Young Athlete Calf Claudication | Anomalous Gastrocnemius | Love-Whelan Types | Surgical Release
- Think PAES in any young athlete with calf claudication and normal resting pulses
- Functional entrapment (Type F) = normal anatomy, hypertrophied gastrocnemius compresses artery during plantarflexion
- Provocative manoeuvres (active plantarflexion, passive dorsiflexion) abolish or diminish pedal pulses
- CT or MR angiography with provocative positioning is the diagnostic gold standard
- Surgical myotomy of the offending muscle head with arterial reconstruction if the vessel is diseased
- “PAES vs CECS: PAES = vascular symptoms (claudication, pallor); CECS = myofascial pain and parasthesiae with normal pulses
- “Bilateral imaging mandatory even if unilateral symptoms
- “Popliteus muscle or fibrous bands can also entrap (Love-Whelan Type IV)
- “Chronic entrapment may cause popliteal artery thrombosis or aneurysm formation
Young athlete (under 40) with calf claudication. Normal resting pulses. No atherosclerotic risk factors. Symptoms on exertion, relieved by rest. Male predominance but increasingly recognised in female athletes.
Pedal pulses diminish or disappear with active plantarflexion against resistance or forced passive dorsiflexion. This is the bedside hallmark. Always check bilateral pulses in both resting and provoked positions.
PAES vs chronic exertional compartment syndrome (CECS): PAES produces true claudication (pallor, cold foot, pulse loss). CECS produces burning myofascial pain, parasthesiae, and foot drop with normal pulses. Measure compartment pressures if uncertain.
Surgical decompression is definitive for functional and anatomical PAES. Myotomy of the medial gastrocnemius head. Diseased artery segment requires interposition vein graft or bypass. Bilateral surgery if bilateral imaging abnormalities.
- Diagnosis
- Provocative pulse loss, MR angio with plantarflexion
- Treatment
- Myotomy of gastrocnemius head
- Key Pearl
- Bilateral imaging mandatory
- Diagnosis
- Normal anatomy on MR but compression on dynamic imaging
- Treatment
- Myotomy alone usually sufficient
- Key Pearl
- Most common form in athletes
- Diagnosis
- CT angio shows occluded popliteal, collaterals
- Treatment
- Thrombectomy + bypass + myotomy
- Key Pearl
- Late presentation, may need emergency revascularisation
P-U-L-S-EPAES vs CECS Differential
Hook:Check the PULSE to separate vascular entrapment from compartment syndrome!
Overview and Epidemiology
Popliteal artery entrapment syndrome (PAES) is the most common cause of non-atherosclerotic claudication in young athletes. It is frequently misdiagnosed as shin splints, CECS, or lumbar radiculopathy, delaying definitive treatment by months to years. A high index of suspicion and simple bedside provocative pulse testing can clinch the diagnosis. Left untreated, chronic PAES may progress to popliteal artery thrombosis, aneurysm formation, or even acute limb ischaemia requiring emergency revascularisation.
