The femoral head sinks too deep into the pelvis | Primary (idiopathic) or secondary to bone-softening or inflammatory disease | Diagnosed on the AP pelvis | THA restores the hip centre and grafts the medial defect
- Protrusio acetabuli means the femoral head has migrated medially, sinking past the ilioischial (Kohler) line so the head lies deep within the pelvis - the joint centre is medialised and the bone medial to the head is deficient
- Most protrusio is secondary - always hunt for an underlying cause (inflammatory arthritis, a bone-softening metabolic disease, Marfan syndrome, trauma, tumour, or infection) before labelling it primary or idiopathic
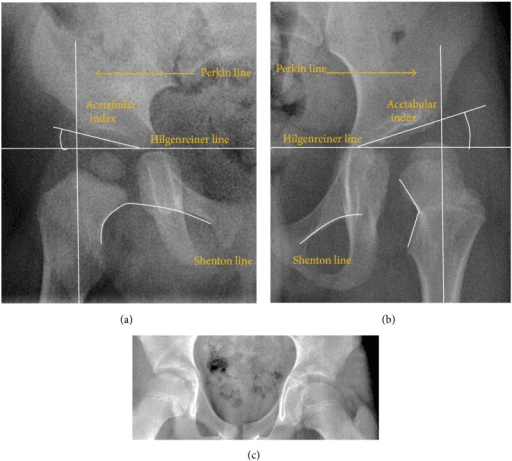
- It is diagnosed on a plain AP pelvis radiograph: the medial wall of the acetabulum lies medial to the ilioischial line, and the lateral centre-edge angle is high (greater than 40 degrees) - the opposite of the shallow, uncovered hip of dysplasia
- In the young hip with little arthritis, treatment aims to stop progression - valgus intertrochanteric osteotomy in the adult, and triradiate cartilage closure in the growing child
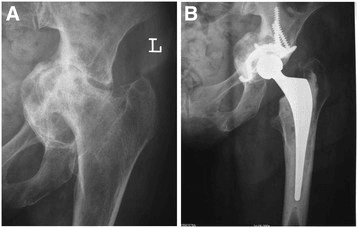
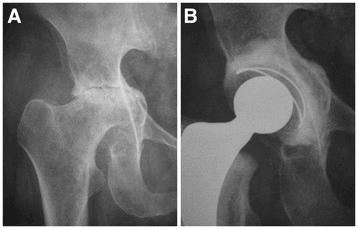
- Total hip arthroplasty is the definitive treatment once the hip is arthritic: the key principles are to lateralise the cup back to the true hip centre and to bone-graft the medial defect, usually with morsellised femoral head autograft
- “The single best test is an AP pelvis radiograph - protrusio is present when the femoral head or medial acetabular wall sits medial to the ilioischial (Kohler) line
- “Protrusio is the mirror image of dysplasia: dysplasia is a shallow socket with a low centre-edge angle, protrusio is a deep socket with a high centre-edge angle
- “New bilateral protrusio in a tall young patient should prompt a search for Marfan syndrome
- “The two THA principles examiners want to hear are restore the hip centre (lateralise the cup) and graft the medial defect with morsellised autograft
Protrusio acetabuli is medial migration of the femoral head into the pelvis, so that the head or medial acetabular wall lies medial to the ilioischial (Kohler) line. The hip centre is medialised and the medial acetabular bone is deficient - the opposite of the shallow, uncovered dysplastic hip.
Always look for a cause: inflammatory arthritis (rheumatoid, ankylosing spondylitis), bone-softening disease (osteomalacia, Paget, osteogenesis imperfecta), Marfan syndrome, trauma, tumour, or infection. Primary (idiopathic) protrusio is a diagnosis of exclusion.
Made on a plain AP pelvis. The medial wall lies medial to the ilioischial line, and the lateral centre-edge angle is high (greater than 40 degrees). The acetabular line crossing medial to the ilioischial line is the classic radiographic sign.
For arthroplasty, examiners want: restore the hip centre by lateralising the cup back to the true (anatomical) position, and bone-graft the medial defect, usually with morsellised femoral head autograft. Rely on the intact peripheral rim for press-fit, not on screws into thin medial bone.
Overview
Protrusio acetabuli describes a hip in which the femoral head has sunk too deep into the acetabulum, migrating medially so that the head and the floor of the socket bulge into the pelvis. The defining radiographic feature is that the medial wall of the acetabulum (or the femoral head itself) lies medial to the ilioischial line - the line that marks the normal medial border of the joint.
