Avulsions | Tendinopathy | Sciatic Nerve
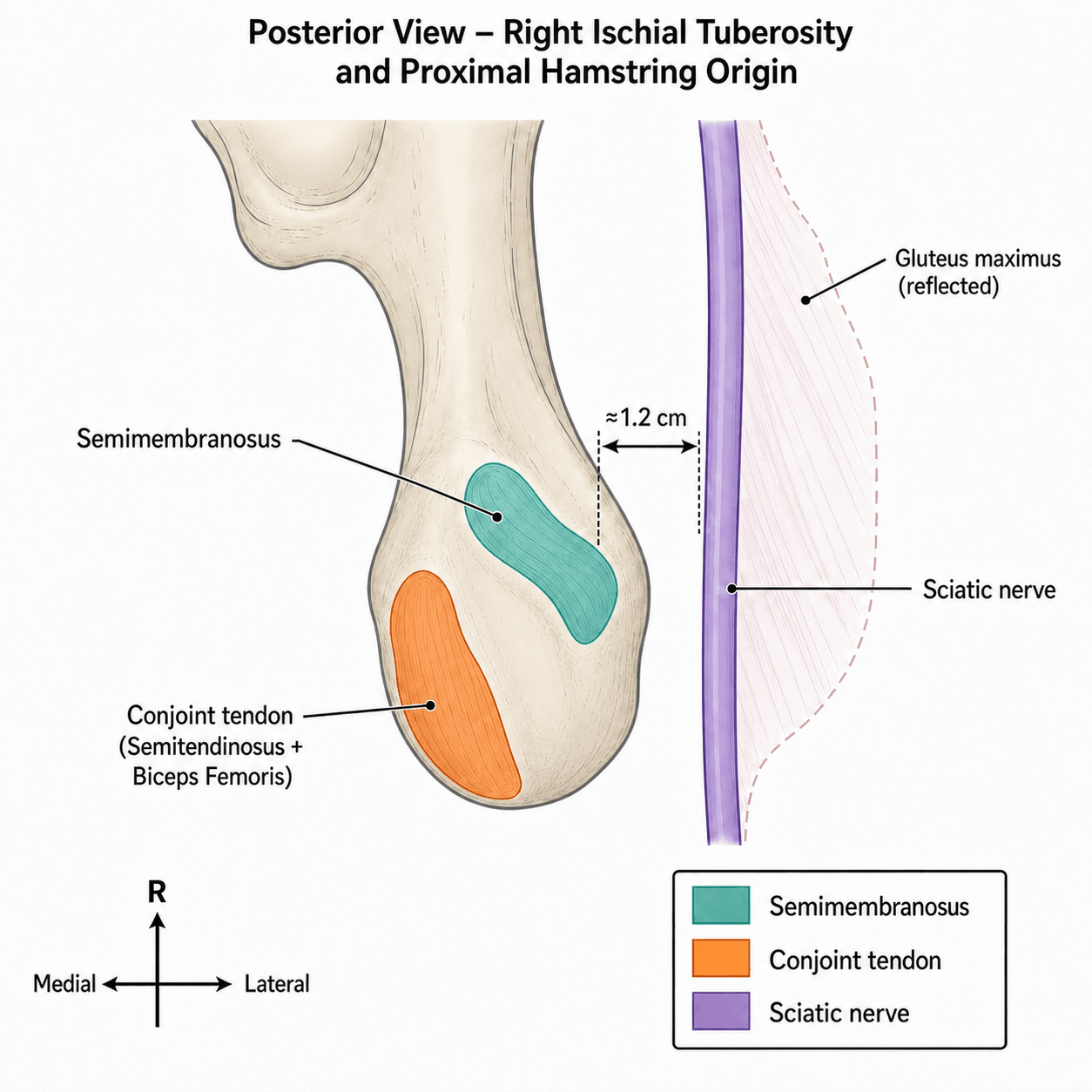
- Anatomy: Semimembranosus origin is superolateral on the tuberosity; the conjoint tendon (semitendinosus + biceps long head) is posteromedial. Biceps short head (linea aspera) is spared.
- Mechanism: Forced hip flexion with the knee extended (waterskiing, doing the splits, slip on wet floor).
