Primary Bacterial Muscle Infection (Tropical Pyomyositis)
- Pyomyositis is a PRIMARY bacterial infection of SKELETAL MUSCLE with INTRAMUSCULAR ABSCESS formation; it is 'primary' because it arises within the muscle (often haematogenously) rather than spreading from adjacent bone/soft tissue, and although classically TROPICAL and PAEDIATRIC, it is increasingly recognised in TEMPERATE climates and in adults, particularly with immunocompromise (diabetes, HIV), and frequently follows minor TRAUMA to the muscle.
- The commonest causative organism is STAPHYLOCOCCUS AUREUS (including METHICILLIN-RESISTANT S. aureus, MRSA), so empirical antibiotic choice must cover it; large muscle groups - the quadriceps/thigh, gluteal muscles and iliopsoas - are typically affected, and lower-limb involvement predominates.
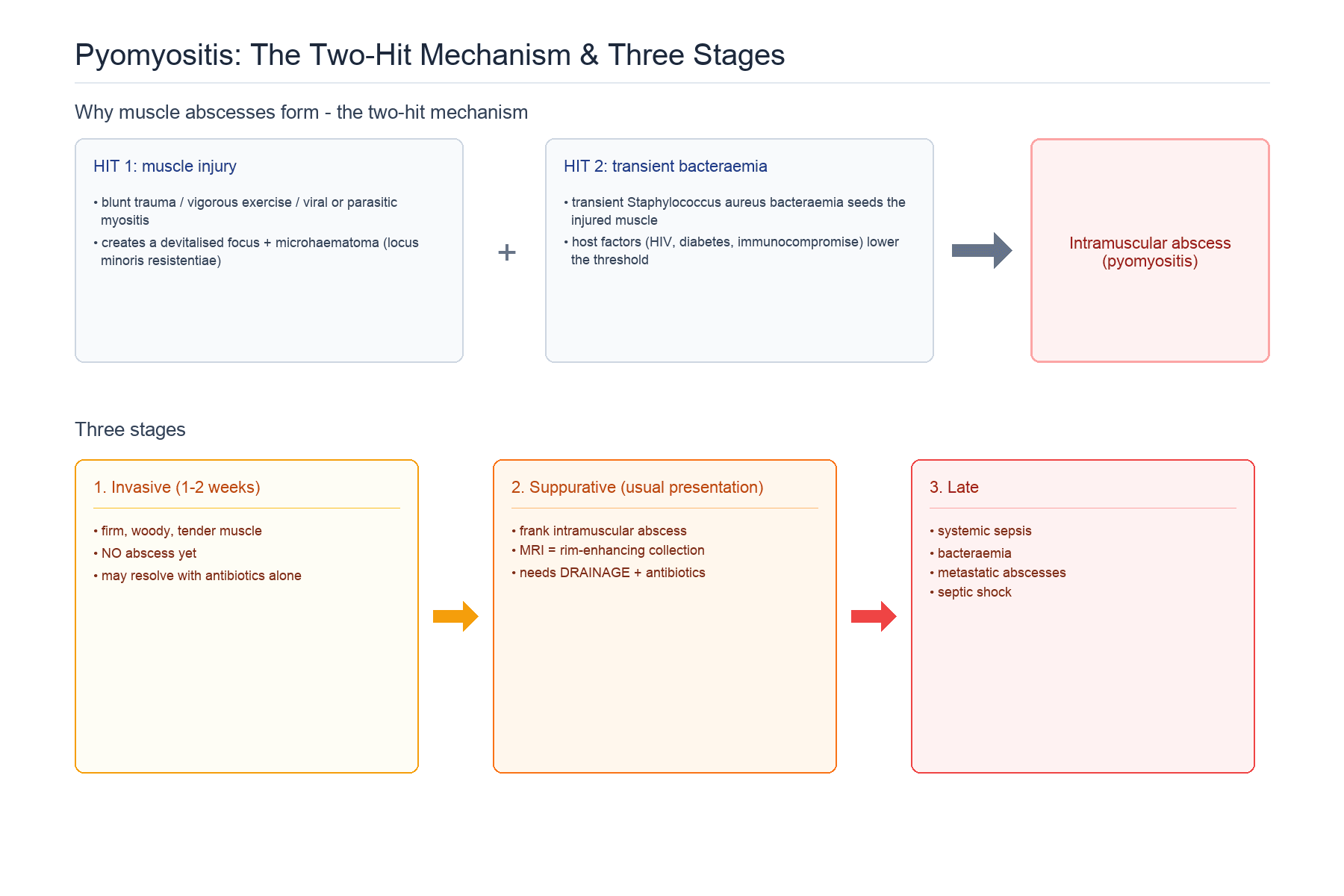
- It evolves through THREE STAGES: STAGE 1 (invasive) - diffuse muscle invasion with cramping pain, low-grade fever and a firm 'woody/doughy' muscle but NO abscess (easily mistaken for a strain, contusion or DVT); STAGE 2 (suppurative) - a frank intramuscular ABSCESS with fever and increasing pain (most patients present here and need drainage) - fluctuance is unreliable in deep muscle and its absence does NOT exclude an abscess; and STAGE 3 (late) - systemic SEPSIS, bacteraemia, metastatic abscesses and complications.
