Pipkin Classification of Femoral Head Fractures
The Pipkin classification
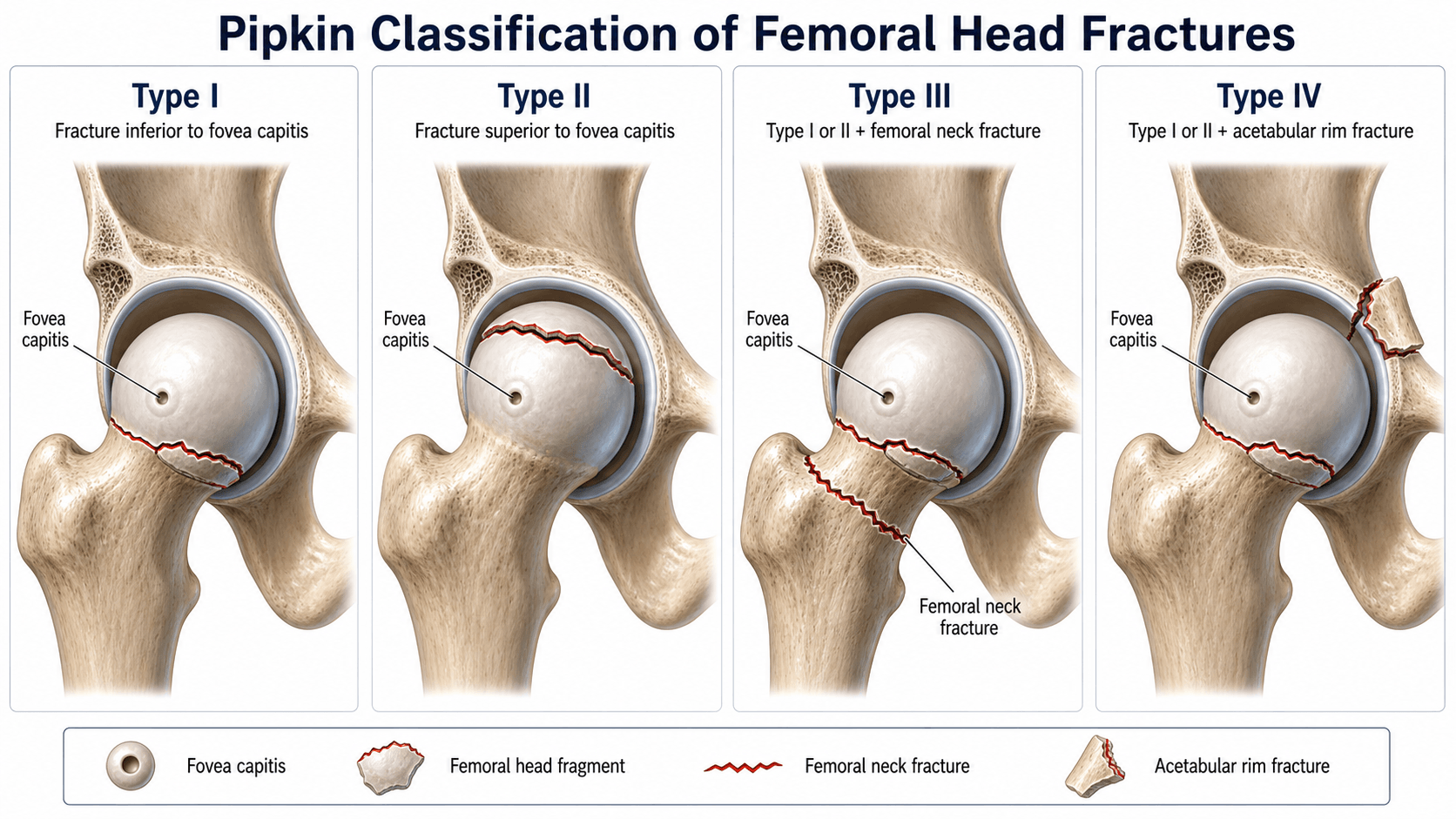
The Pipkin classification applies to femoral head fractures sustained during posterior dislocation of the hip — most commonly a dashboard-type injury. Each type is defined by the fragment's relationship to the fovea capitis and the presence of an associated femoral neck or acetabular fracture.
