Medial Knee Pain | Sartorius-Gracilis-Semitendinosus | Common in Obese and OA
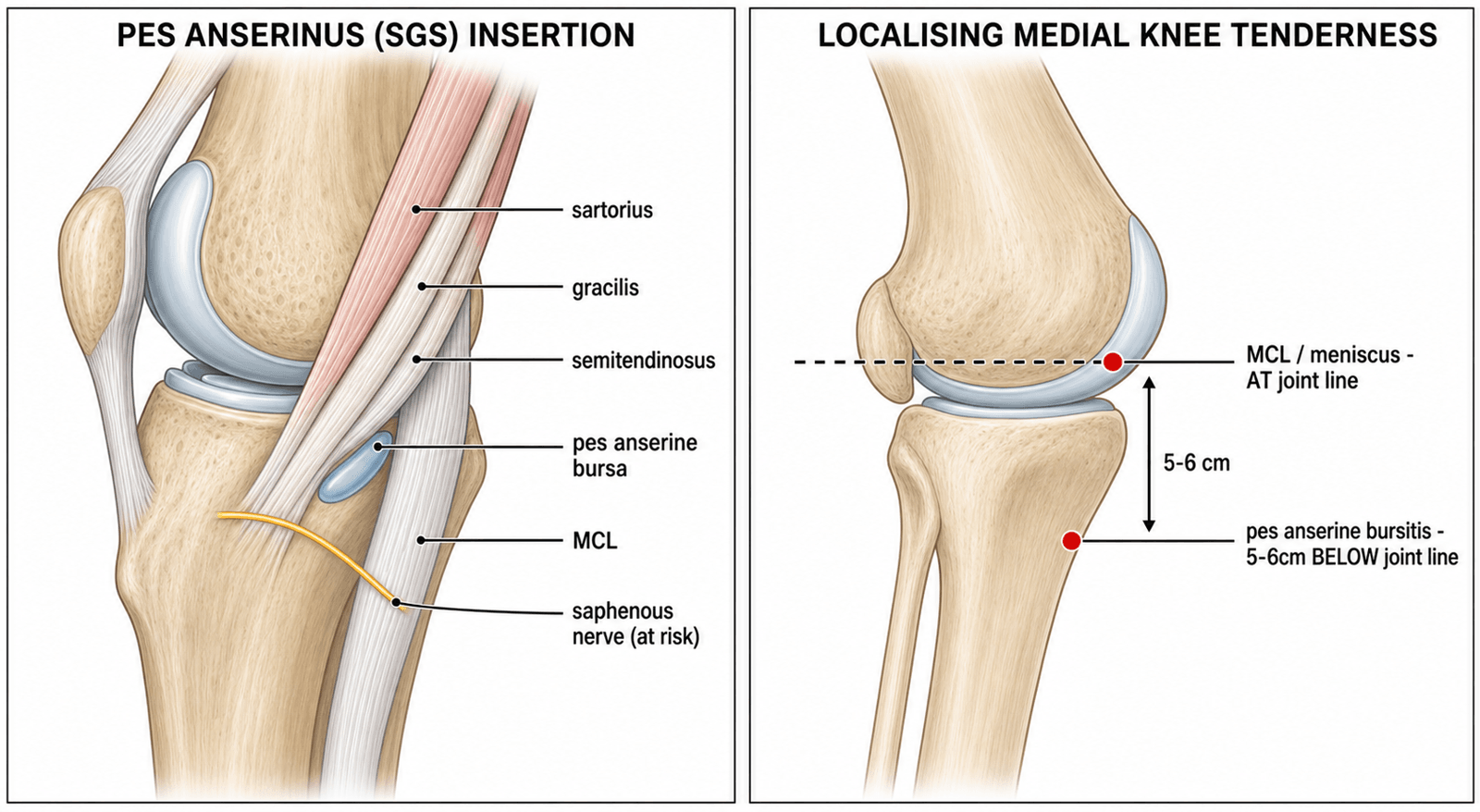
- SGS mnemonic - Sartorius, Gracilis, Semitendinosus form the pes anserinus (goose foot)
- Location 5-6cm below joint line - distinguishes from medial compartment OA or MCL pathology
- Associated with obesity and knee OA - treat underlying conditions for lasting relief
- Injection technique - target 2cm distal and 2cm medial to tibial tuberosity
- Often misdiagnosed as medial meniscal tear or MCL injury - key differentiating feature is tenderness location
- “Pes anserine tendons insert on anteromedial tibia 5-6cm below joint line
- “All three muscles cross both hip and knee joints (except short head biceps)
- “Saphenous nerve runs posterior to pes anserinus - at risk with injection
- “Bursa lies between MCL and conjoined tendon insertion
Sartorius, Gracilis, Semitendinosus - superficial to deep order, insert on anteromedial proximal tibia. All are flexors and internal rotators of the knee. Bursa lies deep to the tendons, superficial to tibial insertion of MCL.