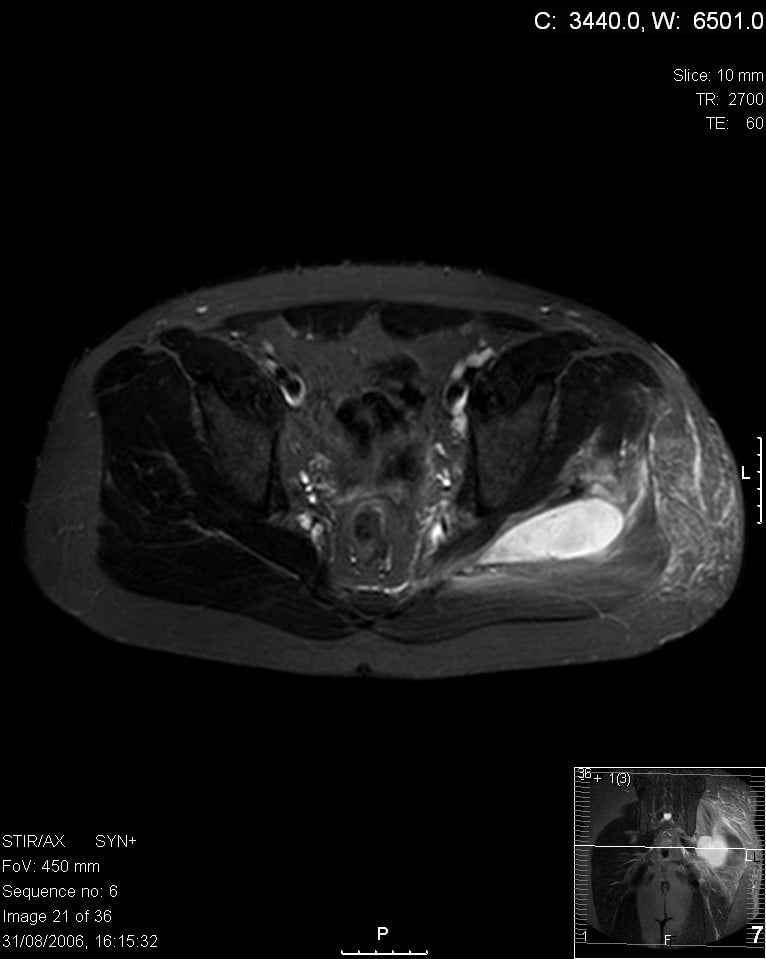
- MRI is the KEY diagnostic tool - it shows the muscle oedema of the early invasive stage and defines the abscess (rim-enhancing collection) and its extent for the suppurative stage; ULTRASOUND and CONTRAST CT are alternatives when MRI is unavailable, and inflammatory markers and blood/abscess cultures guide treatment, with raised CRP/white cells and a positive culture (often S. aureus) supporting the diagnosis.
- The KEY DIFFERENTIAL is from a muscle strain/contusion or DVT (early stage), and from osteomyelitis, septic arthritis, necrotising fasciitis and soft-tissue tumour - the distinguishing feature is a PRIMARY intramuscular abscess on imaging; necrotising fasciitis (a surgical emergency with rapidly spreading fasciocutaneous necrosis and systemic toxicity) must not be missed.
