the probability of fracture with a negative rule was 0% (95% CI up to 0.8%).
- Estimated radiograph reduction of ~34% for the ankle series and ~30% for the foot series.
Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review
- Systematic review/meta-analysis: 32 studies met inclusion, 27 (15,581 patients) pooled.
- Pooled negative likelihood ratio ≈ 0.08 for both the ankle and midfoot (and 0.07 in children) — at a 15% fracture prevalence, a negative rule leaves under 1.4% probability of fracture.
- Sensitivity approaches 100% with modest specificity (specificities were not pooled); applying the rules could reduce radiographs by 30–40%.
Accuracy of Ottawa Ankle Rules to exclude fractures of the ankle and midfoot in children: a meta-analysis
- Pooled 12 paediatric studies (3,130 children, 671 fractures, 21% prevalence).
- Pooled sensitivity 98.5% — the rules reliably exclude fracture in children older than 5 years.
- Estimated x-ray reduction of ~24.8% (range 5–44%); the few missed fractures were mostly Salter-Harris I or insignificant avulsions.
According to PubMed, the rules were derived by Stiell et al. 1992 (DOI) and refined/validated by Stiell et al. 1993 (DOI; 100% sensitivity, ~34%/30% radiograph reduction). The pooled accuracy (negative LR ≈ 0.08, ~100% sensitivity, 30–40% reduction) comes from Bachmann et al. 2003 (DOI), and the paediatric evidence (children over 5 years, sensitivity 98.5%) from Dowling et al. 2009 (DOI).