Pain and tenderness 5-6cm below medial joint line - worse with stairs, rising from chair, night pain lying on affected side. May have local swelling but no effusion. Distinguish from MCL (at joint line) and meniscus (joint line, mechanical symptoms).
Obesity, knee OA, valgus malalignment - common triad. Also runners (especially increasing mileage), diabetics, and women. Mechanical factors include tight hamstrings and pes planus.
Conservative first - relative rest, ice, NSAIDs, stretching, correction of biomechanics. Corticosteroid injection if conservative fails. Target 2cm distal and medial to tibial tubercle. Avoid saphenous nerve.
Overview and Epidemiology
Pes anserine bursitis is inflammation of the anserine bursa located on the anteromedial aspect of the proximal tibia. The name "pes anserinus" (Latin for "goose foot") derives from the fan-shaped appearance of the three tendons that insert at this location. The condition is a common but often underdiagnosed cause of medial knee pain, particularly in middle-aged obese women with concurrent knee osteoarthritis.
- Peak incidence in 40-60 year age group
- Marked female predominance (4:1 ratio)
- Strong association with obesity (BMI greater than 30)
- Prevalence of 2.5% in patients with knee osteoarthritis
- Common in runners and athletes with repetitive knee flexion activities
- Knee osteoarthritis (most common)
- Obesity and metabolic syndrome
- Diabetes mellitus (strong, independent association; ~36% of type 2 diabetics affected, Cohen 1997)
- Type II collagen disorders
- Valgus knee malalignment
- Pes planus (flat foot)
Pes anserine bursitis frequently coexists with medial compartment knee osteoarthritis. In patients with knee OA presenting with medial knee pain, always examine the pes anserinus region - the bursitis may be the primary pain generator and is more amenable to treatment than the underlying OA.
Mechanism: The bursa becomes inflamed through repetitive friction between the pes anserine tendons and the underlying tibial bone or MCL:
- Overuse from running (especially increasing distance rapidly)
- Repetitive knee flexion activities (cycling, swimming breaststroke)
- Direct trauma to the medial knee
- Chronic mechanical irritation from valgus malalignment
Pathophysiology and Anatomy
Pes Anserinus Complex
The pes anserinus is formed by the conjoined tendons of three muscles inserting on the anteromedial surface of the proximal tibia, approximately 5-6cm distal to the medial joint line. The name derives from the resemblance to a goose foot when the tendons fan out at their insertion.
Component Muscles (Superficial to Deep - SGS):
- Origin
- ASIS
- Innervation
- Femoral nerve (L2-3)
- Primary Action
- Hip flexion, knee flexion, external rotation
- Origin
- Inferior pubic ramus
- Innervation
- Obturator nerve (L2-3)
- Primary Action
- Hip adduction, knee flexion, internal rotation
- Origin
- Ischial tuberosity
- Innervation
- Sciatic nerve (tibial division L5-S2)
- Primary Action
- Hip extension, knee flexion, internal rotation
All three pes anserine muscles cross both the hip and knee joints, making them prone to strain with activities involving simultaneous hip and knee motion. They act synergistically as knee flexors and tibial internal rotators - this action counters the automatic external rotation that occurs with knee extension (screw-home mechanism).
Pes Anserine Bursa
The anserine bursa is located:
- Deep to the pes anserine tendon insertion
- Superficial to the tibial attachment of the MCL
- Approximately 5-6cm distal to the medial joint line
- On the anteromedial surface of the proximal tibia
The bursa facilitates gliding of the pes anserine tendons over the underlying MCL and tibial periosteum. A separate bursa may exist between each tendon in some individuals.
Adjacent Structures
Saphenous Nerve: The infrapatellar branch of the saphenous nerve runs in close proximity to the pes anserinus, passing anterior to the sartorius tendon before crossing medially. This nerve is at risk during:
- Corticosteroid injection of the bursa
- Medial knee arthroscopy portals
- Harvesting of hamstring grafts for ACL reconstruction
The infrapatellar branch of the saphenous nerve lies in close proximity to the pes anserinus. Injection should be performed with the needle directed away from the posterior aspect of the knee to minimize nerve injury risk. Numbness over the anteromedial tibia following injection suggests nerve irritation.