It is best understood as the mirror image of hip dysplasia. In dysplasia the socket is shallow and the head is uncovered (a low centre-edge angle); in protrusio the socket is too deep and the head is over-covered (a high centre-edge angle). Both deformities change where the load passes through the joint and both lead to early arthritis, but they need opposite reconstructions - lateralising and deepening for the dysplastic hip, and lateralising the cup back out of the pelvis for the protrusio hip.
For the exam, three things matter: knowing the causes (and that most cases are secondary), being able to diagnose and measure it on a plain radiograph, and understanding the principles of reconstruction, particularly the two rules of total hip arthroplasty - restore the hip centre and graft the medial defect.
Anatomy and Pathophysiology
The normal acetabulum is a deep, hemispherical socket whose medial wall is supported by the thick bone of the quadrilateral plate and stabilised by the surrounding bony columns. In a healthy hip the medial acetabular wall lies lateral to (outside) the ilioischial line, and load passing from the femoral head is spread across the dome and the columns.
How protrusio develops:
- The deformity occurs when the medial acetabular bone is too weak to resist the force transmitted by the femoral head, or when that force is abnormally high. Over time the head pushes the medial wall progressively into the pelvis.
- In bone-softening disease (osteomalacia, Paget disease, osteogenesis imperfecta) the periacetabular bone itself is weak and gradually yields.
- In inflammatory arthritis (rheumatoid, ankylosing spondylitis) synovitis erodes the medial wall and central cartilage, and the softened bone migrates medially.
- In primary (idiopathic) protrusio there is no clear underlying disease - it is typically bilateral and more common in middle-aged women. When severe and bilateral it has historically been called an Otto pelvis.
Why it causes symptoms:
As the head migrates medially the hip centre is displaced, which shortens the effective offset and the lever arm of the abductors, leading to a weak, sometimes limping gait. The deep socket causes impingement of the femoral neck against the rim, limiting movement (especially abduction and rotation), and the abnormal load distribution drives secondary osteoarthritis. Late in the disease the patient presents with progressive pain and stiffness.
- Protrusio acetabuli
- Too deep - head sunk into the pelvis
- Developmental dysplasia
- Too shallow - head uncovered
- Protrusio acetabuli
- High (greater than 40 degrees) - over-coverage
- Developmental dysplasia
- Low (less than 20 to 25 degrees) - under-coverage
- Protrusio acetabuli
- Wall lies medial to the line
- Developmental dysplasia
- Wall lies lateral to the line (normal or more lateral)
- Protrusio acetabuli
- Lateralise the cup outward, graft the medial defect
- Developmental dysplasia
- Place cup at the true centre, may need superolateral graft
Classification
The most useful classification for the exam is simply primary versus secondary, because it drives the search for an underlying cause. Severity can then be graded by how far the femoral head lies medial to the ilioischial line.
- Primary (idiopathic) protrusio acetabuli - no identifiable underlying disease. It is usually bilateral, more common in middle-aged women, and is a diagnosis of exclusion once secondary causes have been ruled out. The severe bilateral form is the historical Otto pelvis.
- Secondary protrusio acetabuli - the result of an identifiable disease that weakens periacetabular bone or increases central load. This is the larger group and the one examiners expect you to work through.
Clinical Presentation
Protrusio is often silent for years and only declares itself when secondary arthritis develops. The history and examination are aimed both at the hip and at the underlying cause.
Progressive groin pain and stiffness, often gradual. Patients notice loss of movement (especially abduction and rotation) before pain becomes severe. Ask about features of inflammatory arthritis and a family history suggesting Marfan or other connective-tissue disease.
Reduced and painful range of movement, particularly abduction, external and internal rotation, because the deep socket causes impingement. Look for a fixed flexion deformity, leg-length difference, and an abductor (Trendelenburg) limp from the medialised hip centre.
Examine for signs of rheumatoid arthritis (hand and other joint involvement), ankylosing spondylitis (stiff spine, reduced chest expansion), and the marfanoid habitus (tall stature, long limbs, arachnodactyly, high-arched palate, lens or aortic problems).
Primary protrusio and the connective-tissue and metabolic causes are typically bilateral, so always examine and image both hips even when only one is painful.
