Platelet-Rich Plasma (PRP) & Orthobiologics
- "PRP" is not one product — platelet dose, leukocyte content, activation method and spin protocol all vary, so two PRP injections can be biologically very different. Always specify the preparation and cite the leukocyte content when quoting a trial. This is the single most examined caveat.
- Use leukocyte-POOR PRP intra-articularly (e.g. knee OA) — leukocytes drive an inflammatory flare in the joint; level-1 data favour LP over LR for knee OA. Leukocyte-rich is the one sometimes argued for tendinopathy.
- PRP does NOT regrow cartilage or replace arthroplasty — it is a symptomatic option for mild-to-moderate OA. Claiming disease modification or cartilage regeneration loses marks.
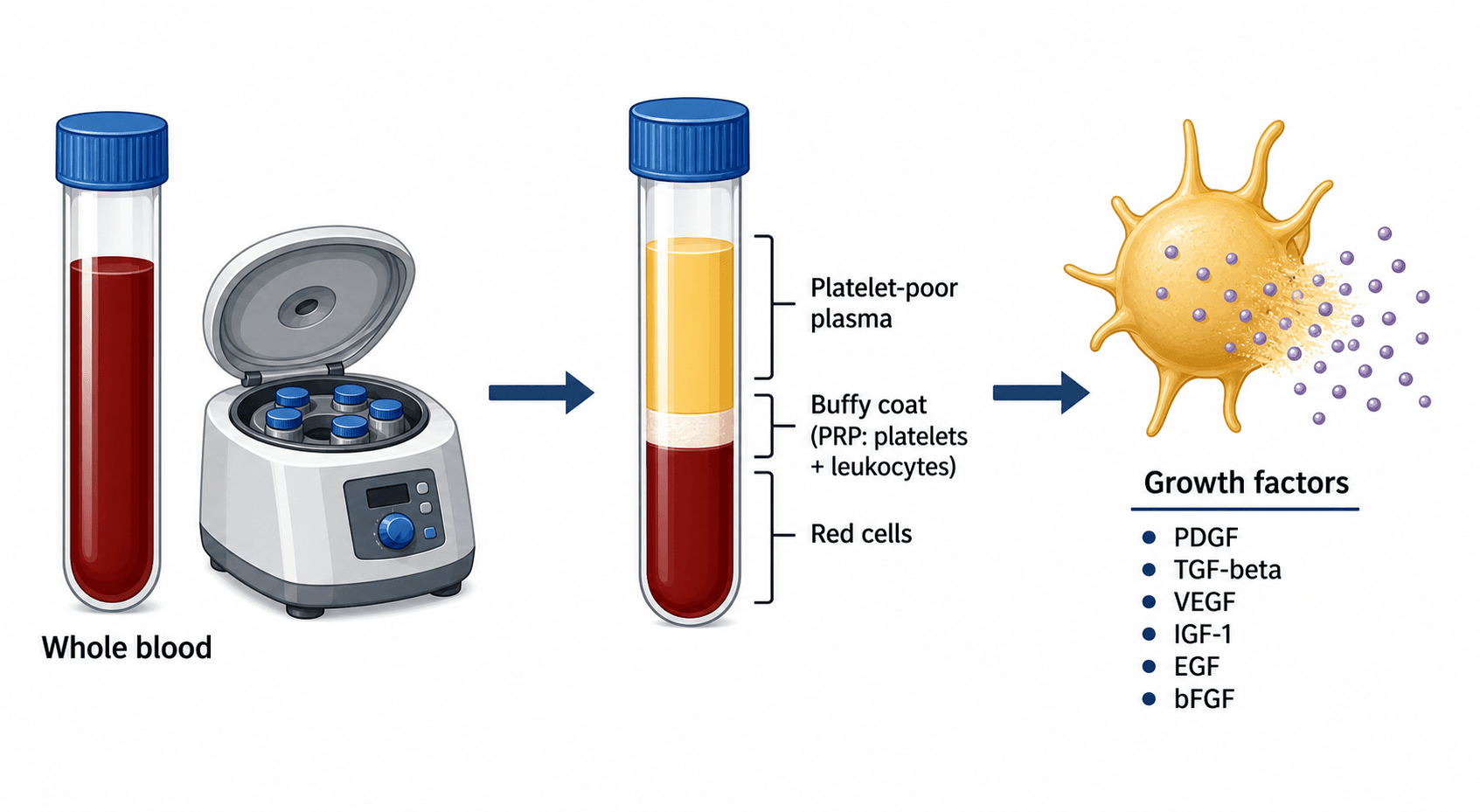
- Name the growth factors and their source — PDGF, TGF-β, VEGF, IGF-1, EGF, bFGF, released from platelet alpha-granules on activation (not dense granules).
- PRP is the best-studied orthobiologic; MSCs are largely investigational/regulated — don't overstate stem-cell therapy.