- Sciatic Nerve: Runs about 1.2cm lateral to the ischial tuberosity; scars to the stump in chronic tears, so neurolysis is part of the operation.
- Surgery Indications: 2-to-3 tendon avulsion with retraction over 2cm in an active patient; any tear with sciatic symptoms.
- Rehab: Avoid the at-risk position (hip flexion + knee extension) for roughly 6 weeks post-op.
- “Bowstring Sign: Active knee flexion at 90 deg hip flexion - absent cord.
- “Ecchymosis in posterior thigh is a pathognomic delayed sign.
- “MRI is gold standard for grading retraction.
- “Chronic repairs (greater than 4 weeks) often need allograft or lysis of adhesions.
The Peril. The sciatic nerve is intimately related to the proximal hamstring origin (approx 1.2cm lateral). In chronic cases, it is scarred to the stump. Neurolysis is mandatory during repair.
The 4 Week Window. Prognosis drops significantly after 4 weeks due to tendon retraction and scarring. Acute repair (less than 4 weeks) is much easier than chronic reconstruction.
- Proximal Avulsion
- Forced Hip Flexion (Waterski)
- Mid-substance Strain
- Running/Sprinting
- Distal Avulsion
- Direct Blow/Cut
- Proximal Avulsion
- Ischial Tuberosity
- Mid-substance Strain
- Musculotendinous Junction
- Distal Avulsion
- Pes Anserinus/Fibula
- Proximal Avulsion
- Massive Posterior Thigh
- Mid-substance Strain
- Localised
- Distal Avulsion
- Knee region
- Proximal Avulsion
- Surgery (if retracted)
- Mid-substance Strain
- Conservative
- Distal Avulsion
- Depends on ligament
Semi-MembranousHamstring Muscles
Hook:Semi-T and Biceps are joined at the hip.
Flex-ExtRehab Danger Zone
Hook:Don't combine Flexion and Extension.
Overview and Epidemiology
Proximal hamstring injuries range from minor strains to complete avulsions. Complete avulsions are devastating injuries in athletes, leading to significant weakness and loss of function if missed.
- Mechanism: Rapid eccentric contraction. Forced hip flexion with knee extension.
- Water skiing (getting up).
- Bull riding.
- Gymnastics (splits).
- Slipping on wet floor (splits).
- Demographics:
- Young Athletes: Epiphyseal avulsions (ischial apophysis).
- Middle-aged: Tendinous avulsions (degeneration).
Pathophysiology and Mechanisms
Hamstring Origin
All originate from Ischial Tuberosity.
- Semimembranosus: Originates from the superolateral impression. It has the largest footprint.
- Conjoint Tendon: Semitendinosus and Biceps Femoris (Long Head). Originates from the posteromedial impression.
Note: Biceps Short Head originates from the Linea Aspera (Femur), not the ischium, so it is spared in avulsions.
The ischial tuberosity is divided into upper and lower facets; the semimembranosus footprint is the largest of the three.
Classification Systems
Wood Classification (MRI based)
Described by Wood et al in their JBJS series of 72 reconstructions (2008).
- Type 1: Osteo-apophyseal (bony) avulsion, typically adolescent.
- Type 2: Musculotendinous junction avulsion.
- Type 3: Incomplete tendinous avulsion.
- Type 4: Complete tendinous avulsion off bone with minimal/no retraction.
- Type 5: Complete avulsion with significant retraction or sciatic nerve involvement (most severe).
Practical descriptor
Most surgeons now describe tears functionally by number of tendons involved (1, 2 or 3) and retraction (under 2cm versus over 2cm). This drives the operative decision more directly than the type number alone.
Clinical Assessment
History
- "Pop" or "tearing" sensation in the buttock.
- Falls while doing splits.
- Immediate pain, inability to walk without limp.
- Sciatic symptoms: Numbness, foot drop (rare but urgent).
Physical Examination
- Inspection: "Hamstring Droop" (loss of proximal contour). Extensive ecchymosis (bruising) tracking down to knee (appears days later).
- Palpation: Defect at ischial tuberosity. Tender.
- Strength: Weakness in Knee Flexion and Hip Extension.
- Note: Knee flexion may still be present due to intact Biceps Short Head, Gracilis, and Sartorius.