Investigations
- What it shows
- Medial wall or head medial to the ilioischial line; high centre-edge angle; deep socket
- Why it matters
- The single key diagnostic test - confirms protrusio and grades severity
- What it shows
- Anterior and posterior wall and overall coverage
- Why it matters
- Help plan reconstruction and assess impingement
- What it shows
- Three-dimensional bone stock, wall and column integrity
- Why it matters
- Templates the cup and shows how much medial bone graft is needed
- What it shows
- Inflammatory markers, rheumatoid serology, calcium, phosphate, vitamin D, ALP, PTH
- Why it matters
- Identifies inflammatory or bone-softening causes
- What it shows
- Genetic and clinical assessment for Marfan or other connective tissue disease
- Why it matters
- A new bilateral protrusio in a young patient needs a cause
Measuring it on the radiograph
The diagnosis rests on the AP pelvis:
- Ilioischial (Kohler) line - the diagnosis is made when the medial acetabular wall or the femoral head lies medial to this line. This is the most important single sign.
- Lateral centre-edge angle of Wiberg - high (greater than 40 degrees) in protrusio, reflecting over-coverage of the head (the opposite of the low angle of dysplasia).
- Acetabular crossing - quantifying how far the floor lies medial to the ilioischial line grades severity and helps planning.
Quantitative criteria (Armbuster): the commonly quoted measurement thresholds define protrusio when the acetabular line lies medial to the ilioischial (Kohler) line by at least 3 mm in men, 6 mm in women, and 3 mm in children. Combined with a centre-edge angle greater than 40 degrees, these figures turn the qualitative "crosses the line" sign into a measurable diagnosis.
A classic exam pairing distinguishes the two by which structure crosses the ilioischial (Kohler) line. In coxa profunda the floor of the acetabular fossa touches or lies medial to the ilioischial line, but the femoral head stays lateral to it - a deep but milder over-coverage that sits within the pincer-type femoroacetabular impingement / acetabular over-coverage spectrum. In protrusio acetabuli the femoral head itself migrates medial to the ilioischial line. So: profunda = the floor crosses the line; protrusio = the head crosses the line. (Note coxa profunda is common even in asymptomatic hips, so its clinical significance is debated and it should not be over-treated; protrusio is the more clearly pathological, progressive entity.)
Read protrusio against dysplasia. If the femoral head is uncovered with a low centre-edge angle, think dysplasia; if the head is buried deep in a socket that crosses the ilioischial (Kohler) line with a high centre-edge angle, think protrusio. The reconstruction is the opposite in each: deepen and cover the dysplastic socket, but lateralise the protrusio cup back out of the pelvis.

Management
Management depends on the age of the patient, the underlying cause, and how much arthritis has developed. The aim early in the disease is to halt progression; once the hip is arthritic the aim is reconstruction.
- Treat the underlying cause - medical control of inflammatory arthritis and correction of metabolic bone disease (vitamin D, treatment of osteomalacia or Paget disease) can slow progression and are essential before considering surgery.
- Skeletally immature child - if recognised before the triradiate cartilage closes, closure or arrest of the triradiate cartilage (sometimes combined with a femoral osteotomy) can stop further medial migration.
- Young adult, minimal arthritis - a valgus intertrochanteric proximal femoral osteotomy redirects load and can relieve symptoms and slow progression while the patient's own joint is preserved.
Surgical Technique
The technically demanding part of the operation is the acetabular reconstruction. The femoral side is usually managed as in routine arthroplasty, but careful templating of offset and leg length is essential because protrusio distorts both.
- Use a familiar approach (posterior, direct lateral, or direct anterior) - the choice matters less than safe delivery of an often incarcerated femoral head from a deep socket.
- Because the head sits deep within the pelvis, dislocation can be difficult and can fracture fragile bone; an in-situ femoral neck cut to deliver the head in pieces is a safe option when dislocation is risky.
- Preserve the resected femoral head - it is the source of morsellised autograft for the medial defect.
Complications
- Why it happens
- Cup seated in the deep medial defect
- How to limit it
- Lateralise the cup and graft the medial defect to rebuild the true centre
- Why it happens
- Poor initial fixation in deficient or grafted medial bone
- How to limit it
- Press-fit on the intact rim; cage or ring if the rim is inadequate
- Why it happens
- Reaming or impacting into thin, soft medial bone
- How to limit it
- Gentle technique, recognise fragile bone, protect the medial wall
- Why it happens
- Failure of the medial bone graft to incorporate
- How to limit it
- Use morsellised autograft on a viable, well-prepared bed
- Why it happens
- Soft-tissue trauma during a demanding reconstruction
- How to limit it
- Recognised common complication - usually managed conservatively
- Why it happens
- Complex deformity not planned for
- How to limit it
- Careful pre-operative templating of both hips
In severe protrusio the femoral head can be incarcerated within the cavernous acetabulum, making dislocation at surgery difficult and risking fracture of fragile bone. Plan the approach, consider an in-situ neck cut to deliver the head safely, and handle soft, osteoporotic medial bone with care.