- Age: 15 to 40 years (peak 20 to 30)
- Sex: Male-to-female ratio approximately 2:1
- Athletes: Over-represented due to muscle hypertrophy
- Bilateral: 60 to 70 percent on imaging (may be asymptomatic contralaterally)
- Incidence: Anatomical variants present in approximately 3 to 5 percent of cadaveric specimens
- Delayed diagnosis: Average 12 to 24 months from symptom onset
- Misdiagnosis rate: Over 50 percent initially misdiagnosed
- Progression risk: Chronic entrapment may cause arterial wall damage, thrombosis, or aneurysm
- Functional limitation: Calf pain on running, walking, or dorsiflexion limits sport
- Acute limb ischaemia: Rare but reported in late presentations with thrombosis
Pathophysiology
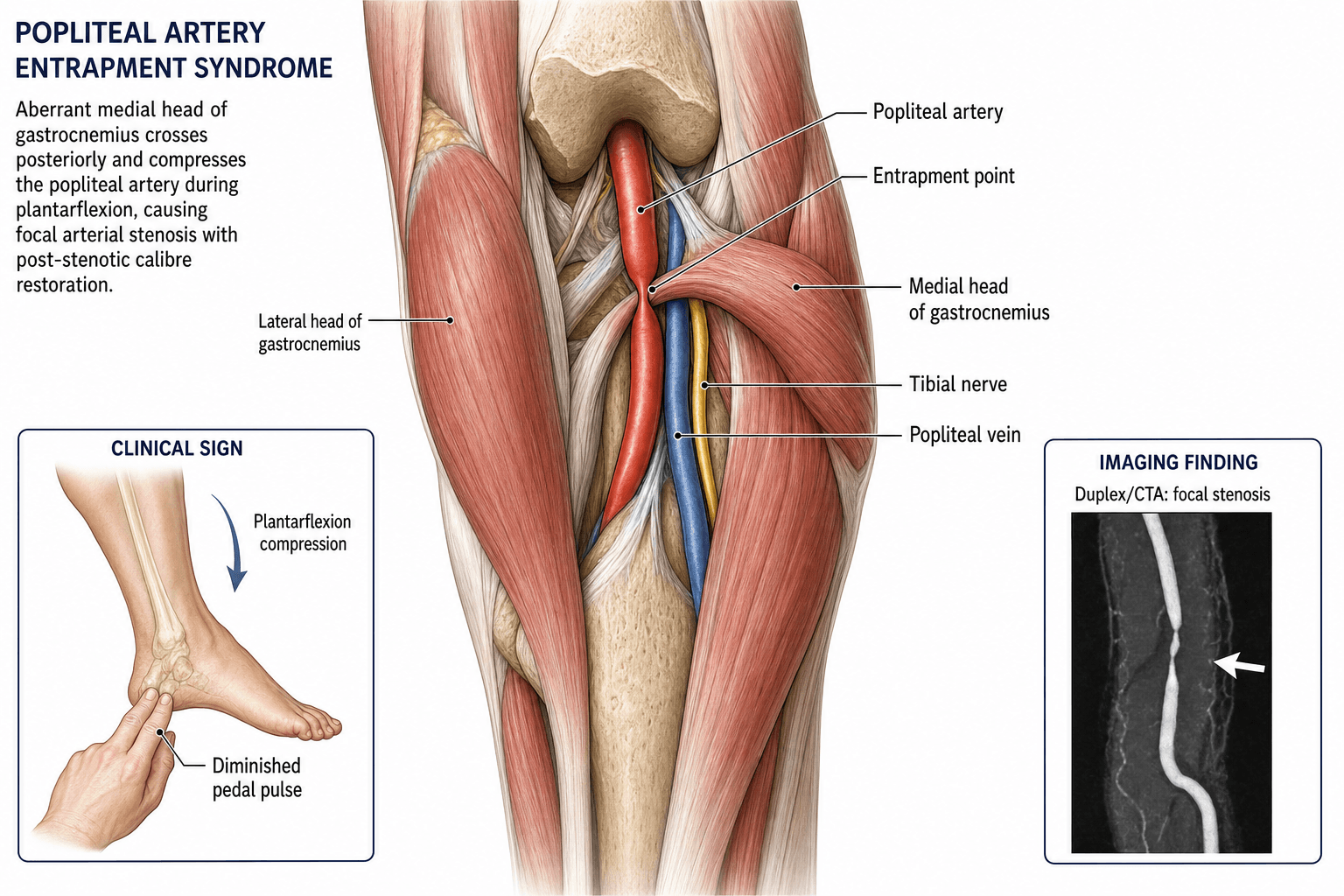
The popliteal artery normally passes between the medial and lateral heads of gastrocnemius through the popliteal fossa without any musculotendinous compression. In PAES, an anomalous relationship between the popliteal artery and the gastrocnemius muscle (most commonly the medial head), popliteus muscle, or fibrous bands leads to repeated arterial compression during plantarflexion and dorsiflexion. This chronic compression causes intimal damage, fibrous narrowing, post-stenotic dilatation, and eventual thrombosis or aneurysm formation. Functional PAES occurs when a normal but hypertrophied gastrocnemius compresses a normally positioned artery during vigorous exercise.