- The strong evidence is knee OA (PRP beats HA); tendinopathy evidence is mixed — don't quote the knee-OA strength for every indication.
Overview & Introduction
Orthobiologics are biologically active preparations used to augment musculoskeletal healing, and platelet-rich plasma (PRP) is the most widely used and best-studied of them. The appeal is simple: take a small volume of the patient's own blood, concentrate the platelets, and deliver their growth-factor payload to a degenerate or injured tissue to nudge it towards repair. Because it is autologous and office-based, PRP has spread rapidly into sports medicine and arthroplasty practice - which is exactly why examiners want a candidate who can separate the genuine level-1 signal (knee osteoarthritis) from the hype and the heterogeneity.
- Rapid clinical uptake ahead of robust evidence makes it a favourite viva theme - the examiner is testing judgement, not enthusiasm.
- The science is examinable: the growth factors, their platelet alpha-granule source, and the leukocyte axis are concrete facts.
- The evidence is uneven: strong for knee OA (PRP beats HA), mixed for tendinopathy, weak/low-level for most other uses.
- Standardisation is the recurring criticism - and the reason PAW/Mishra reporting systems exist.
Concepts: what PRP is & what it delivers
Platelet-rich plasma (PRP) is an autologous preparation in which the patient's own blood is centrifuged to concentrate platelets (commonly several-fold above the whole-blood baseline) into a small plasma volume. Platelets store growth factors in their alpha-granules; on activation they release PDGF, TGF-β, VEGF, IGF-1, EGF and bFGF, among others. The rationale is that delivering a bolus of these factors to an injured or degenerate tissue promotes cell proliferation, matrix synthesis, angiogenesis and modulation of inflammation — augmenting the local healing environment.
- Principal actions
- Chemotaxis and proliferation of mesenchymal cells; angiogenesis
- Principal actions
- Matrix synthesis (collagen); chondrocyte/osteoblast effects; modulates inflammation
- Principal actions
- Angiogenesis (new blood vessel formation)
- Principal actions
- Cell proliferation/survival; matrix production
- Principal actions
- Proliferation, angiogenesis and tissue remodelling
Preparation

PRP is made at the point of care: anticoagulated whole blood is centrifuged so it separates by density into plasma (top), a thin buffy coat of platelets and leukocytes (middle), and red cells (bottom). A single spin ('soft') concentrates platelets in plasma while keeping some red/white cells; a double spin ('hard') achieves higher platelet concentration and lets the operator include or exclude the leukocyte layer to make leukocyte-rich or leukocyte-poor PRP. The product may be used as a liquid (often activated with calcium chloride/thrombin to trigger granule release) or as a fibrin matrix (PRF).
Classification — leukocyte-poor vs leukocyte-rich
Low white-cell content ('pure' PRP). Generally preferred for intra-articular use (e.g. knee OA) because leukocytes (and their catabolic enzymes/cytokines) can provoke a more inflammatory flare in a joint. Level-1 data favour LP-PRP over LR-PRP for knee OA.
Higher white-cell content; more pro-inflammatory. Has been advocated for some tendinopathies (where a controlled inflammatory/anabolic stimulus may help), though comparative evidence is limited.
Because products vary so much, classification systems standardise reporting: PAW (Platelets, Activation, White cells — DeLong), Mishra, and PLRA (Platelet, Leukocyte, Red cell, Activation). For the exam, the headline distinction is LP vs LR, and you should always state the leukocyte content when describing a study's PRP.
Alongside the leukocyte axis, the platelet dose - the absolute number of platelets delivered (the 'P' of PAW) - is increasingly recognised as a key determinant of efficacy. A clinically effective PRP generally needs a meaningful concentration above whole-blood baseline (a commonly-cited target is around a five-fold concentration, or an absolute dose on the order of ~10 billion platelets for knee OA), with an apparent dose-response - too low a dose under-treats. Importantly the relationship may be bell-shaped: very high platelet concentrations can paradoxically be inhibitory in laboratory studies. This is why two leukocyte-poor PRPs from different systems can still behave differently, and why reporting the platelet dose (not just LP vs LR) matters when comparing trials.
The wider orthobiologics toolbox
- What it is
- Autologous concentrated platelets + growth factors
- Typical use / status
- Knee OA (LP-PRP), tendinopathy; best-studied
- What it is
- Concentrated marrow (cells + growth factors)
- Typical use / status
- Cartilage/bone defects, OA; variable evidence
- What it is
- Culture-expanded or concentrated stromal cells
- Typical use / status
- Investigational; regulatory constraints
- What it is
- Serum enriched in anti-inflammatory IL-1Ra
- Typical use / status
- OA/radiculopathy; limited evidence
- What it is
- Viscosupplement (not strictly a 'biologic')
- Typical use / status
- Knee OA — the usual comparator for PRP
- What it is
- Recombinant osteoinductive growth factors
- Typical use / status
- Spinal fusion / selected nonunion (see Bone Signalling)
Across all orthobiologics the limiting issue is lack of standardisation and regulation: dose, cell/platelet content, processing and activation vary between systems and studies, outcomes are heterogeneous, and many indications rest on low-level evidence. The mature position is to use the best-supported indications (e.g. LP-PRP for knee OA), specify the preparation, counsel honestly about uncertainty and cost, and avoid overselling unproven uses.