- Bowstring Sign: Patient prone, knee flexed to 90. Palpate distal tendons. If "bowstringing" is absent or asymmetrical, suggests avulsion.
Investigations

X-Ray
- AP Pelvis: Rule out bony avulsion (Ischial tuberosity fracture).
- Particularly important in adolescents (apophysis).
MRI
- Gold Standard.
- Determines:
- Number of tendons involved (1, 2, or 3).
- Amount of retraction (cm).
- Sciatic nerve involvement.
- Chronicity (fatty atrophy).
Ideally obtained within 2 weeks of injury.
Differential Diagnosis
Buttock and posterior-thigh pain has several mimics. The discriminators below separate a true proximal hamstring avulsion from its common look-alikes.
- Key Discriminator
- Acute pop + extensive posterior-thigh ecchymosis, palpable ischial gap
- Best Test
- MRI (number of tendons + retraction)
- Key Discriminator
- Gradual deep buttock pain worse with sitting/sprinting, no acute pop
- Best Test
- MRI shows tendinosis, no full-thickness gap
- Key Discriminator
- Point tenderness over tuberosity, no strength loss
- Best Test
- MRI/US fluid at bursa
- Key Discriminator
- Sciatic-type leg pain, positive seated piriformis/slump
- Best Test
- MRI plus nerve assessment
- Key Discriminator
- Skeletally immature, bony fragment on X-ray
- Best Test
- AP pelvis radiograph
- Key Discriminator
- Musculotendinous junction tenderness, no ischial gap
- Best Test
- MRI shows oedema at MTJ
- Key Discriminator
- Back pain, dermatomal radiation, neuro deficit
- Best Test
- MRI lumbar spine
Proximal (High) Hamstring Tendinopathy
This topic's title spans avulsions and tendinopathy, and the differential lists "hamstring origin tendinopathy" — the chronic, insidious counterpart to the acute avulsion above. Proximal (high) hamstring tendinopathy is an insertional tendinopathy of the conjoint origin at the ischial tuberosity, typically seen in distance runners, sprinters and hurdlers (and in middle-aged active adults).
Presentation. Gradual-onset deep buttock / ischial pain localised to the tuberosity — there is no acute pop and no massive ecchymosis (that distinguishes it from avulsion). The hallmark is pain that is worse on sitting (especially hard surfaces), with hamstring stretch, and with loaded hip flexion — accelerating, lunging, downhill or fast running. Strength is largely preserved and there is no palpable gap.
Why position matters (the compression model). At end-range hip flexion the proximal tendon is compressed against the ischial tuberosity, which acts as a bony pulley. Tendinopathy at this site is therefore a combined tensile-plus-compressive load problem, which is why deep hip flexion, sitting and aggressive static stretching all aggravate it — and why early management limits compression rather than stretching into it.
- Approach
- Tenderness over the ischial tuberosity; the Puranen-Orava test (standing, hip flexed near 90 degrees on a support with the knee extended), the bent-knee stretch and modified bent-knee stretch tests reproduce deep buttock pain
- Approach
- MRI shows origin tendinosis (thickening, increased signal) with peritendinous oedema and sometimes ischiogluteal bursitis, but no full-thickness avulsion gap; ultrasound can show the same
- Approach
- Reduce ischial compression first — modify sitting, avoid end-range hip-flexion loading and aggressive stretching early
- Approach
- Stage it: isometrics for pain, then heavy slow resistance / isotonic, then eccentric and finally energy-storage (running) loading; address gluteal and lumbopelvic strength and running mechanics
- Approach
- Extracorporeal shockwave therapy; image-guided peritendinous corticosteroid (short-term relief, used cautiously given proximity to the sciatic nerve); platelet-rich plasma has limited evidence; surgery (debridement) is rarely needed
Single-tendon semimembranosus tendinopathy and its specific footprint pathology are developed in the dedicated semimembranosus-tendinopathy topic.
Q: A runner has deep buttock pain that is worst when sitting, with no pop and normal strength. Avulsion or tendinopathy? A: Proximal hamstring tendinopathy. No acute pop, no ecchymosis, no gap, preserved strength, and sitting-aggravated ischial pain point to a compressive insertional tendinopathy — managed with load modification and staged loading, not surgical repair.