- Definition
- Infrafoveal fracture (below the fovea capitis)
- Weight-bearing surface
- Not involved
- Key feature
- Small fragment sheared off; attached to the ligamentum teres
- Definition
- Suprafoveal fracture (above the fovea capitis)
- Weight-bearing surface
- Involved
- Key feature
- Fragment includes the weight-bearing dome; congruity depends on reduction
- Definition
- Type I or II PLUS a femoral neck fracture
- Weight-bearing surface
- Variable
- Key feature
- Highest AVN risk — retinacular vessels disrupted at the neck
- Definition
- Type I or II PLUS an acetabular posterior wall fracture
- Weight-bearing surface
- Variable
- Key feature
- Fracture-dislocation complex; the wall must be addressed

BANWThe four Pipkin types
Hook:1-Below, 2-Above, 3-Neck, 4-Wall — climbing from simple to complex.
Below the fovea (type I) the fragment does not articulate with the acetabulum — it is attached to the ligamentum teres and is often small. Above the fovea (type II) the fragment is part of the weight-bearing dome, so even a small step-off affects joint mechanics — hence a lower threshold for operative fixation of a type II fragment. The articulating surface is what is at stake.
Management & surgical decision-making
- 1Reduce the hip urgentlyClosed reduction within ~6 hours (a maximum of ~two gentle attempts) to limit AVN and chondral damage; document neurovascular status (sciatic/peroneal) before and after. An irreducible or non-concentric reduction mandates urgent open surgery.
- 2Classify on CT, not the injury filmPost-reduction CT (fine cuts) assigns the Pipkin type, checks concentricity, finds loose bodies, and excludes an occult femoral neck or acetabular fracture (which would make it type III/IV).
- 3Fix what needs fixingType I: excise/ORIF if incongruent, loose bodies or incarcerated; type II: ORIF for over 2 mm step-off or any incongruity; type III: ORIF both (young, undisplaced neck) or arthroplasty (older/displaced); type IV: fix the posterior wall (± head).
- 4Choose the approach by what you must reachAnterior (Smith-Petersen) for the head fragment (preserves the posterior MFCA supply); posterior (Kocher-Langenbeck) for the wall; Ganz surgical dislocation when both articular surfaces need access.

- Non-operative if…
- Congruent reduction, small fragment, no loose bodies, stable
- Operative indication
- Incongruent reduction, loose bodies, incarcerated fragment
- Preferred approach
- Anterior (Smith-Petersen) for excision or ORIF
- Non-operative if…
- Rarely — most need fixation
- Operative indication
- Step-off over 2 mm or any joint incongruity
- Preferred approach
- Anterior (Smith-Petersen) or Ganz surgical dislocation
- Non-operative if…
- Rarely
- Operative indication
- Young + non-displaced neck → ORIF both; older/displaced → arthroplasty
- Preferred approach
- Anterior for head+neck; Ganz for comprehensive access
- Non-operative if…
- Almost always operative
- Operative indication
- Posterior wall fixation ± femoral head ORIF
- Preferred approach
- Posterior (Kocher-Langenbeck); Ganz if the head also needs work
Closed reduction of the hip is the immediate priority in every Pipkin injury. AVN risk rises sharply if the hip remains dislocated beyond ~6 hours; attempt no more than ~two gentle closed reductions (repeated forceful attempts increase chondral damage and AVN). After reduction, confirm concentric reduction and proceed to CT. An irreducible dislocation, or a non-concentric reduction (often an interposed fragment), mandates urgent open intervention.
