Pseudoachondroplasia
Despite the short limbs, PSACH is COMP (not FGFR3), normal at birth (not evident at birth), has a normal face and intelligence, and involves the spine (platyspondyly). Reflexively calling any short-limbed child 'achondroplasia' is the classic error.
Atlantoaxial instability from odontoid hypoplasia + ligamentous laxity can cause cord injury on intubation or positioning. Assess the cervical spine (flexion-extension films, MRI if indicated) before any general anaesthetic - missing this is a real and exam catastrophe.
Overview & Significance
Pseudoachondroplasia (PSACH) is one of the classic "compare and contrast" dysplasias of fellowship exams, paired against achondroplasia. The name is a trap and a teaching point in one: the child has the short-limb, disproportionate habitus that superficially resembles achondroplasia ("pseudo"), but the underlying biology, the timing, the face, and the spine are all different.
It matters clinically because the systemic features are mild — normal intelligence, normal facial appearance, no foramen-magnum or respiratory compromise — so the patient lives a long life dominated by mechanical orthopaedic problems: malaligned, painful, early-arthritic lower limbs, and an at-risk cervical spine. The orthopaedic surgeon, not the geneticist, carries most of the lifelong care.
Pathophysiology, Genetics & Mechanism
PSACH is caused by autosomal dominant mutations in the gene for cartilage oligomeric matrix protein (COMP) on chromosome 19 (19p13.1). COMP is a large pentameric extracellular-matrix glycoprotein of cartilage, tendon and ligament. Most mutations cluster in the calcium-binding (type-3 thrombospondin repeat) domains (with some in the C-terminal globular domain) and compromise protein folding.
The misfolded COMP cannot be secreted and is instead retained inside the chondrocyte endoplasmic reticulum, dragging its binding partners (type IX collagen, matrilin-3) in with it. This makes PSACH — together with the COMP form of multiple epiphyseal dysplasia (MED), its allelic partner — an ER storage disorder: the retained protein forms characteristic lamellar inclusion bodies in the rough ER, triggers ER stress with oxidative and inflammatory injury, and drives chondrocyte death. The net effect is failure of orderly endochondral growth and short stature.
PSACH and the COMP form of MED are a spectrum: identical gene, PSACH the more severe end (more short stature, spine involvement, ligamentous laxity) and MED the milder (mainly epiphyses, spine spared). Inheritance is autosomal dominant with ~50% transmission to offspring; new (de novo) mutations and recurrence through parental gonadal mosaicism both occur, which is important for genetic counselling.
Clinical presentation
- Normal at birth — undetectable clinically and radiologically; birth length is normal
- Short-limb, often rhizomelic, disproportionate dwarfism emerging in early childhood (~2 years), as the child starts walking
- Waddling (Trendelenburg) gait, marked generalised ligamentous laxity (wrists, hands, knees), exaggerated lumbar lordosis, lower-limb deformity
- Markedly reduced adult height (well below achondroplasia in many cases)
- NORMAL face and skull — no frontal bossing, no midface hypoplasia
- NORMAL intelligence
- No foramen-magnum stenosis and no characteristic respiratory compromise (unlike achondroplasia)
- These three are the discriminators an examiner is listening for.
Ligamentous laxity is generalised and often striking at the hands, wrists and knees — but the elbows characteristically show restricted extension rather than hyperlaxity. A child with diffuse joint laxity, a waddling gait and limited elbow extension is a recognisable PSACH picture.
Unlike achondroplasia (evident at birth with characteristic facies), PSACH has no specific clinical or radiological findings at birth; the features develop slowly through childhood. Diagnosis is made on the evolving short stature, gait and skeletal changes, supported by radiographs and confirmed by COMP genetic testing. Serial assessment, not a single neonatal film, makes the diagnosis.