Hamstring Syndrome (Deep Gluteal Sciatic Entrapment)
The differential lists "deep gluteal / hamstring syndrome", and Viva 2 attributes chronic sitting pain to the stump scarring to the nerve — this is hamstring syndrome, first described by Puranen and Orava: extra-spinal entrapment of the sciatic nerve by tight tendinous/fibrous bands at the lateral ischial tuberosity, by the proximal hamstring origin, or by scar tethering after a healed avulsion or repair.
It sits within "deep gluteal syndrome" (extra-spinal sciatic entrapment in the subgluteal space) but is a distinct cause from its neighbours — keep them separate in the viva:
- Site / cause
- Sciatic nerve tethered by tendinous bands / scar at the ischial origin
- Routed to
- this topic
- Site / cause
- Nerve compressed at/under the piriformis
- Routed to
piriformis-anatomy
- Site / cause
- Quadratus femoris pinched between lesser trochanter and ischium
- Routed to
ischiofemoral-impingement
Presentation. Deep buttock pain radiating down the posterior thigh, worse on sitting and with stretching/sprinting, often with tenderness near the ischial tuberosity; it frequently coexists with proximal hamstring tendinopathy or follows a healed avulsion. Seated slump, Puranen-Orava and straight-leg-raise variants that tension the nerve reproduce the pain.
Investigation. MRI / MR neurography looks for perisciatic scarring and oedema at the ischium and excludes a space-occupying lesion; lumbar radiculopathy (L5/S1) must be excluded as the commonest mimic. An image-guided peri-neural injection of local anaesthetic is both diagnostic and therapeutic.
Management. First-line is conservative — neural mobilisation, hamstring/gluteal load management, activity modification and image-guided injection. Surgical decompression / neurolysis (release of the tethering bands and freeing of the sciatic nerve at the ischium) is reserved for refractory cases — the same neurolysis principle that is mandatory during chronic avulsion repair.
Management Algorithm
Treatment Strategy
- Single tendon tears.
- Low retraction (less than 2cm).
- Sedentary patients.
- Partial tears.
- 2 or 3 tendon avulsion.
- Retraction greater than 2cm.
- Active patients / Athletes.
- Sciatic nerve symptoms.
- Persistent pain/weakness.
- Requires Allograft usually.
- Neurolysis required.
RAWSurgical Indications
Hook:Repair Raw hamstrings.
Surgical Technique
Open Proximal Hamstring Repair
Position: Prone. Jack-knife position (flex hips to relax hamstrings). Incision: Transverse gluteal fold incision or Longitudinal posterior incision. Exposure:
- Identify Gluteus Maximus inferior border. Retract superiorly.
- FIND SCIATIC NERVE: First step. Identify and protect.
- Identify Ischial Tuberosity (debride to bleeding bone).
- Find tendon stump (often retracted distally).
Fixation:
- Suture anchors (titatium or PEEK) into ischial tuberosity (usually 2-4 anchors).
- Locking stitch (Krackow) in tendon.
- Reduce tendon to bone (Flex knee to 90 if needed).
- Tie sutures.
Care must be taken to avoid over-tensioning.
Complications
- Risk
- Unknown
- Note
- Stretch or direct injury. Most resolve.
- Risk
- low
- Note
- If rehab is too aggressive
- Risk
- Common
- Note
- Scar tissue at ischium (Ischial bursitis)
- Risk
- Common
- Note
- Gluteal fold is high tension/moisture area
Postoperative Care
Rehabilitation Protocol
- Phase 1 (0-6 weeks):
- Brace: Hip extension brace or Knee flexion brace? Usually Knee brace locked at 30-90 deg?
- Typically: Hip orthosis preventing flexion greater than 45, or simply crutches and cautious movement.
- Weight Bearing: Toe touch / PWB for 4-6 weeks.
- Avoid: Hip Flexion + Knee Extension (The stretch).
- Phase 2 (6-12 weeks):
- Wean crutches.
- Active hamstring curls (no resistance).
- stationary bike.
- Phase 3 (3-6 months):
- Strengthening. Nordic curls.
- Jogging.
- Return to sport at 6 months.
Surgical Complications Detail
- Sciatic Nerve Palsy: Can be neuropraxia from retraction or direct injury.