- Normal Position
- Between medial and lateral gastrocnemius heads
- Entrapment Variant
- Medial to medial head or deep to popliteus
- Clinical Consequence
- Compression with ankle movement
- Normal Position
- Originates from medial femoral condyle posteriorly
- Entrapment Variant
- Aberrant origin lateral or deep to artery
- Clinical Consequence
- Direct arterial compression
- Normal Position
- Deep to neurovascular bundle in popliteal fossa
- Entrapment Variant
- Hypertrophied or anomalous fibres crossing artery
- Clinical Consequence
- Type IV entrapment
- Normal Position
- Variable, thin tendon
- Entrapment Variant
- Anomalous slip crossing neurovascular bundle
- Clinical Consequence
- Rare entrapment variant
Stage 1: External compression during exercise (functional)
Stage 2: Intimal irritation and fibrosis from repeated compression
Stage 3: Fibrous narrowing and post-stenotic dilatation
Stage 4: Thrombosis, aneurysm, or complete occlusion
End result: Acute or chronic limb ischaemia
Muscle hypertrophy: Progressive gastrocnemius enlargement narrows the popliteal space
Repetitive ankle movement: Running, cycling, and rowing produce thousands of compression cycles
Functional PAES: Normal anatomy with hypertrophied muscle is the most common form in athletes
Training intensity: Higher training loads correlate with worse compression
Classification and Types
Love-Whelan Anatomical Classification (Types I-VI)
- Anatomical Relationship
- Medial gastrocnemius normal, artery runs medial to it
- Mechanism
- Artery deviates medially around normal muscle course
- Frequency
- Approximately 10 to 15 percent
- Anatomical Relationship
- Aberrant medial gastrocnemius head, artery in normal position
- Mechanism
- Abnormal muscle head crosses and compresses the artery
- Frequency
- Approximately 15 to 20 percent
- Anatomical Relationship
- Anomalous accessory slip of gastrocnemius
- Mechanism
- Muscle slip wraps around artery, compressing it
- Frequency
- Approximately 10 to 15 percent
- Anatomical Relationship
- Popliteus muscle or fibrous band compresses deep artery
- Mechanism
- Artery entrapped deep to popliteus or by congenital fibrous band
- Frequency
- Approximately 5 to 10 percent
- Anatomical Relationship
- Any of Types I-IV with venous entrapment as well
- Mechanism
- Both popliteal artery and vein compressed by anomalous structures
- Frequency
- Approximately 5 percent
- Anatomical Relationship
- Normal anatomy, hypertrophied muscle
- Mechanism
- Muscle hypertrophy compresses artery during exercise only
- Frequency
- Most common form in athletes
The Love-Whelan classification guides surgical planning: anatomical types require resection of the anomalous structure, while functional entrapment responds to myotomy of the gastrocnemius medial head.
M-A-S-S-FLove-Whelan Classification
Hook:MASSF = the types of PAES from medial deviation to functional entrapment!