Investigations & Radiographic Features
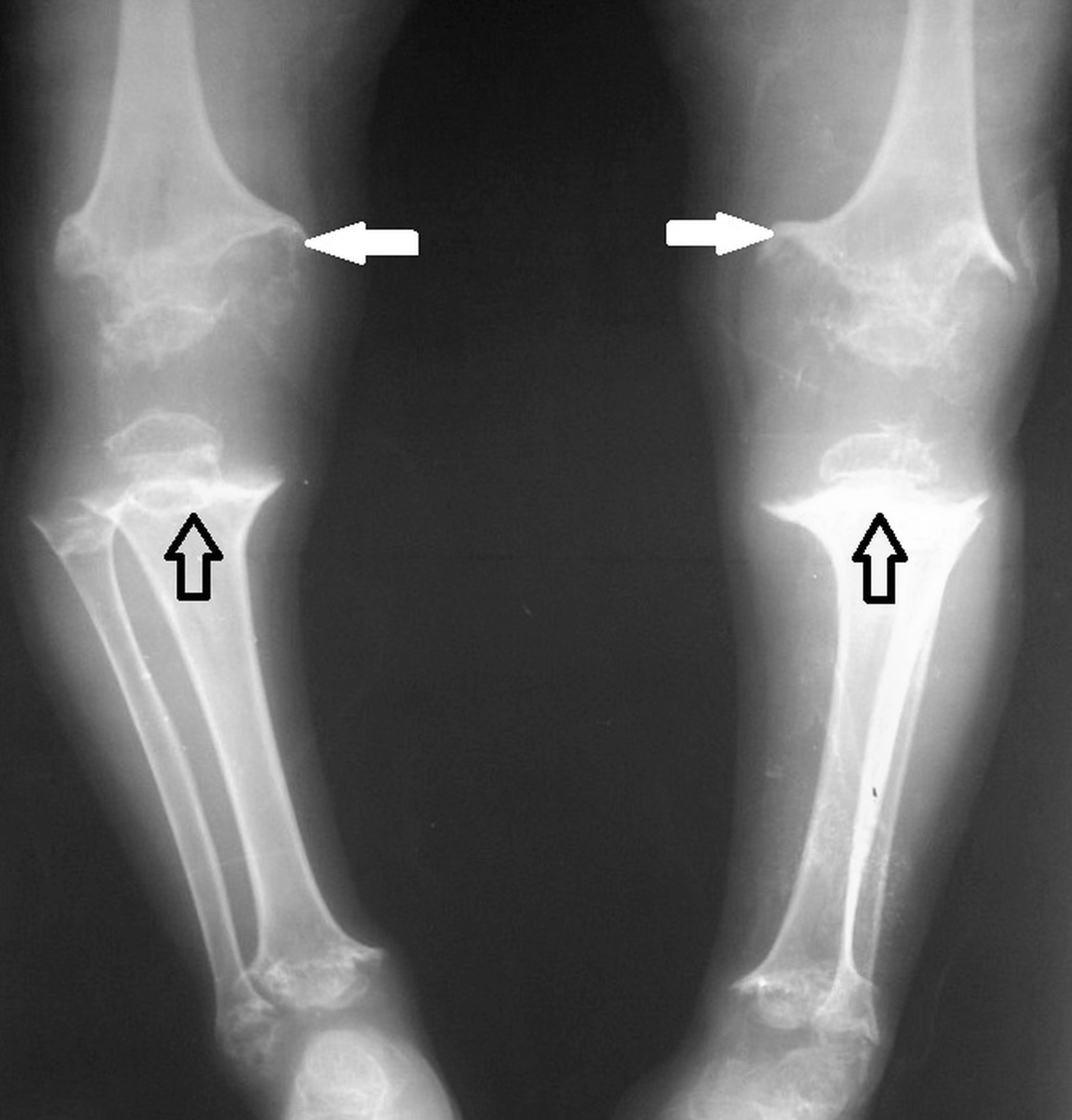
The radiographic signature is an epiphyseal AND metaphyseal dysplasia with spine involvement — the combination, in a child who was normal at birth, is what nails PSACH.