Medial Collateral Ligament (MCL): The superficial MCL inserts on the tibial metaphysis, deep to the pes anserine insertion. The bursa lies between these two structures. MCL pathology can cause similar medial knee pain but tenderness is located at the joint line.
Pathophysiology of Bursitis
Inflammation develops through:
- Friction: Repetitive movement causes mechanical irritation
- Compression: Valgus alignment increases load on medial structures
- Degeneration: Age-related changes decrease bursal resilience
- Systemic factors: Diabetes impairs tissue healing and predisposes to inflammation
Dynamic Medial Stabilisation by the Pes Anserinus
Beyond being a source of medial pain, the pes anserine group is a functionally important dynamic stabiliser of the medial knee. Because sartorius, gracilis and semitendinosus all cross the knee posteromedially and insert anterior to the tibial axis of rotation, their conjoined pull flexes the knee and internally rotates the tibia, opposing the obligate external rotation of terminal extension (the screw-home mechanism referenced above).
- The pes anserinus acts as a secondary dynamic restraint to valgus load and to anteromedial rotatory instability, supplementing the superficial MCL, which remains the primary static valgus restraint (see the MCL injuries topic).
- Semitendinosus and gracilis, acting as tibial internal rotators, help resist the anterolateral rotatory subluxation that characterises anterior cruciate ligament deficiency; this dynamic contribution is one reason the semitendinosus-gracilis (hamstring) tendons are a mainstay ACL graft.
- Harvesting these tendons removes part of this dynamic medial support, a consideration when a patient with prior hamstring-graft ACL reconstruction later presents with medial knee symptoms.
valgus malalignment and weak frontal-plane control chronically overload the medial soft tissues and the pes anserine complex, which is why hip-abductor and gluteus medius strengthening (frontal-plane control) — not just local treatment of the bursa — is central to durable rehabilitation.
The pes anserinus resists tibial external rotation and valgus. When frontal-plane control is poor (weak gluteus medius, valgus thrust), the medial structures are chronically overloaded. Addressing proximal (hip) control, rather than only the local bursa, is what prevents recurrence — a point examiners look for when you discuss rehabilitation strategy.
Clinical Presentation
History
Pain Characteristics:
- Location: Medial knee, specifically below the joint line
- Character: Aching, burning, or sharp pain
- Onset: Usually gradual, may follow increase in activity
- Aggravating factors: Stairs (especially descending), rising from chair, pivoting
- Night pain: Characteristic - worse lying on affected side
- Morning stiffness: Common, lasting less than 30 minutes
Patients with pes anserine bursitis often report night pain when lying on the affected side due to direct pressure on the inflamed bursa. This distinguishes it from OA pain which typically improves with rest. Asking about sleeping position is a valuable history question.
Associated Symptoms:
- Localized swelling over the medial tibia
- Stiffness of the knee
- Difficulty with activities requiring knee flexion
- Weakness in knee flexion (pain-limited)
Examination
- Localized swelling over anteromedial proximal tibia (may be subtle)
- No knee joint effusion
- Valgus malalignment may be present
- Assess gait for valgus thrust
- Point tenderness 5-6cm below the medial joint line
- Tenderness over the anteromedial tibial surface
- May feel boggy swelling if bursa is distended
- No joint line tenderness (unless concurrent meniscal pathology)
- Technique
- Patient supine, examiner resists knee flexion from 90 degrees
- Positive Finding
- Pain at pes anserine region
- Technique
- Patient seated, knee at 90 degrees, resist tibial internal rotation
- Positive Finding
- Pain at anteromedial tibia
- Technique
- Valgus stress to extended knee
- Positive Finding
- Pain over pes anserinus (not joint line)
- Technique
- Passive knee extension with hip flexed to 90 degrees
- Positive Finding
- Pain at anteromedial tibia
Red Flags to Exclude
The following findings suggest alternative diagnosis and require further investigation:
- Joint line tenderness (meniscal injury, OA)
- Knee joint effusion (intra-articular pathology)
- Instability on valgus stress (MCL injury)
- Mechanical symptoms - locking, giving way (meniscal tear)
- Systemic symptoms - fever, weight loss (infection, malignancy)
Investigations
Pes anserine bursitis is primarily a clinical diagnosis. Investigations are used to exclude other pathology and confirm the diagnosis in unclear cases.