Mnemonics & Memory Aids
- PRP = autologous concentrated platelets releasing PDGF, TGF-β, VEGF, IGF-1, EGF, bFGF from alpha-granules.
- Leukocyte-poor vs leukocyte-rich is the key axis — LP intra-articular (less inflammatory), LR sometimes for tendinopathy.
- Knee OA: level-1 evidence PRP beats HA at 6–12 months; LP-PRP over LR-PRP; no extra adverse events.
- Tendinopathy (e.g. lateral epicondylitis): mixed evidence, used when conservative care fails.
- Reporting systems: PAW (DeLong), Mishra, PLRA.
- The central caveat: lack of standardisation — always specify the preparation and counsel honestly.
PRP-VIDEGrowth factors + the caveat
Hook:PRP-VIDE: the platelet factors (PDGF, TGF-β, VEGF, IGF-1, EGF, bFGF) and the standardisation caveat.
LP-JOINTThe best-supported use
Hook:LP-JOINT: leukocyte-poor PRP into the joint is the best-supported PRP use.
Clinical evidence
Two level-1 meta-analyses anchor the knee-OA story: intra-articular PRP outperforms hyaluronic acid for pain and function at 6 and 12 months without more adverse events, and leukocyte-poor PRP does better than leukocyte-rich intra-articularly. In Belk et al. (18 level-1 RCTs) the mean WOMAC improvement was 44.7%PRP versus 12.6%HA.
This is where the evidence is best. Level-1 meta-analyses show intra-articular PRP gives better pain relief and function than hyaluronic acid at 6 and 12 months, with no increase in adverse events, and that leukocyte-poor PRP is associated with better outcomes than leukocyte-rich. PRP is used as a non-operative option, particularly in mild-to-moderate OA, for symptomatic relief and to potentially delay surgery (it does not regrow cartilage or replace arthroplasty for end-stage disease).
PRP is autologous and very safe, but examiners expect the practical caveats. Relative/absolute contraindications include active infection (local or systemic), active malignancy (especially at the injection site), critical thrombocytopenia or platelet-function disorders, and significant anaemia; anticoagulation is a relative contraindication. The key drug interaction: NSAIDs and aspirin inhibit platelet COX and granule release, so they are usually withheld around the procedure (commonly about a week before and one-to-several weeks after), and a recent intra-articular corticosteroid may blunt the anabolic response, so the two are spaced apart. The main adverse effect is a self-limiting post-injection pain/inflammatory flare (more common with leukocyte-rich PRP); serious complications such as infection are rare. Counsel about the transient flare, the need to pause anti-inflammatories, and the out-of-pocket cost.
Evidence Base
Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- Meta-analysis of 18 level-1 RCTs (811 PRP vs 797 HA patients, mean follow-up 11.1 months): mean WOMAC total improvement was significantly higher with PRP (44.7%) than HA (12.6%).
- 6 of 11 VAS-based trials and 3 of 6 IKDC-based trials showed significantly better pain/function with PRP at latest follow-up.
- Leukocyte-POOR PRP was associated with significantly better subjective IKDC scores than leukocyte-rich PRP.
Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: a meta-analysis
- Meta-analysis of 20 RCTs: intra-articular PRP reduced pain (WOMAC pain/VAS) more effectively than HA at 6 and 12 months.
- PRP gave better functional recovery (WOMAC function) at 1, 3, 6 and 12 months, and better IKDC at 3 and 6 months, than HA.
- PRP did not increase the risk of adverse events compared with HA.
Platelet-rich plasma: the PAW classification system
- Protocols for PRP preparation vary widely and are often poorly documented, making results hard to compare or replicate.
- Proposes the PAW classification on 3 components: the absolute number of Platelets, the manner of Activation, and the presence/absence of White cells.
- A standard reporting scheme is needed to compare protocols and group studies for meta-analysis.
The knee-OA efficacy statements (PRP superior to HA; leukocyte-poor better than leukocyte-rich) come from two level-1 meta-analyses - Belk et al. 2021 (DOI) and Tang et al. 2020 (DOI); and the PAW reporting framework from DeLong, Russell & Mazzocca 2012 (DOI). The growth-factor list and preparation details are standard, well-established descriptions; the lack of standardisation is a consistently reported limitation that the PAW system was created to address.