- Management: Observation for 3 months. EMG at 3 months if no recovery.
- Wound Dehiscence: Transverse gluteal crease incisions are high risk due to moisture and sitting pressure.
- Prevention: meticulous closure, avoiding prolonged sitting in early phase.
- Deep Infection: Rare but devastating. Requires debridement and often anchor removal.
- Rerupture: Occurs in 1-3% of repairs.
- Risk factors: Early return to sport, non-compliance with brace.
Outcomes and Prognosis
Acute Surgical Repair Outcomes
Return to Sport:
- Overall return rate: 80-90%
- Return to pre-injury level: 70-80%
- Mean time to return: 6 months
Functional Outcomes:
- Isokinetic strength testing shows 85-95% recovery vs contralateral
- Endurance activities recover well
- Sprinting and explosive movements may have persistent deficit
- Acute Repair
- 82-90%
- Chronic Repair
- 65-75%
- Conservative
- 50-60%
- Acute Repair
- 72%
- Chronic Repair
- 55%
- Conservative
- 30%
- Acute Repair
- 85-95%
- Chronic Repair
- 70-80%
- Conservative
- 60-70%
- Acute Repair
- High
- Chronic Repair
- Moderate
- Conservative
- Low-Moderate
Acute repair consistently outperforms delayed treatment.
Guidelines, Registries & Global Practice
Global Epidemiology
- Hamstring strains are among the most common injuries in running, football (soccer), rugby, Australian rules and track-and-field. True proximal origin avulsions are far rarer but functionally far more serious.
- Classic mechanisms recur worldwide: waterskiing (rising from a submerged start), gymnastics and dance (splits), bull riding, and slips into a sudden split.
- Two demographic peaks: adolescent athletes (ischial apophyseal avulsion, open growth plate) and middle-aged active adults (degenerate tendinous avulsion). Surgical series report a mean age in the mid-40s (Hillier-Smith 2022; Wood 2020).
Guidance Across Societies (side by side)
- Common ground
- MRI is the reference standard to count tendons and measure retraction
- Where emphasis differs
- Some European/US groups use ultrasound first-line where MRI access is limited
- Common ground
- Complete 2-3 tendon avulsion with retraction over 2cm in an active patient = repair
- Where emphasis differs
- Threshold for the borderline 2-tendon tear varies with surgeon/region
- Common ground
- Earlier repair is technically easier and lowers re-rupture and nerve dysfunction
- Where emphasis differs
- No society sets an absolute "too late" cut-off
- Common ground
- Most protocols brace the hip/knee early postoperatively
- Where emphasis differs
- Brace-free accelerated rehab increasingly reported
No single national orthopaedic society (AAOS, BOA, EFORT) publishes a dedicated proximal-hamstring-avulsion guideline; practice is driven by the systematic reviews and series cited above rather than formal level-1 guidance.
Registry and Resource Notes
- Unlike arthroplasty, proximal hamstring repair is not tracked in national joint/implant registries (NJR, AJRR, AOANJRR, SHAR), so the evidence base is series and reviews, not registry data.
- High-resource settings: prompt MRI, early specialist referral and acute repair with suture anchors are the norm.
- Limited-resource settings: delayed presentation is more common, raising the proportion of chronic, retracted tears that need mobilisation, neurolysis or allograft augmentation - and shifting the balance toward non-operative care for lower-demand patients.
Controversies and Areas of Uncertainty
A complete 3-tendon avulsion with retraction over 2cm in an active patient is a clear repair. The genuine uncertainty is the 2-tendon partial/complete tear with borderline retraction - here demand level, age and symptoms drive a shared decision rather than a fixed rule.
Acute repair is technically easier (Wood 2020) but chronic repairs still improve SHORE scores and strength (Sallay 2008). There is no validated cut-off beyond which repair becomes futile - retraction, fatty atrophy and surgeon experience matter more than a calendar number.
Systematic-review data favour bracing for lower re-rupture (Wyatt 2024), yet brace-free accelerated protocols report acceptable results and better compliance. Protocol heterogeneity means the optimal regimen is not settled.