Imaging
- AP, lateral, and skyline views
- Usually normal in isolated pes anserine bursitis
- May show concurrent medial compartment osteoarthritis
- Exclude other bony pathology (stress fracture, tumour)
- Investigation of choice for confirming diagnosis
- Shows anechoic or hypoechoic fluid collection at pes anserine bursa
- Bursa thickness greater than 2mm suggests bursitis
- Can assess MCL and demonstrate tendinopathy
- Useful for guiding injection therapy
- Reserved for diagnostic uncertainty or suspected concurrent pathology
- Shows high T2 signal in bursal region
- Can assess menisci, ligaments, and articular cartilage
- Demonstrates extent of bursal distension
- May reveal concurrent tendinopathy of pes anserine tendons
- Findings
- Usually normal, may show OA
- Clinical Utility
- Exclude bony pathology
- Findings
- Hypoechoic bursal fluid, thickness greater than 2mm
- Clinical Utility
- First-line imaging, guide injection
- Findings
- High T2 signal, bursal distension
- Clinical Utility
- Diagnostic uncertainty, assess for concurrent pathology
Laboratory Tests
Not routinely required. Consider in atypical presentations:
- ESR, CRP - if infection suspected
- Uric acid - if gout suspected
- Rheumatoid factor, anti-CCP - if inflammatory arthritis suspected
- HbA1c - screen for diabetes in recurrent cases
On ultrasound, the diagnosis of pes anserine bursitis is supported by bursal thickness greater than 2mm with hypoechoic fluid collection. The examination should include assessment of the pes anserine tendons for concurrent tendinopathy and the MCL for associated pathology.
Medial Periarticular Fluid Collections that Mimic the Anserine Bursa
Rennie's MRI series (Rennie 2005) emphasised that anserine bursal fluid must be distinguished on axial imaging from other medial periarticular fluid collections, several of which produce medial knee pain or a palpable medial swelling and are routinely mislabelled as anserine bursitis.
- Location
- Deep to conjoined tendons, superficial to distal MCL, anteromedial tibia
- Distinguishing feature
- Fluid below the joint line at the tendon insertion
- Location
- Between semimembranosus tendon and superficial MCL, posteromedially at or above the joint line
- Distinguishing feature
- Sits more posterior and higher than the anserine bursa
- Location
- Between the superficial and deep layers of the MCL
- Distinguishing feature
- Vertically orientated fluid within the ligament complex
- Location
- Adjacent to the medial joint line, communicating with a meniscal tear
- Distinguishing feature
- Traced to a horizontal meniscal tear (see the meniscus tears topic)
- Location
- Variable, may be intratendinous or periarticular
- Distinguishing feature
- Well defined, often septated, no communication with the bursa
The practical rule is anatomical: the anserine bursa lies below the joint line at the conjoined tendon insertion, whereas the semimembranosus-TCL bursa, the MCL bursa and parameniscal cysts sit at or just above the joint line. Axial and coronal sequences localise the collection; a fluid track to a meniscal tear reclassifies the lesion as a parameniscal cyst (managed as meniscal pathology), and joint-line collections should prompt review of the MCL and menisci rather than an anserine label.
Not every medial cystic collection is an anserine bursa. Fluid at or above the joint line favours a semimembranosus-TCL bursa, an MCL bursa, or a parameniscal cyst; anserine bursal fluid sits below the joint line at the tendon insertion. Axial MRI is the sequence that reliably separates them (Rennie 2005).
Differential Diagnosis
Medial knee pain has multiple potential causes. Accurate diagnosis depends on the precise location of tenderness and associated clinical features.
- Location of Tenderness
- 5-6cm below medial joint line
- Key Features
- Night pain, worse on stairs, no effusion
- Location of Tenderness
- Medial joint line
- Key Features
- Mechanical symptoms, effusion, McMurray positive
- Location of Tenderness
- At medial joint line, along MCL
- Key Features
- History of valgus injury, instability on testing
- Location of Tenderness
- Medial joint line
- Key Features
- Crepitus, bony enlargement, X-ray changes
- Location of Tenderness
- Medial patellofemoral joint
- Key Features
- Snapping, anterior knee pain, tender band
- Location of Tenderness
- Along saphenous nerve distribution
- Key Features
- Burning pain, paraesthesia, Tinel positive
The distinguishing feature of pes anserine bursitis is the location of maximum tenderness - 5-6cm BELOW the medial joint line. MCL injuries, meniscal pathology, and medial compartment OA all cause tenderness AT the joint line. Always measure from the joint line when examining for pes anserine bursitis.
Management
Treatment is primarily conservative, with corticosteroid injection reserved for cases not responding to initial measures. Addressing underlying risk factors (obesity, OA, biomechanics) is essential for lasting relief.