Clinical Assessment
- Calf claudication: Reproducible pain in the calf or foot on exertion, relieved promptly by rest
- Age: Under 40, typically an athlete or military recruit
- No risk factors: No diabetes, smoking, or hyperlipidaemia
- Cold foot: Numbness, pallor, or coldness in the foot during exercise
- Bilateral symptoms: Up to 30 percent report bilateral symptoms
- Resting examination: Often completely normal with palpable pedal pulses
- Provocative tests: Active plantarflexion against resistance or forced passive dorsiflexion
- Pulse assessment: Palpate DP and PT pulses before, during, and after provocative manoeuvres
- Skin inspection: Look for pallor, delayed capillary refill, or dependent rubor post-exertion
- Bilateral assessment: Always examine both legs even if unilateral symptoms
Technique: With the patient supine, palpate the dorsalis pedis and posterior tibial pulses. Ask the patient to actively plantarflex the foot against resistance (examiner pushes against the forefoot). Alternatively, passively dorsiflex the ankle to maximum.
Positive test: Pedal pulses diminish or disappear during the provocative manoeuvre and return when the ankle returns to neutral.
Key point: A positive provocative test in a young athlete with exertional calf pain is highly suggestive of PAES and mandates imaging. A negative test does not exclude the diagnosis (sensitivity is imperfect, especially for functional PAES where compression occurs only at higher forces).
- Technique
- Patient pushes foot down against examiner resistance
- Positive Finding
- Pulse diminution or loss
- Notes
- Most sensitive bedside test
- Technique
- Examiner forces ankle into maximal dorsiflexion
- Positive Finding
- Pulse diminution or loss
- Notes
- Stretches gastrocnemius, compresses artery
- Technique
- Patient actively dorsiflexes against resistance
- Positive Finding
- Less reliable than plantarflexion
- Notes
- May help identify popliteus-related entrapment
- Pulses
- Diminish with provocation
- Key Discriminator
- Exertional pallor + pulse loss, no atherosclerosis
- Definitive Test
- Dynamic MR/CT angio with provocative positioning
- Pulses
- Normal
- Key Discriminator
- Burning tight pain, raised compartment pressure post-exertion
- Definitive Test
- Compartment pressure measurement pre/post-exercise
- Pulses
- May be diminished
- Key Discriminator
- Cyst in arterial wall, not muscle entrapment
- Definitive Test
- MRI showing cystic lesion in popliteal artery wall
- Pulses
- Absent or reduced
- Key Discriminator
- Atherosclerotic risk factors present, older patient
- Definitive Test
- CT angio showing atheromatous disease
- Pulses
- Normal
- Key Discriminator
- Radiating pain, neurological signs, back pain
- Definitive Test
- MRI lumbar spine
- Pulses
- Normal
- Key Discriminator
- Diffuse posteromedial tibial tenderness, no vascular symptoms
- Definitive Test
- Clinical diagnosis; bone scan if stress fracture suspected
PAES is a vascular problem: calf claudication with pallor, cold foot, and diminished pulses on provocation. The pain is ischaemic. CECS is a myofascial problem: burning, tight, bursting pain with normal pulses. Parasthesiae and foot drop may occur from nerve compression within the compartment. The pain is from elevated compartment pressure. The two conditions can coexist and must be investigated independently. Measure compartment pressures and perform dynamic vascular imaging if either diagnosis is suspected.