Endoscopic/arthroscopic-assisted repair is emerging for partial and selected complete tears, but comparative evidence against open repair is limited and short-term; open repair remains the reference standard for retracted complete avulsions.
MCQ Practice Points
Q: What is the relationship of the Sciatic nerve to the Ischial Tuberosity? A: Lateral. Approximately 1.2cm lateral to the tuberosity.
Q: What is the main blood supply to the proximal hamstrings? A: Perforating branches of Profunda Femoris and Inferior Gluteal Artery.
Q: Which muscle originates most Anterolaterally on the tuberosity? A: Semimembranosus. The Conjoint tendon (Semi-T/Biceps) is Posteromedial.
Q: Which unit is most commonly avulsed from the ischium? A: The conjoint tendon (semitendinosus + biceps long head). In Koulouris and Connell's surgical series 14 of 16 ischial avulsions were conjoint, only 2 were isolated biceps. (Note: biceps femoris is the most commonly strained muscle in mid-substance injuries.)
Q: What is a key risk factor for chronic tendon degeneration? A: Fluoroquinolone antibiotics (rare) but more commonly Previous Injury and Age.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male water-skier felt a pop in his buttock when the boat accelerated. He has a massive bruise down his posterior thigh and cannot run. MRI shows a 3-tendon avulsion with 4cm retraction.”
“A 50-year-old runner presents 6 months after a 'pulled hamstring'. He has difficulty sitting and deep buttock pain. He has weakness. MRI shows a chronic rupture with 6cm retraction.”
“A 14-year-old sprinter feels a pop at the start of a race. X-ray shows a bony fragment displaced 1cm from the ischial tuberosity.”
Classification
- 1 Tendon: Conservative
- 2 Tendons: Gray zone (Retraction?)
- 3 tendon + greater than 2cm = Surgery
- Bony Avulsion: Conservative (Adolescent)
Diagnosis
- Waterskiing/Splits mechanism
- Bruising prone to knee
- Palpable gap
- MRI Gold Standard
Management
- Acute (less than 4 wk): Primary Repair
- Chronic (greater than 4 wk): Allograft?
- Neurolysis of Sciatic Nerve
- Rehab: No tension (flexion) for 6 weeks
Anatomy
- Ischial Tuberosity Origin
- Sciatic Nerve 1.2cm Lateral
- Conjoint Tendon = Medial
- Semimembranosus = Lateral
Evidence Base
Avulsion of the Proximal Hamstring Origin (classification source)
- Complete avulsion is the dominant pattern (87.5%)
- Mean retraction 7cm (range 0-20cm)
- Delay makes repair harder and increases sciatic involvement and bracing need
- Source of the Wood classification used worldwide
Hamstring Injuries Among Water Skiers (landmark mechanism series)
- Defined the classic waterski mechanism
- Complete disruptions did worst non-operatively
- Persistent deficit drove delayed surgery in some
- Established the injury as functionally disabling
Operative vs Non-operative: Meta-analysis
- Repair beats non-operative on satisfaction and strength
- Acute repair superior to chronic
- Complication rate around 23% - counsel patients
- Non-operative comparison group was small (low certainty)
Outcomes of Surgical Management: Systematic Review and Meta-analysis
- Return to sport 84.5% at ~6.5 months
- Re-rupture only 1.2% overall
- Sciatic nerve dysfunction 3.5%, lower if acute
- Acute repair = quicker return, fewer re-ruptures
MRI vs Ultrasound for Avulsion Detection
- MRI sensitivity 16/16 for ischial avulsion
- Ultrasound less reliable (7/12)
- Imaging discriminates avulsion from strain
- Identifies who needs surgery vs conservative care
Timing of Repair (SHORE outcomes)
- Repair improves SHORE regardless of timing
- Earlier surgery = better recovery and more return to baseline
- Acute repair is shorter and technically easier
- Fewer neurological symptoms with acute repair
Bracing vs No Bracing After Repair
- Re-rupture much lower with bracing
- Higher satisfaction and return to sport when braced
- Evidence base is heterogeneous (level 4)
- Brace protocols remain the conservative default
Chronic and Acute Repair: Functional Recovery
- Strength keeps improving past 12 months
- Both acute and chronic repairs satisfied patients
- Suture-anchor fixation to ischium
- Chronic tears are still worth repairing