Conservative Management
First-Line Measures:
- Relative rest from aggravating activities
- Ice application 15-20 minutes, 3-4 times daily
- NSAIDs (topical or oral) for 2 weeks
- Activity modification - avoid stairs, squatting
- Night splint or pillow between knees for sleeping
- Physiotherapy referral
- Hamstring and quadriceps stretching
- Hip abductor strengthening (gluteus medius)
- Core stability exercises
- Address biomechanical factors
- Graduated return to activity
- Weight loss programme if obese
- Footwear modification or orthotics if required
- Continue stretching and strengthening
- Address underlying OA if present
Physiotherapy Focus:
- Exercises
- Hamstring stretch, ITB stretch, quadriceps stretch
- Rationale
- Reduce tension on pes anserine complex
- Exercises
- Hip abductors, VMO, gluteus medius
- Rationale
- Improve frontal plane control, reduce valgus
- Exercises
- Single leg stance, wobble board
- Rationale
- Improve neuromuscular control
- Exercises
- Gait retraining, squat technique
- Rationale
- Address underlying movement dysfunction
Corticosteroid Injection
Indicated when conservative measures fail after 4-6 weeks. Local corticosteroid injection is the intervention with the strongest historical trial evidence (Alvarez-Nemegyei 2004), but reported response is variable and best in patients with an ultrasound-confirmed bursa (Yoon 2005).
Supine with knee slightly flexed (20-30 degrees) on pillow
- Identify tibial tuberosity
- Move 2cm distally
- Move 2cm medially
- This is the target point overlying the bursa
- Mark injection site
- Clean skin with antiseptic
- Insert 25G needle perpendicular to skin
- Advance until periosteum contacted, then withdraw 2-3mm
- Aspirate to exclude vascular puncture
- Inject 1ml of corticosteroid (e.g., triamcinolone 40mg) with 2ml of local anaesthetic
- Rest for 24-48 hours
- Ice application
- Avoid strenuous activity for 2 weeks
- Review at 4-6 weeks
Following these steps ensures accurate bursa targeting while minimizing complications such as saphenous nerve injury or subcutaneous steroid deposition.
- Saphenous nerve: Direct needle away from posterior aspect of knee
- Infection: Maintain strict aseptic technique
- Skin atrophy: Use deep injection, avoid subcutaneous deposition
- Tendon rupture: Avoid injecting into tendon substance
- Diabetes: Warn about potential blood glucose elevation
- Maximum 3 injections: Risk of soft tissue atrophy with repeated injections
Addressing Underlying Factors
Long-term success requires addressing contributing factors:
- Most important modifiable risk factor
- Every 1kg weight loss reduces knee load by 4kg
- Refer to dietitian and weight management programme
- Treat medial compartment OA if present
- Consider viscosupplementation for concurrent OA
- Unloader bracing if significant valgus
- Orthotics for pes planus
- Footwear advice (supportive shoes)
- Gait retraining for valgus thrust
- Hip strengthening for frontal plane control
Surgical Management
Rarely required. Consider only after failure of comprehensive conservative management including multiple injection attempts.
Options:
- Arthroscopic bursectomy
- Open bursectomy with release of MCL
- Excision of concurrent pathology (medial plica, loose bodies)
Surgical outcomes are variable and should be considered a last resort.
Prognosis and Outcomes
Pes anserine bursitis generally has a good prognosis with appropriate management. However, recurrence is common, particularly if underlying risk factors are not addressed.
- Most patients improve with conservative measures
- Symptoms often improve within 4-6 weeks
- Recovery is variable (reported 10 days to 36 months); full resolution may take several months
- Provides faster relief than rehabilitation alone, with comparable medium-term outcome (Sarifakioglu 2016)
- Duration of relief variable (weeks to months)
- May require repeat injection (maximum 3)
- Best responses in ultrasound-confirmed bursitis; combine with physiotherapy for durable benefit
- Unfavorable
- Chronic symptoms greater than 6 months
- Unfavorable
- Obesity (BMI greater than 30)
- Unfavorable
- Severe medial compartment OA
- Unfavorable
- Poor engagement with rehabilitation
- Unfavorable
- Ongoing contributing factors
The key to preventing recurrence is addressing modifiable risk factors: weight loss, correction of biomechanical abnormalities, and maintenance of flexibility and strength. Patients should be counselled that injection provides symptomatic relief but does not address the underlying cause.