- Finding
- Small, irregular, fragmented, late-ossifying (esp. capital femoral epiphyses, knees)
- Why it matters
- Drives early osteoarthritis and can mimic bilateral Perthes/MED
- Finding
- Irregular, flared, widened
- Why it matters
- Distinguishes PSACH from MED (which spares metaphyses)
- Finding
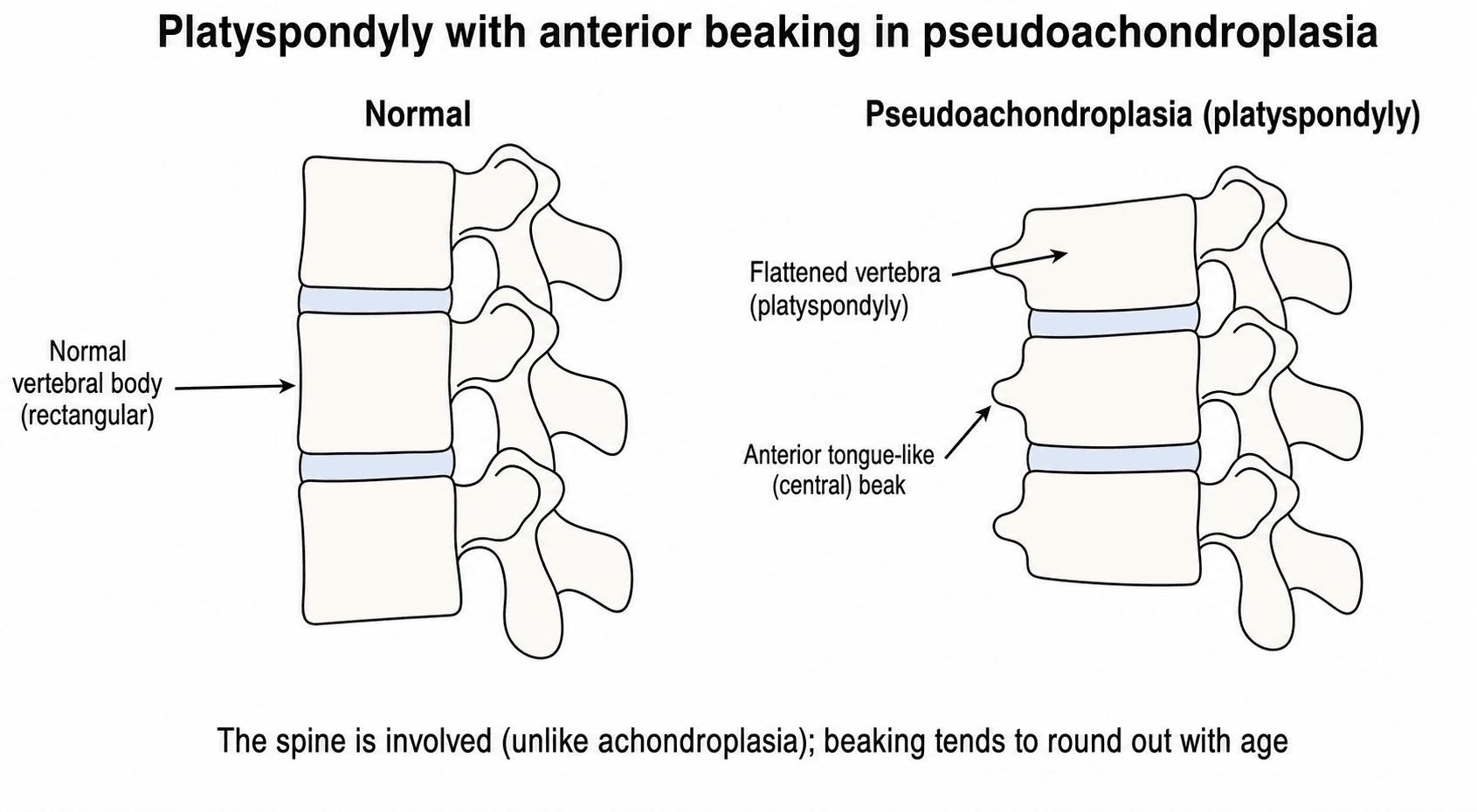
- Platyspondyly (flattened vertebrae) with anterior tongue-like beaking; tends to round out with age
- Why it matters
- Confirms spine involvement — the spine is NOT spared (unlike achondroplasia)
- Finding
- Odontoid hypoplasia + ligamentous laxity
- Why it matters
- Atlantoaxial instability — screen before anaesthesia
- Finding
- Short tubular bones, brachydactyly, small irregular carpals
- Why it matters
- Part of the short-limb, short-digit habitus
- Finding
- Small irregular capital femoral epiphyses, irregular acetabula, coxa vara
- Why it matters
- Sets up hip malalignment and early hip OA


The location of vertebral beaking is a favourite radiology discriminator. PSACH shows anterior tongue-like (central) beaking with platyspondyly that tends to normalise in adulthood. Compare: Morquio (MPS IV) classically shows central beaking with universal platyspondyly and odontoid hypoplasia; Hurler (MPS I) and achondroplasia show antero-inferior beaking, often with a thoracolumbar gibbus. Don't over-commit to a single beak in the viva — describe what you see and name the differentials.