The reduction itself is examinable. Perform it under adequate sedation or general anaesthesia with muscle relaxation - a tense patient prevents reduction and forces repeated forceful attempts. The standard Allis maneuver: the patient supine, an assistant stabilises the pelvis, and the surgeon applies in-line longitudinal traction with the hip and knee flexed to about 90° and gentle internal/external rotation to lever the head over the posterior rim. Alternatives are the Bigelow, the Stimson (patient prone with the leg hanging, gravity traction plus downward pressure on the flexed knee) and the Captain Morgan (the surgeon's flexed knee under the patient's knee as a fulcrum). A palpable/audible clunk and a concentric reduction on imaging confirm success; then reassess neurovascular status and stability. Limit to a few gentle attempts - an irreducible hip (often an interposed fragment) goes to urgent open reduction.
HWBSurgical approach selection
Hook:Head = Anterior, Wall = Posterior, Both = Ganz.
The dominant blood supply to the adult femoral head is the deep branch of the medial femoral circumflex artery (MFCA), whose terminal lateral epiphyseal / superior retinacular vessels ascend the posterosuperior femoral neck (deep to the short external rotators) to enter the head. The artery of the ligamentum teres (foveal artery) and the lateral femoral circumflex contribute little to the adult head. This anatomy explains the two rules above: a posterior (Kocher-Langenbeck) approach and a femoral neck fracture (type III) both threaten that posterosuperior retinacular arcade - so an isolated head fragment is approached anteriorly (Smith-Petersen, sparing the MFCA) and type III carries the highest AVN risk. Counter-intuitively, the Ganz trochanteric-flip is also MFCA-safe, because the trochanteric osteotomy protects the deep branch.
Complications & pitfalls
- Avascular necrosis (AVN) is the most significant complication; the largest systematic review found a pooled AVN rate of about 12%, and it is highest in type III (the femoral neck fracture disrupts the retinacular vessel arcade). Older series quote higher type-specific ranges. Time to reduction is regarded as the key modifiable factor (the ~6-hour rule), though one cohort did not find a statistically significant time effect — so reduce promptly but counsel that AVN can occur despite ideal care.
- Post-traumatic osteoarthritis is common long-term (~20% in the systematic review), driven by chondral damage at dislocation, residual step-off, or late AVN collapse — anatomical reduction of the head fragment is the main surgeon-controlled variable.
- Heterotopic ossification is common after operative management (~17%); prophylaxis with indometacin or single-fraction radiotherapy is used.
- Sciatic nerve injury (usually the peroneal division) complicates posterior fracture-dislocations — document neurovascular status before and after reduction; most neuropraxias recover.
- Missed injuries — always exclude an occult femoral neck fracture on CT (a missed neck fracture converts a type I/II into a type III and changes everything), and screen for knee injuries (dashboard mechanism → PCL, patella).
- Loose bodies preventing concentric reduction are an absolute indication for removal regardless of type.
The 4 TsAVN risk factors after hip dislocation
Hook:The 4 Ts of AVN: Time, Type, Trauma, Technique.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 32-year-old man is involved in a head-on road traffic collision. His right lower limb is shortened and internally rotated. Radiographs show a posterior dislocation of the right hip with a femoral head fracture fragment visible in the joint. How do you manage this patient?”
“A 55-year-old woman sustains a posterior fracture-dislocation of the hip. After successful closed reduction, CT confirms a Pipkin type III injury: a suprafoveal femoral head fragment and a minimally displaced femoral neck fracture. How would you manage this?”
Exam & revision
Everything below condenses the Pipkin classification for revision and viva practice.
- Reduce the hip first (~6 h), then classify on CT — never assign a Pipkin type from the injury film.
- The fovea is the dividing line: I infrafoveal (non-weight-bearing), II suprafoveal (weight-bearing dome → low threshold to fix).
- Type III (+ femoral neck) = highest AVN risk; type IV (+ posterior wall) is a fracture-dislocation complex.