Investigations
Imaging and Investigation Protocol
Resting scan: Assess popliteal artery calibre, flow velocities, and any aneurysmal change
Dynamic scan: Repeat with active plantarflexion and passive dorsiflexion
Positive finding: Greater than 50 percent velocity increase or complete flow cessation with provocative manoeuvres
Advantage: Non-invasive, bedside, dynamic, no radiation
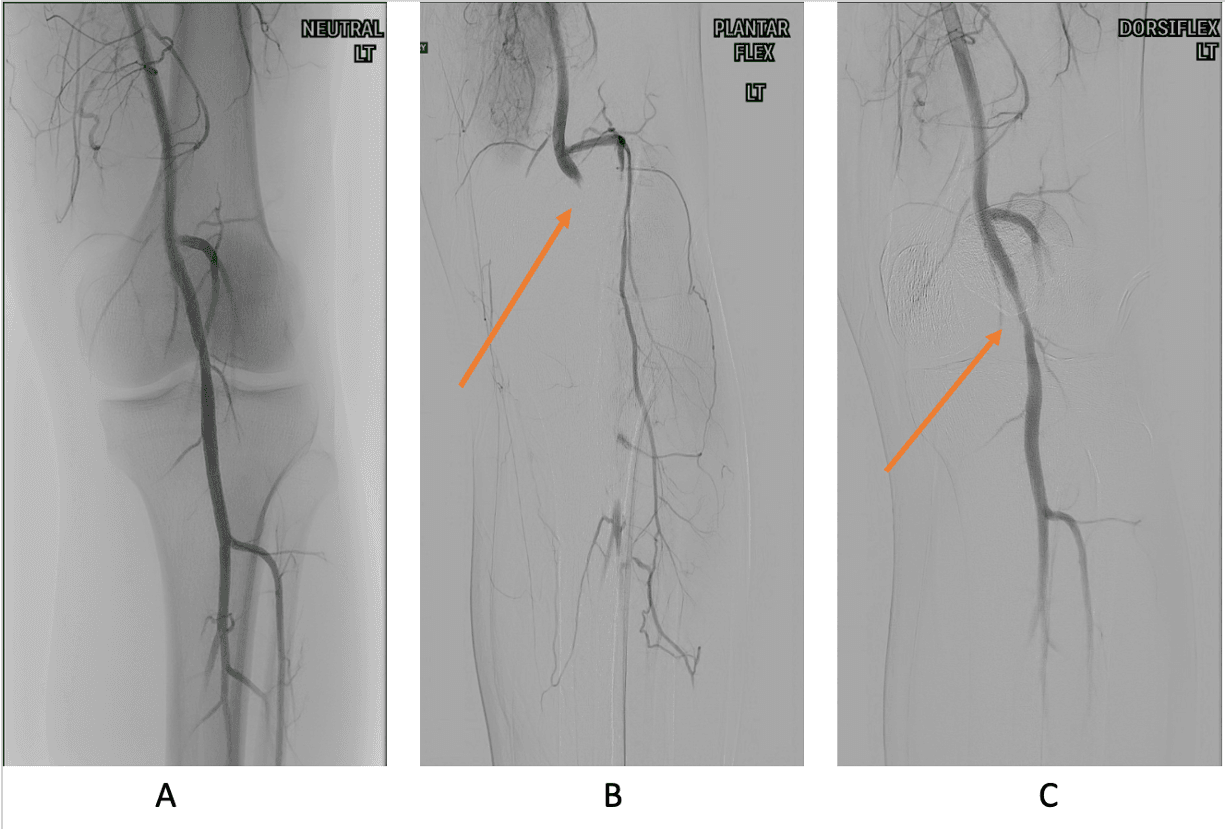
Protocol: MR angiography of the popliteal fossa in neutral position, then with the foot in active plantarflexion or passive dorsiflexion
Findings: Compression or occlusion of the popliteal artery, anomalous musculotendinous structures, arterial wall changes (thickening, aneurysm)
Advantages: No radiation, excellent soft tissue characterisation, shows muscle anatomy and arterial lumen simultaneously
Always image both legs: Bilateral abnormalities found in 60 to 70 percent
Indication: If MRI contraindicated (pacemaker, claustrophobia) or if rapid assessment needed for acute presentation
Protocol: CTA in neutral and plantarflexion positions
Advantages: Faster than MRI, excellent arterial detail, can assess for calcification
Limitation: Ionising radiation, less soft tissue detail than MRI
Indication: If imaging suggests complete popliteal artery occlusion or if endovascular intervention is being considered
Findings: Segmental occlusion, collateral formation, "spindle-shaped" post-stenotic dilatation
Therapeutic role: Catheter-directed thrombolysis for acute thrombosis
The critical step is dynamic imaging with provocative positioning. A resting MRI or CTA alone may be completely normal in functional PAES. The artery must be imaged during plantarflexion or dorsiflexion to demonstrate the compression. Always specify this in the imaging request or the study will be non-diagnostic.