Guidelines, Registries & Global Practice
Pes anserine bursitis (or "anserine syndrome") is a clinical diagnosis managed predominantly in primary care, sports medicine and rheumatology worldwide; there is no dedicated implant or device registry. Orthopaedic referral is reserved for diagnostic uncertainty or refractory disease. The most useful evidence comes from epidemiology and small treatment trials, and from major knee osteoarthritis (OA) guidelines, because the bursitis frequently coexists with — and is overshadowed by — medial compartment OA.
Global epidemiology (verified):
- Finding
- 2.5% (509 MRI studies, 488 patients, UK)
- Source
- Rennie 2005
- Finding
- 36% on clinical exam (94 patients, Israel)
- Source
- Cohen 1997
- Finding
- Strong female predominance (91% of diabetic cases)
- Source
- Cohen 1997
- Finding
- Only 8.7% (26 patients, Korea)
- Source
- Yoon 2005
Side-by-side guideline framing (no society publishes a dedicated pes anserine guideline; relevant guidance comes from knee OA and soft-tissue injection standards):
- Relevant position
- OA CPG supports exercise, weight loss and NSAIDs; intra-articular corticosteroid for OA is limited/inconclusive — extra-articular pes anserine injection is off that scope and used pragmatically
- Relevant position
- OA guidance prioritises exercise and weight management as core treatment; injections are adjuncts, not first-line; supports conservative-first pathways
- Relevant position
- Emphasises addressing biomechanics and OA; image-guided injection where a true bursa is demonstrated
- Relevant position
- Of NSAIDs, physiotherapy and glucocorticoid injection, only injection had trial-proven efficacy at review
Practice variation by resource setting:
- High-resource settings: Ready access to diagnostic ultrasound and image-guided injection; ultrasound increasingly used to confirm a true fluid bursa before injecting and to avoid the saphenous nerve.
- Limited-resource settings: Diagnosis and landmark-guided injection performed on clinical grounds alone; emphasis on low-cost, high-value measures — activity modification, hamstring and hip-abductor rehabilitation, weight loss and generic NSAIDs.
- Universal principle: Outcomes depend more on addressing modifiable drivers (obesity, OA, valgus malalignment, diabetes, training error) than on any single injection, regardless of healthcare system.
Controversies and Areas of Uncertainty
The condition is more contested than its textbook simplicity suggests. High-yield areas of genuine uncertainty:
- Is it actually a bursitis? Imaging frequently fails to demonstrate a fluid-filled bursa. In one ultrasound cohort only 8.7% of clinically diagnosed cases had US-confirmed bursitis (Yoon 2005), and reviews argue for the broader term "anserine syndrome" because the symptomatic structure (bursa, tendon enthesis, or both) is undefined (Helfenstein 2010; Alvarez-Nemegyei 2004).
- Primary pain generator vs incidental finding. Because it coexists with medial compartment OA so often, debate persists over whether the pes anserine region is the true source of pain or a tender accompaniment of OA. This matters: treating the bursitis may give incomplete relief if OA is the driver.
- Injection vs physiotherapy as first-line. A randomised comparison found no significant difference between corticosteroid injection and physiotherapy at 8 weeks (Sarifakioglu 2016), while older evidence-based appraisal credited only injection with trial-proven efficacy (Alvarez-Nemegyei 2004). The pragmatic position is shared decision-making, with injection offering speed and physiotherapy addressing cause.
- Role of ultrasound guidance. Guidance reliably confirms whether a true bursa is present and helps avoid the saphenous nerve, but a clear, consistently quantified accuracy/outcome advantage over landmark injection for this specific target is not well established in high-quality trials — claims of precise accuracy percentages should be treated with caution.
- Biologics (PRP) and the obesity/diabetes link. Platelet-rich plasma and other biologics lack robust topic-specific evidence and remain experimental here. The mechanism behind the strong diabetes association (independent of BMI and glycaemic control) is unexplained.
Show the examiner you know the term "anserine syndrome" and that the lesion is often a soft-tissue enthesopathy rather than a true bursitis. State that you would confirm the diagnosis clinically (point tenderness below the joint line), exclude OA and meniscal pathology, treat conservatively first, and reserve image-guided injection for confirmed or refractory cases.
MCQ Practice Points
Q: What is the order of tendons in the pes anserinus from superficial to deep?
A: Sartorius, Gracilis, Semitendinosus (SGS). Remember "Say Grace before Semitendinosus" - the sartorius is most superficial (from ASIS), gracilis is middle (from pubis), and semitendinosus is deepest (from ischial tuberosity). All three are knee flexors and tibial internal rotators.
Q: What is the key anatomical landmark distinguishing pes anserine bursitis from medial meniscus or MCL pathology?