Postoperative Care and Rehabilitation
- Weight-bearing - many surgeons protect weight-bearing for a period after a medially grafted reconstruction to allow the bone graft to incorporate before full load is applied; the exact regimen depends on the quality of fixation and the surgeon's judgement.
- Thromboprophylaxis and early mobilisation - standard arthroplasty venous thromboembolism prophylaxis and supervised physiotherapy to restore movement and abductor strength, which is often weak because of the previously medialised hip centre.
- Manage the underlying disease - continue medical control of inflammatory arthritis and treatment of metabolic bone disease, and review steroid and disease-modifying therapy with the rheumatology team to support bone healing and reduce infection risk.
- Follow-up imaging - serial radiographs to confirm the graft has incorporated, the cup remains well-fixed, and the restored hip centre is maintained, with attention to any sign of medial migration or loosening.
Outcomes and Prognosis
Published series of total hip arthroplasty for protrusio report good and durable results when the principles are followed - particularly the use of an uncemented cup with bone grafting of the medial defect and restoration of the hip centre.
- A systematic review of 18 studies (783 hips, mean follow-up about 8.9 years) found good outcomes with uncemented cups plus bone graft, identified restoration of the anatomical hip centre as paramount for durability, and noted that routine screw augmentation is not recommended.
- The commonest complications across series were aseptic loosening (which required revision) and heterotopic ossification (usually managed conservatively).
- A cohort using press-fitted cups reported that stable, well-fixed cups did well even when the centre was slightly medialised, with similar hip scores whether the centre was fully restored or left medialised - underlining that solid initial fixation on the rim is the key driver of a good result.
- Overall the prognosis after well-executed reconstruction is comparable to routine arthroplasty, while the natural history without treatment is progressive medial migration, stiffness and secondary osteoarthritis.
Guidelines, Registries & Global Practice
- No single international guideline governs protrusio acetabuli specifically; practice rests on the age-based treatment ladder described in classic reviews - triradiate cartilage closure in the child, valgus intertrochanteric osteotomy in the young adult with a preserved joint, and total hip arthroplasty once the hip is arthritic.
- The consensus on reconstruction across published series is consistent worldwide: use an uncemented cup with bone grafting of the medial defect, aim to restore the hip centre, rely on the intact peripheral rim for fixation, and avoid routine screw augmentation - the principles confirmed by the 2024 systematic review.
- Registry data (NJR, AJRR, AOANJRR and the Scandinavian registries) do not track protrusio as a separate diagnosis, but their broad message applies: well-fixed uncemented cups on supportive bone do well, and reconstructions that fail to achieve solid initial fixation are at higher risk of aseptic loosening and revision.
- Global practice variation mainly reflects the underlying disease mix and resource setting - inflammatory arthritis dominates where rheumatology care identifies these hips, while access to CT planning, modern uncemented cups and reinforcement cages varies between settings rather than any disagreement on the surgical principles.
Memory aids
PROTRUDESCauses of Secondary Protrusio
Hook:The femoral head PROTRUDES through the medial wall - the letters list the diseases that let it happen.
DEEPReading the AP Pelvis for Protrusio
Hook:A protrusio hip is DEEP - deep socket, high edge angle, crosses the Kohler line on the plain film.
GRAFTTHA Principles for Protrusio
Hook:Think GRAFT for the protrusio THA - Graft, Restore the centre, Anchor on the rim, Fixation by rim not medial screws, Template.
MCQ Practice Points
Q: A 55-year-old woman has bilateral hips where the medial acetabular wall lies medial to the ilioischial line, with a centre-edge angle of 45 degrees. What is the diagnosis? A: Protrusio acetabuli - medialisation past the ilioischial (Kohler) line with a high centre-edge angle (greater than 40 degrees) is the defining picture. A low centre-edge angle with an uncovered head would instead be dysplasia.
Q: A 24-year-old tall man with arachnodactyly has bilateral protrusio and minimal arthritis. What is the best next step? A: Assess for Marfan syndrome and, for the hip, choose joint-preserving surgery (valgus intertrochanteric osteotomy) rather than arthroplasty, because he is young with a preserved joint.
Q: At total hip arthroplasty for protrusio, what are the two key reconstruction principles? A: Restore the hip centre by lateralising the cup to the true position, and bone-graft the medial defect with morsellised femoral head autograft, fixing on the intact peripheral rim. Routine screw augmentation is not recommended.