Management Algorithm
Functional PAES (Type VI): Treatment Algorithm
Goal: Eliminate arterial compression by releasing the gastrocnemius medial head
Treatment Protocol
Imaging: Bilateral MR angiography with provocative positioning confirmed
Assess: Artery wall integrity (normal in functional PAES, no graft needed)
Counsel: Bilateral surgery if bilateral compression demonstrated; return to sport at 6 to 8 weeks
Approach: Posterior popliteal fossa exploration (S-shaped or zig-zag incision)
Identify: Medial head of gastrocnemius, popliteal artery and vein, tibial nerve
Myotomy: Divide the medial head of gastrocnemius at its musculotendinous junction, ensuring full decompression of the popliteal artery through the full range of ankle motion intra-operatively
Verify: Intra-operative duplex or palpable distal pulses through full ankle ROM
Mobilise: Weight-bearing as tolerated from post-operative day 1
Splint: Short period of ankle neutral splint (24 to 48 hours) for wound healing
Monitor: Distal pulses, wound healing, calf swelling
Anticoagulation: Not routinely required unless arterial repair performed
Progressive activity: Graduated running programme from 4 weeks
Full sport: Usually cleared at 6 to 8 weeks
Follow-up: Duplex ultrasound at 6 weeks and 12 months to confirm decompression and arterial patency
For functional PAES, myotomy alone is curative in 85 to 95 percent of cases because the artery itself is normal. The key is complete division of the medial gastrocnemius head with intra-operative verification of arterial patency through full ankle range of motion. Failure to divide the muscle completely is the most common cause of recurrent symptoms.
R-E-L-I-E-FSurgical Management Steps
Hook:RELIEF is what the athlete gets after proper surgical decompression!
Complications
- Incidence
- 10 to 20 percent of untreated anatomical PAES
- Risk Factors
- Delayed diagnosis, Type I-III entrapment
- Management
- Urgent revascularisation + entrapment release
- Incidence
- 5 to 10 percent of chronic PAES
- Risk Factors
- Long-standing entrapment, post-stenotic dilatation
- Management
- Aneurysm repair + entrapment release
- Incidence
- 5 to 15 percent
- Risk Factors
- Incomplete myotomy, arterial wall damage not addressed
- Management
- Repeat imaging; consider completion myotomy or bypass
- Incidence
- 5 to 10 percent at 5 years
- Risk Factors
- Poor vein quality, technical error, ongoing compression
- Management
- Revision bypass or endovascular salvage
- Incidence
- 5 to 10 percent
- Risk Factors
- Posterior incision, re-operation, obesity
- Management
- Wound care, antibiotics, delayed mobilisation
- Incidence
- Less than 5 percent
- Risk Factors
- Incomplete muscle division, scar tissue
- Management
- Revision surgery with wider decompression
Untreated PAES follows a predictable pathological course: repeated arterial compression leads to intimal fibrosis, which progresses to fibrous stenosis, post-stenotic dilatation, and eventually thrombosis or aneurysm formation. Young patients with anatomical PAES should be offered surgical decompression even if asymptomatic, because the natural history is one of progressive arterial damage. Functional PAES may be observed if symptoms are mild, but surgery is indicated for competitive athletes and those with documented arterial wall changes.