Differential diagnosis
The whole point of PSACH in exams is telling it apart from its neighbours. The discriminators are gene, timing of presentation, face, spine, and which part of the bone is affected.
- Pseudoachondroplasia
- COMP (AD)
- Achondroplasia
- FGFR3 (AD)
- MED
- COMP / COL9 / MATN3 (AD)
- SED congenita
- COL2A1 (AD)
- Pseudoachondroplasia
- Normal — presents ~2y
- Achondroplasia
- Evident at birth
- MED
- Normal — presents in childhood
- SED congenita
- Evident at birth
- Pseudoachondroplasia
- Normal
- Achondroplasia
- Frontal bossing, midface hypoplasia
- MED
- Normal
- SED congenita
- Normal (but flat face); ocular/hearing issues
- Pseudoachondroplasia
- Involved — platyspondyly
- Achondroplasia
- Length preserved (but stenosis)
- MED
- Spared / minimal
- SED congenita
- Platyspondyly (involved)
- Pseudoachondroplasia
- Epiphyseal + metaphyseal
- Achondroplasia
- Metaphyseal (rhizomelic)
- MED
- Epiphyseal only
- SED congenita
- Spondylo + epiphyseal (no metaphyseal)
- PSACH vs achondroplasia: different gene (COMP vs FGFR3), normal vs abnormal face, normal-at-birth vs evident-at-birth, and the spine is involved in PSACH but length-preserved in achondroplasia. Intelligence is normal in both.
- PSACH vs MED: same gene possible (allelic COMPopathies), but PSACH is more severe, involves the metaphyses and the spine, and has marked ligamentous laxity; MED is milder, epiphyses only, spine essentially spared.
Short stature with platyspondyly and an unstable odontoid is not unique to the dysplasias - the mucopolysaccharidoses sit in the same differential, and the overlap matters because they share the atlantoaxial instability that drives the anaesthetic risk. Morquio (MPS IVA, keratan-sulfate accumulation) has platyspondyly with odontoid hypoplasia and atlantoaxial instability like PSACH, but is given away by corneal clouding, hearing loss, valvular/aortic disease, raised urinary glycosaminoglycans and a progressive course - with normal intelligence. Hurler (MPS IH) adds coarse facies, hepatosplenomegaly, corneal clouding, intellectual disability and a thoracolumbar gibbus. PSACH, by contrast, has a normal face and cornea, no organomegaly, normal urinary GAGs and normal intelligence, and is confirmed on COMP testing. If the face is coarse, the cornea is hazy or the urine GAGs are raised, think storage disease - not a COMPopathy.
Management & Orthopaedic Problems
There is no disease-modifying drug; management is multidisciplinary, largely orthopaedic and supportive, with genetic counselling. The aims are to preserve alignment and joint function, manage early arthritis, and protect the cervical spine.
- 1Protect the cervical spine firstBefore any general anaesthetic or major surgery, assess the C-spine for atlantoaxial instability (clinical exam + flexion-extension radiographs, MRI if indicated). Odontoid hypoplasia and ligamentous laxity can cause cord injury on intubation or positioning.
- 2Correct lower-limb malalignmentGenu varum, valgum or windswept deformity is the rule. In the growing child use guided growth (hemiepiphysiodesis / tension-band plating); after maturity use corrective osteotomy. Deformity is often multiplanar and can recur — plan for surveillance.
- 3Manage early osteoarthritisHips and knees develop premature OA from the dysplastic incongruent joints. Activity and weight management buy time; many patients ultimately need hip or knee arthroplasty — technically demanding given small bones, deformity and laxity.