- MANAGEMENT is ANTIBIOTICS plus DRAINAGE/DEBRIDEMENT of the abscess: the early invasive stage may resolve with antibiotics alone, but an established abscess (the usual presentation) requires drainage - image-guided aspiration for small/accessible collections or open surgical debridement for larger/multiloculated ones - with antibiotics tailored to culture (covering MRSA empirically where prevalent); prompt surgical debridement with culture-directed antibiotics gives a high recovery rate, but a proportion progress to OSTEOMYELITIS, so vigilance for bone involvement and sepsis is essential.
- “Pyomyositis = PRIMARY bacterial muscle abscess (not spread from bone); S. aureus (incl. MRSA) commonest; large muscles (thigh/glutei/iliopsoas); often after trauma; tropical but now also temperate/adult/immunocompromised.
- “3 stages: invasive (woody muscle, no abscess - mimics strain/DVT) -> suppurative (abscess - DRAIN) -> late (sepsis). MRI is the key diagnostic tool.
- “Treat with culture-directed antibiotics (cover MRSA) + DRAINAGE/debridement of the abscess. Watch for osteomyelitis, septic arthritis and sepsis.
Pain, fever and a firm, woody large muscle (thigh/glutei/iliopsoas) - fluctuance often never appears - often after trauma. Early it mimics a strain/contusion/DVT - MRI shows muscle oedema then a rim-enhancing abscess.
Culture-directed antibiotics (cover MRSA) + drainage/debridement of the abscess. Watch for osteomyelitis, septic arthritis and sepsis. Exclude necrotising fasciitis (emergency).
What It Is, Who Gets It, and How It Presents
Pyomyositis is a primary bacterial infection of skeletal muscle with intramuscular abscess formation, arising within the muscle (often haematogenously) rather than spreading from adjacent bone. It is classically tropical and paediatric but is increasingly seen in temperate climates and adults, especially with immunocompromise (diabetes, HIV), and often follows minor trauma. The commonest organism is Staphylococcus aureus (including MRSA), and large muscles - quadriceps/thigh, gluteal, iliopsoas - are typically affected. It evolves through three stages: invasive (woody muscle, no abscess), suppurative (frank abscess - the usual presentation), and late (systemic sepsis and complications).
Pathogenesis: Why Muscle, and the Two-Hit Mechanism
Pyomyositis arises haematogenously yet frequently follows minor trauma, and one mechanism reconciles those two facts. The paradox is that normal skeletal muscle is remarkably resistant to blood-borne infection: even during a transient bacteraemia, intact, well-perfused muscle is very rarely seeded. Pyomyositis therefore needs a local susceptibility before a passing organism can take hold - the "two-hit" mechanism.
Blunt trauma, vigorous exercise, or pre-existing muscle damage (viral or parasitic myositis - one reason the disease is common in the tropics) creates a devitalised focus / microhaematoma - a locus minoris resistentiae. This is why most patients give a history of recent trauma, and why bulky, exercise-loaded lower-limb muscles (quadriceps, glutei, iliopsoas) are the typical sites.
A transient Staphylococcus aureus bacteraemia then seeds the injured muscle, where the haematoma is an ideal culture medium and the local defences are impaired. Host factors lower the threshold further - HIV (the major driver of the temperate-world rise), diabetes, malignancy, steroids and other immunocompromise - so an unexplained muscle abscess should prompt a search for occult immunocompromise.
Microbiology Beyond Staphylococcus aureus
Staphylococcus aureus (including MRSA) is the dominant organism, but empirical therapy and the differential depend on the wider spectrum - particularly because the immunocompromised host broadens it.
- Staphylococcus aureus (incl. MRSA) - the large majority; MRSA drives the aggressive temperate cases.
- Group A beta-haemolytic Streptococcus (S. pyogenes) - the second commonest, more aggressive and able to blur into a necrotising soft-tissue infection.
- Gram-negatives (E. coli, Klebsiella, Pseudomonas; Salmonella in sickle-cell disease), anaerobes, and mycobacteria/fungi - mainly in the immunocompromised, diabetic or HIV-positive host and in chronic/atypical presentations.
Empirical cover must include S. aureus/MRSA (where prevalent) and streptococci, and should be broadened to Gram-negatives in the immunocompromised - then de-escalated to culture. Detailed agent selection, dosing and duration are covered in the Orthopaedic Antibiotic Therapy topic; the point here is to match the empirical net to the host.