Outcomes and Prognosis
- Treatment
- Myotomy alone
- Expected Outcome
- 85 to 95 percent symptom resolution
- Long-term Function
- Full return to sport at 6 to 8 weeks
- Treatment
- Muscle resection + decompression
- Expected Outcome
- 80 to 90 percent symptom resolution
- Long-term Function
- Full return to sport at 8 to 12 weeks
- Treatment
- Resection + vein bypass graft
- Expected Outcome
- 70 to 85 percent graft patency at 5 years
- Long-term Function
- Return to sport at 3 to 6 months, may have activity limits
- Treatment
- Emergency revascularisation + release
- Expected Outcome
- 60 to 80 percent limb salvage
- Long-term Function
- Variable; depends on ischaemia time and muscle damage
Best prognosis: Functional PAES with myotomy alone (normal artery, simple decompression)
Good prognosis: Anatomical PAES diagnosed early before arterial wall damage
Guarded prognosis: Late presentation with popliteal artery thrombosis or aneurysm requiring bypass
Poor prognostic indicators: Delayed diagnosis over 12 months, acute limb ischaemia at presentation, popliteal artery occlusion with poor run-off
Guidelines, Registries & Global Practice
- PAES prevalence: Anatomical variants found in approximately 3 to 5 percent of cadaveric specimens globally
- Athlete predominance: Reported worldwide in runners, cyclists, rowers, footballers, and military recruits
- Functional PAES: Most common form in athletes; incidence increasing with recognition and dynamic imaging
- Late presentation: Average diagnostic delay of 12 to 24 months reported across centres in Europe, North America, and Australasia
- High-resource: MR angiography with provocative positioning as first-line dynamic imaging; posterior surgical approach with intra-operative duplex
- Limited-resource: Dynamic duplex ultrasound with provocative manoeuvres is a low-cost, high-yield alternative; open myotomy with clinical verification of decompression
- Universal principle: The diagnosis is clinical (young athlete + provocative pulse loss); imaging confirms and classifies
- Surgery: Posterior popliteal approach is the global standard; arterial reconstruction techniques vary by surgeon training
- Diagnosis Emphasis
- Provocative pulse testing in all young claudicants
- Imaging
- Dynamic duplex first-line; MR/CT angio for surgical planning
- Surgery
- Myotomy for functional; resection + bypass if artery diseased
- Diagnosis Emphasis
- High index of suspicion in athletes; check bilateral pulses
- Imaging
- CTA or MRA with provocative positioning; duplex screening
- Surgery
- Surgical decompression; endovascular has limited role (external compression)
- Diagnosis Emphasis
- Differentiate from CECS with pulse examination
- Imaging
- Bilateral imaging mandatory; dynamic protocol essential
- Surgery
- Early referral to vascular surgery; myotomy curative for functional PAES
There is no dedicated international registry for PAES due to its rarity. The evidence base comprises case series, systematic reviews of pooled series, and expert consensus. ESVS guidelines recommend dynamic imaging and early surgical decompression. The key message for exams: PAES is rare but important as a cause of young-person claudication, and the diagnosis is often delayed. A simple provocative pulse test can be diagnostic.
Record in any young patient with exertional calf pain:
- Provocative pulse testing performed and result (positive or negative)
- Bilateral pulse assessment in resting and provoked positions
- Differential diagnosis considered (PAES, CECS, cystic adventitial disease, radiculopathy)
- Imaging requested with dynamic provocative protocol specified
- If PAES confirmed, bilateral imaging and early vascular surgical referral
Missed PAES leading to popliteal artery thrombosis is a preventable cause of acute limb ischaemia in young patients. Always perform provocative pulse testing in any young person with exertional calf symptoms.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old competitive rower presents with a 6-month history of reproducible left calf pain and foot numbness during training. The pain resolves within 2 minutes of rest. He has no medical history and does not smoke. Resting examination reveals normal palpable pedal pulses bilaterally. When you ask him to actively plantarflex against resistance, the left dorsalis pedis pulse disappears. What is your diagnosis, investigation, and management?”
“A 32-year-old military recruit presents to the emergency department with a 4-hour history of sudden onset severe left calf pain, foot pallor, and numbness. He reports a 2-year history of intermittent calf pain during training that was attributed to shin splints. Examination reveals an absent left dorsalis pedis pulse, cold pale foot with reduced sensation, and intact motor function. CT angiography shows a short segment popliteal artery occlusion with an anomalous medial gastrocnemius head compressing the vessel. How would you manage this?”