- 4Watch the spine and counsel the familyMonitor for scoliosis and excessive lumbar lordosis; treat as indicated. Provide genetic counselling (AD, ~50% transmission) and a multidisciplinary plan.
Genu varum, valgum or windswept deformity is the rule and is often multiplanar and recurrent. In the growing child, guided growth (hemiepiphysiodesis / tension-band plating) is the workhorse; after maturity, corrective osteotomy realigns the limb. Plan for surveillance and repeat correction through growth, and consider deformity in both planes on long-leg alignment films.
As with several dysplasias, cervical (atlantoaxial) instability — from odontoid hypoplasia and ligamentous laxity — can occur and risks cord injury. Assess the cervical spine (clinical examination plus flexion-extension radiographs, and MRI as indicated) before any general anaesthetic or significant surgery, and during growth. Stabilise if symptomatic or demonstrably unstable. Missing this is a classic exam (and real-world) catastrophe.
Small, irregular, fragmented capital femoral epiphyses bilaterally can be mistaken for bilateral Legg-Calvé-Perthes disease or bilateral avascular necrosis. PSACH (and MED) produce symmetrical epiphyseal change with the wider dysplastic context (metaphyses, spine, short stature, family history) — bilateral symmetrical "Perthes" should prompt a hunt for an underlying epiphyseal dysplasia.
Alignment and worn joints aside, families often ask about the short stature itself. Limb lengthening (distraction osteogenesis) is described and can add height while correcting deformity, but it is more controversial and less predictable in PSACH than in achondroplasia: the epiphyses and joints are themselves dysplastic and ligamentously lax, so lengthening loads already-abnormal joints and may accelerate the early osteoarthritis and instability that dominate the condition - hence careful patient selection and specialist-centre care, with priority given to alignment and joint preservation over height. Growth hormone gives little benefit here: the problem is an intrinsic cartilage-matrix / ER-storage defect, not growth-hormone deficiency, so the responsiveness seen in some other short-stature conditions does not apply.
Complications & prognosis
The prognosis for life and intellect is normal; the prognosis for joints is not. Expect:
- Early, often disabling osteoarthritis of the weight-bearing joints (hips and knees), frequently from the third decade — the dominant long-term problem.
- Recurrent / multiplanar lower-limb deformity requiring staged correction through growth.
- Cervical instability with its neurological risk, and spinal deformity (scoliosis, lordosis).
- Reduced final height and the functional/psychosocial issues of disproportionate short stature.
AVN-mimicking epiphyseal change, joint incongruity and laxity together explain why these joints wear out early. The orthopaedic relationship is lifelong — from guided growth in childhood to arthroplasty in adulthood.
Mnemonics & Memory Aids
COMPPseudoachondroplasia core
Hook:Pseudoachondroplasia is a COMP problem: COMP gene, Cervical care, OA, Metaphyseal/epiphyseal dysplasia, Presents in childhood.
NOT-ASNot achondroplasia
Hook:PSACH is 'NOT-AS' achondroplasia: Normal at birth/face/intelligence, COMP not FGFR3, Spine involved.
PSACHRadiographic signature
Hook:The radiographs spell PSACH: Platyspondyly, Small epiphyses, Abnormal metaphyses, Cervical odontoid, Hands short.
Exam & revision
Everything below condenses PSACH for revision and viva practice — the high-yield points, memory hooks, worked vivas, and a one-screen cheat sheet.
- COMP, autosomal dominant, chromosome 19 — a "COMPopathy" / ER storage disorder, allelic with the COMP form of MED.
- Normal at birth; presents ~2 years — with short-limb dwarfism, waddling gait and ligamentous laxity.
- Normal face, skull and intelligence — the cleanest discriminators from achondroplasia.
- Epiphyseal + metaphyseal dysplasia AND platyspondyly — the spine IS involved (unlike achondroplasia).
- C-spine instability (odontoid hypoplasia/laxity) — screen before anaesthesia.
- Orthopaedic burden: lower-limb malalignment (guided growth/osteotomy) and early OA (→ arthroplasty).
The numbers worth carrying: inheritance is autosomal dominant with around 50% transmission to offspring, the gene sits on chr 19COMP, and presentation is typically around 2 yrage of age — with a normal face and intelligence throughout.