- Approach by target: anterior for the head (protects the MFCA), posterior for the wall, Ganz for both.
- Always exclude an occult femoral neck fracture on CT (a missed type III changes management).
- AVN ~12% overall, highest in type III; PTA ~20%; HO ~17%.
One-Below, Two-Above, Three-Neck, Four-WallThe four types
Hook:1-Below, 2-Above, 3-Neck, 4-Wall.
Exam cheat sheet
The four types (fovea is the key landmark)
- Type I: infrafoveal, below fovea, non-weight-bearing - non-operative if congruent and no loose bodies
- Type II: suprafoveal, above fovea, weight-bearing dome - ORIF if step-off over 2 mm or incongruity
- Type III: any head fracture PLUS femoral neck fracture - highest AVN risk
- Type IV: any head fracture PLUS acetabular posterior wall fracture - almost always operative
Management sequence
- Step 1: urgent closed reduction (~6 h) - max ~two gentle attempts; document neurovascular status
- Step 2: post-reduction CT for classification and planning
- Step 3: non-concentric reduction or loose bodies = operative, regardless of type
- Step 4: approach - anterior for head, posterior for wall, Ganz for both
Complications
- AVN ~12% overall (systematic review), highest in type III; time to reduction the key modifiable factor
- Post-traumatic arthritis ~20%; heterotopic ossification ~17% (prophylax with indometacin/radiotherapy)
- Always exclude an occult femoral neck fracture on CT (missed type III)
- Sciatic nerve (peroneal division) at risk - document pre/post reduction
Evidence Base
Treatment of grade IV fracture-dislocation of the hip
- Original description of the four-type classification of femoral head fractures associated with posterior hip dislocation.
- Defined the fovea capitis as the landmark separating type I (infrafoveal) from type II (suprafoveal), with type III adding a neck fracture and type IV an acetabular fracture.
- Emphasised prompt reduction of the dislocation and open treatment of displaced fragments.
Fractures of the femoral head
- Literature review of 238 published cases plus 27 of the authors' own, addressing the ambiguities of earlier classification schemes.
- Proposed an improved (Brumback) classification with treatment guidelines for each femoral head fracture type.
- Emphasised prompt concentric reduction followed by individualised treatment of each fracture type.
Intermediate-term experience of Pipkin fracture-dislocations of the hip
- 33 patients (mean 49-month follow-up): 67% good, 18% fair, 15% poor (no excellent results).
- The Pipkin scheme predicted outcome - types 1/2 did significantly better than types 3/4 (p under 0.02).
- Time to reduction, timing of definitive surgery and operative approach did NOT significantly affect outcome; prognosis improved when treatment achieved anatomic reduction, joint stability and removal of all interposed fragments.
Management, complications and clinical results of femoral head fractures
- Systematic review of 453 femoral head fractures (450 patients; 84.3% road-traffic injuries); Pipkin was the most widely used classification (65.4%).
- Major late complications: avascular necrosis 11.9%, post-traumatic arthritis 20%, heterotopic ossification 16.8%.
- For Pipkin 1, fragment excision tended to give better results than ORIF (p=0.07); for Pipkin 2, anatomic reduction and stable fixation are advised; the trochanteric-flip and anterior approaches did not endanger the head blood supply more than the posterior approach.
According to PubMed: the classification comes from Pipkin 1957 (PMID 13475403); its refinement and individualised treatment from Brumback et al. 1987 (PMID 3546215); the outcome data (Pipkin predicts outcome; reduction timing/approach not statistically decisive in that cohort) from Marchetti et al. 1996 (DOI); and the pooled complication rates (AVN 11.9%, PTA 20%, HO 16.8%) and approach-safety data from Giannoudis et al. 2009 (DOI). These are an original case series, a review and retrospective/systematic reviews (Level III-IV) - the best available for this rare injury. The ~6-hour reduction rule is standard trauma teaching across the broader literature.