Key Anatomy
- Popliteal artery passes between medial and lateral gastrocnemius heads through the popliteal fossa
- Anomalous medial gastrocnemius head is the most common compressive structure
- Popliteus muscle and fibrous bands can also entrap (Type IV)
- Bilateral anatomical variants present in 60 to 70 percent of cases on imaging
Diagnosis
- Young athlete (under 40) with calf claudication and no atherosclerotic risk factors
- Provocative pulse testing: active plantarflexion or passive dorsiflexion abolishes pedal pulses
- Dynamic MR or CT angiography with provocative positioning is the gold standard
- Always image both legs and order dynamic (not resting-only) imaging
Classification (Love-Whelan)
- Types I-III: Anatomical variants of gastrocnemius-artery relationship
- Type IV: Popliteus or fibrous band compression
- Type V: Any anatomical type with coexisting venous entrapment
- Type VI (Functional): Normal anatomy, hypertrophied muscle compresses artery on exercise
Treatment Algorithm
- Functional PAES (Type VI): Myotomy of medial gastrocnemius head alone (85 to 95 percent cure)
- Anatomical PAES with normal artery: Resection of anomalous tissue + decompression
- Anatomical PAES with diseased artery: Resection + interposition saphenous vein graft
- Acute thrombosis: Urgent thrombectomy + bypass + entrapment release + consider fasciotomy
PAES vs CECS Differential
- PAES: vascular symptoms (pallor, cold foot, pulse loss) with normal compartment pressures
- CECS: myofascial burning pain with raised compartment pressures and normal pulses
- Both can coexist and must be investigated independently
- Dynamic duplex and compartment pressure studies are complementary investigations
Evidence Base and Key Trials
Popliteal artery entrapment syndrome
- Original description of the anatomical classification of popliteal artery entrapment
- Identified the medial head of gastrocnemius as the primary compressive structure
- Established the concept of anomalous musculo-arterial relationships causing claudication in young patients
- Recommended surgical exploration and division of the anomalous muscle fibres
Functional popliteal artery entrapment syndrome: A poorly understood and often missed diagnosis that is frequently mistreated
- Distinguished functional from anatomical PAES as separate entities requiring different surgical strategies
- Functional PAES is the most common form in athletes, with normal anatomy but muscle hypertrophy causing compression
- Myotomy of the medial gastrocnemius head is curative for functional PAES without arterial reconstruction
- Recommended dynamic imaging with provocative manoeuvres for diagnosis
Popliteal entrapment syndrome
- Systematic review of published series totalling over 300 cases of PAES in athletes
- Functional entrapment accounted for the majority of cases in the athletic population
- Myotomy alone achieved symptom resolution in over 85 percent of functional PAES cases
- Arterial reconstruction was required in approximately 30 percent of anatomical PAES cases
- Bilateral imaging abnormalities were found in approximately 60 percent of patients
Long-term outcomes after revascularization for advanced popliteal artery entrapment syndrome with segmental arterial occlusion
- Long-term follow-up of surgical myotomy and arterial reconstruction for PAES with segmental occlusion
- Autologous vein bypass for diseased arteries achieved durable patency in the majority of patients
- Early intervention before arterial wall damage develops leads to superior long-term outcomes
- Incomplete myotomy was identified as a primary cause of recurrent symptoms
Popliteal artery entrapment syndrome
- Comprehensive review of PAES classification, diagnostic modalities, and management strategies
- Dynamic duplex ultrasound with provocative manoeuvres is the recommended first-line non-invasive investigation
- Greater than 50 percent velocity increase or complete flow cessation during plantarflexion is diagnostic
- Resting ultrasound alone misses functional PAES; dynamic imaging protocol is essential
- MR or CT angiography with provocative positioning is the gold standard for surgical planning