Staph aureus is far and away the commonest; Group A streptococcus is the classic second; think Gram-negatives, anaerobes and atypicals (and look for HIV/immunocompromise) when the host is not a healthy child or the course is unusual.
Diagnosis & Differential
- MRI is the key diagnostic tool - muscle oedema in the invasive stage and a rim-enhancing abscess with its extent in the suppurative stage; ultrasound/contrast CT are alternatives when MRI is unavailable.
- Bloods/cultures: raised CRP and white cells; blood and abscess cultures (often S. aureus) guide antibiotics.
- Differential: muscle strain/contusion or DVT (early); osteomyelitis, septic arthritis, necrotising fasciitis (a surgical emergency - do not miss), and soft-tissue tumour - the discriminator is a primary intramuscular abscess on imaging.
Two Findings That Mislead: Absent Fluctuance and a Normal CK
Stage 2 is described as the suppurative stage with fluctuance, and both halves of that sentence set traps.
Fluctuance is frequently absent, and its absence excludes nothing. These abscesses sit deep within bulky muscle bellies enclosed by investing fascia, so the pus is held away from the examining hand - the overlying skin is often entirely normal, with woody induration rather than a soft, fluctuant swelling. Fluctuance is therefore a late and unreliable sign, and waiting for it is one of the ways drainage gets delayed. That is precisely why the diagnosis rests on MRI rather than on palpation: a rim-enhancing intramuscular collection is an abscess whether or not it can be felt as one.
A normal creatine kinase does not exclude it either - and is actually a clue. CK is typically normal or only mildly raised in pyomyositis, because the process is a focal, walled-off collection rather than widespread myocyte breakdown. That is the opposite of a primary inflammatory myositis, where CK is substantially elevated, so the combination of a hot, tender muscle with high inflammatory markers and a normal CK points towards infection rather than inflammation. It is a discriminator that the framing follows from HIV and the Musculoskeletal System, and the inflammatory myopathies themselves are in Dermatomyositis and Polymyositis.
The practical consequence of both is the same: in a patient with fever, focal muscle pain and raised CRP, neither a soft-feeling muscle nor a normal CK is a reason to defer imaging.
Management
- Early invasive stage: may resolve with antibiotics alone (covering S. aureus/MRSA empirically where prevalent).
- Established abscess (usual): drainage - image-guided aspiration for small/accessible collections, or open surgical debridement for larger/multiloculated ones - with culture-directed antibiotics.
- Monitor: clinical and inflammatory-marker response; watch for osteomyelitis, septic arthritis and sepsis, which change the management.
- Support: treat sepsis, optimise comorbidities (glycaemic control), and address any immunocompromise.
How long, and when to switch. The course follows the same rules as musculoskeletal infection elsewhere, so one set of figures applies: intravenous until the patient is afebrile with a falling CRP - typically 3 to 5 days - then oral to complete a total of about 3 to 6 weeks, with the CRP checked weekly. A CRP that plateaus or climbs means an undrained or re-accumulating collection, or a metastatic focus, and should prompt re-imaging rather than a longer prescription. Multifocal disease, proven bacteraemia or endocarditis extends the course. The same thresholds are used in Paediatric Acute Osteomyelitis and Paediatric Psoas Abscess, where the psoas is simply pyomyositis in a particular muscle.
HIV is named as the single largest driver of pyomyositis appearing outside the tropics, which makes it an instruction rather than a piece of epidemiology. Offer an HIV test to any patient presenting with pyomyositis in a temperate setting, particularly where there is no obvious preceding muscle injury, the disease is multifocal, or the patient is an adult with no other explanation for immunocompromise.
The same logic applies to the rest of the host work-up: check glucose and HbA1c for undiagnosed diabetes, and take a history for steroids, malignancy, injecting drug use and cirrhosis. A muscle abscess in a previously healthy-seeming adult is a presenting feature of an immunocompromising condition often enough that finding one changes the patient's long-term management far more than the abscess does. In advanced HIV, also send the pus for mycobacterial and fungal culture, not only routine bacteriology - the wider spectrum in that host is set out in HIV and the Musculoskeletal System.