Protrusio is present when the medial acetabular wall or femoral head lies medial to the ilioischial (Kohler) line on the AP pelvis. This single fact is the most commonly tested point.
The lateral centre-edge angle is high (greater than 40 degrees) in protrusio (over-coverage) and low in dysplasia (under-coverage). Examiners love this opposite pairing.
The favourite distractor is calling it primary. Rheumatoid arthritis is the classic secondary cause; primary (idiopathic) protrusio is a diagnosis of exclusion in middle-aged women and is the basis of the Otto pelvis.
The correct reconstruction is to lateralise the cup to the true hip centre and bone-graft the medial defect with morsellised autograft, fixing on the intact rim. Routine screw augmentation is the wrong answer.
For the young hip with minimal arthritis the answer is a valgus intertrochanteric osteotomy (or triradiate closure in a child), not arthroplasty.
A tall young patient with bilateral protrusio is a classic prompt to choose Marfan syndrome as the underlying cause.
At a Glance
- Answer
- Medial migration of the femoral head into the pelvis, past the ilioischial (Kohler) line
- Answer
- AP pelvis - medial wall medial to the ilioischial line, centre-edge angle greater than 40 degrees
- Answer
- Mostly secondary - find the cause; primary is bilateral, middle-aged women, diagnosis of exclusion
- Answer
- Inflammatory arthritis (rheumatoid, ankylosing spondylitis); also bone-softening disease and Marfan
- Answer
- Valgus intertrochanteric osteotomy (adult); triradiate closure (child)
- Answer
- Total hip arthroplasty - restore the hip centre and graft the medial defect
- Answer
- Protrusio is dysplasia's mirror image - deep socket, high centre-edge angle
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are shown an AP pelvis radiograph of a 55-year-old woman with bilateral deep-seated hips. The examiner asks what protrusio acetabuli is and how you would confirm and investigate it.”
“A 62-year-old woman with long-standing rheumatoid arthritis has a painful, stiff right hip. The radiograph shows protrusio with secondary osteoarthritis. She wants surgery. How would you plan and perform the reconstruction?”
“A 24-year-old man is found to have bilateral protrusio with only mild joint space change. He is tall with long fingers. How would you approach him?”
Definition
- Medial migration of the femoral head into the pelvis
- Head or medial wall lies medial to the ilioischial (Kohler) line
- Lateral centre-edge angle high (greater than 40 degrees) - over-coverage
- The mirror image of dysplasia
Causes
- Most are secondary - always find the cause
- Inflammatory: rheumatoid arthritis, ankylosing spondylitis
- Bone-softening: osteomalacia, Paget, osteogenesis imperfecta
- Connective tissue: Marfan and Ehlers-Danlos; also trauma, tumour, infection
- Primary (idiopathic) - bilateral, middle-aged women, diagnosis of exclusion (Otto pelvis)
Management Ladder
- Treat the underlying cause first
- Child: closure or arrest of the triradiate cartilage
- Young adult, minimal arthritis: valgus intertrochanteric osteotomy
- Arthritic hip: total hip arthroplasty
THA Principles
- Restore the hip centre - lateralise the cup to the true position
- Graft the medial defect with morsellised femoral head autograft
- Press-fit on the intact rim; cage or ring if the rim is deficient
- Avoid relying on medial screws; template offset and leg length
Evidence Base and Key Studies
Total Hip Arthroplasty in Protrusio Acetabuli (Systematic Review)
- Systematic review of 18 studies (8 prospective, 10 retrospective) covering 783 hips, mean age 60 years, followed for a mean of about 8.9 years
- Eighty percent of patients were female and most had inflammatory arthritis as the underlying cause
- Good outcomes were achieved with uncemented cups combined with bone graft, with restoration of the anatomical hip centre highlighted as paramount for durability
- Screw augmentation for fixation was not recommended unless absolutely necessary; the commonest complications were aseptic loosening (needing revision) and heterotopic ossification (managed conservatively)
Is Restoration of the Hip Centre Mandatory in THA for Protrusio?
- Retrospective review of 26 cementless THAs in 22 patients with protrusio, mean follow-up 5.1 years
- Press-fit of the cup was prioritised over hip-centre restoration; the centre was restored in 17 cups and left medialised in 9
- All 26 cups remained stable at final follow-up, including the medialised press-fitted cups
- Modified Harris Hip Scores were similar between the restored and medialised groups (about 83.6 versus 83.8)