A: Tenderness 5-6cm BELOW the medial joint line. MCL injuries and meniscal tears cause tenderness AT the joint line. The pes anserine bursa lies on the anteromedial proximal tibia, between the conjoined tendon insertion and the tibial attachment of the MCL.
Q: What nerve is at risk during corticosteroid injection for pes anserine bursitis?
A: The infrapatellar branch of the saphenous nerve. This nerve runs in close proximity to the pes anserinus, anterior to the sartorius tendon. To minimize risk, direct the needle away from the posterior aspect of the knee. Ultrasound guidance improves placement accuracy over the blind landmark technique and confirms whether a true fluid-filled bursa is present.
Q: A 55-year-old obese woman with knee OA presents with medial knee pain worse at night lying on the affected side. What is the most likely diagnosis?
A: Pes anserine bursitis. The classic triad is obesity, knee OA, and female gender (marked female predominance). Night pain when lying on the affected side is characteristic of bursal inflammation from direct pressure. Diabetes is a strong, independent risk factor (around 36% of type 2 diabetics affected in Cohen's series). Pain is also worse on stairs and rising from chairs.
Q: What is the correct injection target for pes anserine bursa injection using landmarks?
A: 2cm distal AND 2cm medial to the tibial tuberosity. Insert a 25G needle perpendicular to skin, advance to periosteum then withdraw 2-3mm. Inject triamcinolone 40mg with 2ml local anaesthetic. Maximum 3 injections due to soft tissue atrophy risk.
At a Glance
Pes anserine bursitis causes medial knee pain at the conjoined tendon insertion of Sartorius, Gracilis, and Semitendinosus (SGS) on the anteromedial proximal tibia. Key diagnostic feature is point tenderness 5-6 cm below the medial joint line—distinguishing it from MCL injury (joint line tenderness) and medial meniscal pathology (mechanical symptoms). Strong associations with obesity, knee osteoarthritis, and valgus malalignment (4:1 female predominance). Pain worsens with stairs, rising from chairs, and lying on the affected side; no joint effusion present. Conservative treatment (relative rest, NSAIDs, hamstring stretching, biomechanical correction) is first-line and effective for most patients, though recovery is variable (reported from 10 days to 36 months). Corticosteroid injection targets 2 cm distal and medial to tibial tubercle—avoid the saphenous nerve which runs posterior to the pes anserinus.
SGSPes Anserinus Components - SGS (Say Grace before Semitendinosus)
Hook:Say Grace before Semitendinosus - superficial to deep order at insertion
OWLPes Anserine Bursitis Risk Factors - OWL
Hook:OWL stays up at night - like pes anserine bursitis night pain!
PITSPes Anserine Examination - PITS
Hook:PITS - the location feels like a pit below the medial joint line
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“In pes anserine bursitis, tenderness is located 5-6cm BELOW the medial joint line on the anteromedial proximal tibia - this is the key distinguishing feature. Other causes of medial knee pain have different sites of maximum tenderness.”
“The examiner is testing anatomical knowledge relevant to injection technique and understanding of the pathology.”
“This tests understanding of the multifactorial nature of the condition and comprehensive management approach.”
“The examiner wants you to demonstrate clinical reasoning and examination skills.”
“The examiner is assessing injection technique safety awareness.”