The two traps in pyomyositis are missing it early and under-treating it late. In the invasive stage the firm, painful muscle is easily dismissed as a strain, contusion or DVT, so a low threshold for MRI - which shows the muscle oedema and then the rim-enhancing abscess - is what makes the diagnosis. Once an abscess has formed, antibiotics alone are usually insufficient: the collection must be drained, by image-guided aspiration if small and accessible or by open debridement if large or multiloculated, with antibiotics directed by culture and covering MRSA empirically where it is prevalent. Throughout, remain vigilant for progression - a proportion develop osteomyelitis, and untreated disease advances to bacteraemia, metastatic abscesses and septic shock - and keep necrotising fasciitis, a true surgical emergency, in the differential when there is rapidly spreading necrosis and disproportionate systemic toxicity.
Mnemonics & Memory Aids
PUS
Hook:PUS: Primary Staph muscle abscess, Use MRI, Stages + Surgical drainage + Sepsis vigilance.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has fever and a painful, firm thigh after minor trauma. Over days it becomes fluctuant. What is your diagnosis and management?”
What it is
- Primary bacterial infection of skeletal muscle with intramuscular abscess
- S. aureus commonest (incl. MRSA); large muscles (thigh/glutei/iliopsoas); often post-trauma
- Tropical/paediatric classically; now also temperate/adult/immunocompromised
Stages
- 1 Invasive: woody muscle, no abscess (mimics strain/contusion/DVT)
- 2 Suppurative: frank abscess (usual presentation - drain)
- 3 Late: systemic sepsis, metastatic abscesses, complications
Diagnosis
- MRI is the key tool (oedema -> rim-enhancing abscess)
- Ultrasound/contrast CT if MRI unavailable; raised CRP/WCC
- Blood/abscess cultures; exclude necrotising fasciitis
Management
- Early: antibiotics alone may suffice (cover MRSA)
- Abscess: drainage (aspiration or open debridement) + culture-directed antibiotics
- Watch for osteomyelitis, septic arthritis and sepsis
Evidence & Key Studies
Primary purulent infectious myositis (pyomyositis) of the extremities in children
- In 53 children with primary purulent infectious myositis (pyomyositis) of the extremities, the lower extremity was involved in 69% and a history of trauma preceded symptoms in 69%; Staphylococcus aureus was identified in 69% of cultures.
- MRI was the most important diagnostic tool, especially for differential diagnosis; when unavailable, physical examination, laboratory parameters, other imaging and needle aspiration support the surgical decision.
- After rapid surgical debridement, full recovery was achieved in 95%, but osteomyelitis developed during follow-up in 10%, underscoring the need for prompt drainage and vigilance for bone involvement.
Pyomyositis in a healthy adult in a temperate region (MRSA)
- Pyomyositis, traditionally prevalent in the tropics, is increasingly diagnosed in temperate climates and in otherwise healthy individuals, and its nonspecific symptoms often delay diagnosis, requiring advanced imaging.
- A healthy adult developed extensive abscesses due to methicillin-resistant Staphylococcus aureus; linezolid gave only partial improvement and recurrent abscesses required surgical drainage.
- An integrated approach of antimicrobial therapy plus surgical intervention achieved recovery, highlighting the aggressive nature of MRSA and the need for prompt diagnosis and combined treatment.
The epidemiology (lower-limb predominance, frequent preceding trauma, S. aureus in most cultures), the central role of MRI, and the outcomes of prompt debridement (high recovery but a 10% rate of osteomyelitis) come from the cited Zeybek paediatric series; the increasing occurrence in temperate climates and healthy adults, the role of MRSA, and the need for combined antibiotic-and-surgical treatment from the cited Saad report. The three-stage classification (invasive/suppurative/late) and the differential with strain/DVT, osteomyelitis, septic arthritis and necrotising fasciitis are standard, well-established teaching, as is the unreliability of fluctuance in a deep, fascia-enclosed muscle. The normal-or-mildly-raised creatine kinase as a discriminator from primary inflammatory myositis follows HIV and the Musculoskeletal System, and the antibiotic durations and CRP monitoring follow Paediatric Acute Osteomyelitis, so the same figures apply across the musculoskeletal infection topics. (See also Necrotizing Fasciitis, Paediatric Psoas Abscess, Paraspinal Abscess and Dermatomyositis and Polymyositis.)