Viva practice
Practise clinical reasoning and management decisions out loud
“A 3-year-old presents with short-limbed short stature and a waddling gait; the parents say the child looked normal at birth. The face is normal and development is normal. What is the likely diagnosis, what is the gene, and how do you distinguish it from achondroplasia?”
“What orthopaedic problems would you anticipate in pseudoachondroplasia, and what must you check before this child has a general anaesthetic?”
Identity
- Autosomal dominant COMP mutation (chromosome 19); a 'COMPopathy' (allelic with the COMP form of MED)
- ER storage disorder: misfolded COMP retained, causing chondrocyte stress/death
- Short-limb disproportionate dwarfism
Clinical
- NORMAL at birth; presents ~2y with short stature + waddling gait + ligamentous laxity
- NORMAL face/skull and NORMAL intelligence (key vs achondroplasia)
- Laxity generalised but elbow extension often restricted
Radiographs
- Epiphyseal dysplasia (small, irregular, fragmented epiphyses)
- Metaphyseal dysplasia (irregular/flared) - distinguishes from MED
- Platyspondyly +/- anterior beaking; short tubular bones; odontoid hypoplasia
Orthopaedic care
- Lower-limb malalignment: guided growth/osteotomy; early OA leads to arthroplasty
- Scoliosis/lordosis; ligamentous laxity
- SCREEN cervical spine (atlantoaxial instability) before anaesthesia
Evidence
Mutations in exon 17B of cartilage oligomeric matrix protein (COMP) cause pseudoachondroplasia
- The landmark study identifying COMP mutations as the cause of pseudoachondroplasia, mapping the gene to chromosome 19p12-13.1.
- All mutations identified in 8 familial/isolated cases involved exon 17B, mostly deleting or changing a conserved aspartic acid in the calcium-binding type-3 repeats.
- Established the molecular basis that defines the diagnosis and underpins COMP genetic testing.
Cartilage oligomeric matrix protein: COMPopathies and beyond
- Pseudoachondroplasia and multiple epiphyseal dysplasia are 'COMPopathies' caused by autosomal dominant COMP mutations, the majority in the calcium-binding domains, which compromise protein folding.
- They are ER storage disorders: retention of misfolded COMP in the chondrocyte endoplasmic reticulum stimulates cellular stress, oxidative and inflammatory processes and chondrocyte death, leading to loss of long-bone growth.
- COMP also functions in collagen secretion/fibrillogenesis and is being explored as a biomarker in osteoarthritis, fibrosis and other diseases.
Bone dysplasia with short limb
- In contrast to achondroplasia, where features are evident at birth, pseudoachondroplasia has no specific clinical or radiological findings at birth.
- Clinical and radiological findings develop slowly through childhood, so serial assessment is needed.
- Each short-limb dysplasia (achondroplasia, pseudoachondroplasia, metaphyseal chondrodysplasia, mesomelic dysplasia) has characteristic clinical and radiographic features that allow diagnosis on careful examination.
Mental health conditions, physical functioning, and health-related quality of life in adults with a skeletal dysplasia: a cross-sectional multinational study
- Across 142 adults with skeletal dysplasia (including pseudoachondroplasia, MED and SED congenita), 99% reported pain and 36% a prior psychiatric diagnosis; clinically significant depression in 23% and anxiety in 13%.
- Adults with 'other skeletal dysplasias' (the group including PSACH) reported more pain, more psychiatric symptoms, greater difficulty with daily activities and lower quality of life than those with achondroplasia.
- The most affected functional domains were activities, reach and walking - reflecting the lifelong joint/limb burden.
The founding genetics come from Hecht et al. (Nature Genetics, DOI), the COMPopathy/ER-storage mechanism from Posey et al. (DOI), the 'normal at birth, develops through childhood' clinical course from Kobayashi et al. (Clin Calcium 2008;18(12):1786-91), and the lifelong pain/quality-of-life burden from Fagereng et al. (DOI). The radiographic features, the achondroplasia/MED/SED comparison and the cervical-instability caveat are standard, well-established dysplasia knowledge. (See also our Skeletal Dysplasias, Multiple Epiphyseal Dysplasia and Achondroplasia material.)