ANATOMY
- SGS = Sartorius, Gracilis, Semitendinosus (superficial to deep)
- Location: anteromedial proximal tibia, 5-6cm below medial joint line
- Bursa lies between pes anserine tendons and MCL insertion
- Saphenous nerve at risk - runs anterior to sartorius
CLINICAL FEATURES
- Tenderness 5-6cm below medial joint line - KEY distinguishing feature
- Night pain worse lying on affected side
- Pain on stairs, rising from chair, pivoting
- No joint effusion (unlike meniscal/ligament injury)
- Positive resisted knee flexion and internal rotation
RISK FACTORS - OWL
- O = Obesity and Osteoarthritis
- W = Women (4:1) and Wrong biomechanics (valgus, pes planus)
- L = Loading errors (training mistakes, sudden increase in activity)
- Also diabetes (strong independent association, ~36% of type 2 diabetics)
DIFFERENTIAL
- MCL injury - tenderness AT joint line, history of valgus injury
- Medial meniscus tear - joint line tender, mechanical symptoms, effusion
- Medial compartment OA - joint line, crepitus, X-ray changes
- Saphenous neuritis - burning pain, Tinel positive
IMAGING
- X-ray: usually normal, exclude OA and bony pathology
- Ultrasound: investigation of choice, bursa greater than 2mm thickness
- MRI: reserved for diagnostic uncertainty, shows high T2 signal
- Clinical diagnosis primarily - imaging for confirmation or differential
INJECTION TECHNIQUE
- Target: 2cm distal AND 2cm medial to tibial tuberosity
- Triamcinolone 40mg + 2ml local anaesthetic
- Direct needle AWAY from posterior knee (saphenous nerve)
- Maximum 3 injections - risk of soft tissue atrophy
- Ultrasound guidance improves placement and confirms a true bursa
MANAGEMENT PEARLS
- Address underlying factors: obesity, OA, biomechanics
- Physiotherapy: hamstring stretch, hip abductor strengthening
- Most respond to conservative measures (recovery variable)
- Injection for refractory cases - fastest relief, comparable medium-term outcome
- Surgery rarely indicated - last resort only
Evidence Base
- Randomised: physiotherapy vs corticosteroid injection (n=60 with PATB)
- Both effective; no significant difference at 8 weeks
- Bursitis worsens pain and function over OA alone
- Injection a fast, inexpensive option
- 509 MRI studies, 488 patients with knee pain
- Prevalence on MRI 2.5%
- Often mimics medial meniscal tear clinically
- Axial MRI distinguishes bursa from other fluid
- 36% of type 2 diabetics had anserine bursitis
- 91% of affected patients were women
- Independent of age, BMI and glycaemic control
- Strong female predominance confirmed
- Only 8.7% had US-confirmed bursitis despite clinical diagnosis
- Corticosteroid injection improved VAS and WOMAC
- US-positive patients had the best response
- Many clinically diagnosed cases lack a true bursa lesion
- Imaging frequently cannot confirm true bursitis
- Diabetes is the best-established risk factor
- Recovery highly variable (10 days to 36 months)
- Pathoanatomy remains uncertain
- Only glucocorticoid injection had trial-proven efficacy at the time
- NSAID and physiotherapy evidence was weak
- Diagnosis is clinical (inferomedial tenderness)
- Significant knowledge gaps in pathogenesis
Suggested Reading
- Helfenstein M Jr, Kuromoto J. Anserine syndrome. Rev Bras Reumatol. 2010;50(3):313-327. doi:10.1590/S0482-50042010000300011
- Sarifakioglu B, Afsar SI, Yalbuzdag SA, et al. Comparison of the efficacy of physical therapy and corticosteroid injection in the treatment of pes anserine tendino-bursitis. J Phys Ther Sci. 2016;28(7):1993-1997. doi:10.1589/jpts.28.1993
- Yoon HS, Kim SE, Suh YR, et al. Correlation between ultrasonographic findings and the response to corticosteroid injection in pes anserinus tendinobursitis syndrome in knee osteoarthritis patients. J Korean Med Sci. 2005;20(1):109-112. doi:10.3346/jkms.2005.20.1.109
- Draghi F, Ferrozzi G, Urciuoli L, et al. Ultrasound of the knee bursae. J Ultrasound. 2015;18(4):293-303. doi:10.1007/s40477-015-0168-7
- Rennie WJ, Saifuddin A. Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal Radiol. 2005;34(7):395-398. doi:10.1007/s00256-005-0918-7
- Cohen SE, Mahul O, Meir R, Rubinow A. Anserine bursitis and non-insulin dependent diabetes mellitus. J Rheumatol. 1997;24(11):2162-2165.
- Alvarez-Nemegyei J, Canoso JJ. Evidence-based soft tissue rheumatology IV: anserine bursitis. J Clin Rheumatol. 2004;10(4):205-206. doi:10.1097/01.rhu.0000135561.41660.b0
- Nguyen US, Zhang Y, Zhu Y, et al. Increasing prevalence of knee pain and symptomatic knee osteoarthritis. Ann Intern Med. 2011;155(11):725-732. doi:10.7326/0003-4819-155-11-201112060-00004
Key Guidelines
- AAOS Clinical Practice Guideline: Management of Osteoarthritis of the Knee (Non-Arthroplasty), 3rd ed (2021)
- NICE NG226 / BOA guidance on osteoarthritis: assessment and management (UK)
- EFORT / European consensus statements on non-operative knee OA management
Additional Reading
- Uson J, Aguado P, Bernad M, et al. Pes anserinus tendino-bursitis: what are we talking about? Scand J Rheumatol. 2000;29(3):184-186.
- Abeles M. Anserine bursitis: a cause of knee pain in patients with osteoarthritis. Prim Care. 2004;31(4):905-912.