A Mimic of Hip Septic Arthritis
- A PSOAS (iliopsoas) ABSCESS is a collection of pus within the psoas/iliacus muscle; PRIMARY abscesses arise HAEMATOGENOUSLY (most often Staphylococcus aureus, including MRSA) in otherwise healthy children, while SECONDARY abscesses spread from an adjacent source - spinal osteomyelitis/discitis, bowel disease, or renal/retroperitoneal infection - so the source must be sought.
- The KEY clinical lesson is that the paediatric psoas abscess MIMICS HIP SEPTIC ARTHRITIS (and sometimes appendicitis): the child is FEBRILE and TOXIC, holds the HIP FLEXED, resists EXTENSION (a positive PSOAS sign), limps or refuses to weight-bear, and may have flank/back/groin pain - so a HIGH INDEX OF SUSPICION is needed to avoid misdiagnosis.
- INVESTIGATION shows raised WHITE CELLS and inflammatory markers (CRP), usually NORMAL plain radiographs, and MRI as the KEY diagnostic tool - it defines the abscess and its extent and detects any SPINAL source; ULTRASOUND and contrast CT are alternatives, and blood and abscess CULTURES guide antibiotics.
- The DIFFERENTIAL is principally hip SEPTIC ARTHRITIS, but also transient synovitis, osteomyelitis (femur/pelvis/spine), discitis, appendicitis and pyomyositis - and distinguishing a psoas abscess from a septic hip changes the management (drainage of the psoas collection rather than arthrotomy of the hip), which is why imaging is decisive.
- MANAGEMENT is ANTIBIOTICS plus DRAINAGE: empirical antibiotics covering S. aureus/MRSA (then culture-directed), and DRAINAGE of the abscess - IMAGE-GUIDED aspiration for small/accessible collections, or OPEN (retroperitoneal) drainage for larger or loculated ones - prompt imaging and appropriate treatment (drainage plus antibiotics) give good outcomes, with the child typically recovering full function.
- Any SECONDARY SOURCE (spinal osteomyelitis/discitis, GI or renal infection) must be IDENTIFIED and TREATED, and the child monitored for progression/complication; the prognosis with timely diagnosis and treatment is good, but delay (from mistaking it for transient synovitis) risks ongoing sepsis.
- “Pediatric psoas abscess = pus in psoas/iliacus; PRIMARY (haematogenous, S. aureus/MRSA) vs SECONDARY (spine/GI/renal source). MIMICS hip septic arthritis/appendicitis.
- “Presentation: fever + toxic child + HIP HELD FLEXED, painful on EXTENSION (positive PSOAS sign) + limp/refusal to weight-bear + flank/back pain. Raised CRP/WCC; plain films usually normal.
- “MRI is the KEY diagnostic tool (also defines a spinal source). Treat with antibiotics (cover MRSA) + DRAINAGE - IMAGE-GUIDED percutaneous is first-line, open retroperitoneal the fallback, never through the hip joint; find/treat any secondary source. High index of suspicion.
Febrile, toxic child with the hip held flexed, pain on hip extension (positive psoas sign), limp, and flank/back pain - mimics hip septic arthritis. Raised CRP/WCC; plain films usually normal.
MRI is the key test (and finds a spinal source). Treat with antibiotics (cover MRSA) + drainage - image-guided percutaneous first-line, open retroperitoneal as fallback; identify any secondary source.
Iliopsoas Anatomy and the Basis of the Psoas Sign
The clinical picture - the flexed hip, the pain on extension and the flank/groin/thigh pain - follows directly from iliopsoas anatomy, which also explains how the abscess spreads and why it is drained retroperitoneally.
- Psoas major arises from the bodies, intervertebral discs and transverse processes of T12-L5 and runs retroperitoneally within the psoas (fascial) sheath, anterior to the lumbar transverse processes.
- Iliacus arises from the iliac fossa and joins the lateral psoas; together they pass under the inguinal ligament to insert by a common tendon on the lesser trochanter.
- Action: the primary hip flexor (also a lateral rotator and trunk flexor). The lumbar plexus and femoral nerve (L1-L3 contributions) lie within and on the muscle.
- The hip is held flexed because flexion relaxes the inflamed psoas (position of comfort), shortening the muscle and easing tension on the abscess.
- Pain on hip extension (the psoas sign) occurs because extension stretches the inflamed muscle; resisted active hip flexion is also painful.
- Because the psoas is retroperitoneal, the abscess causes flank/back and groin pain and can track distally along the muscle below the inguinal ligament toward the lesser trochanter, presenting as a groin/thigh swelling.
Spread pathways and surgical relevance: pus within the psoas sheath can extend cranially toward the spine (or arrive from it) and caudally into the thigh, and the muscle lies close to the lumbar plexus and femoral nerve, ureter, kidney and bowel - which is why a secondary source (spine, bowel, kidney) must be sought and why the deep retroperitoneal collection is drained retroperitoneally or by an image-guided percutaneous catheter, never through the hip joint.
Separating It From a Septic Hip at the Bedside
Imaging settles the question, but the examination should have raised it, and the discriminator follows from which structure each condition irritates.
- Psoas abscess
- Hip flexed - flexion shortens and relaxes the inflamed psoas
- Septic arthritis of the hip
- Hip flexed, ABDUCTED and externally rotated - the position of maximum capsular volume and therefore lowest intra-articular pressure
- Psoas abscess
- Relatively tolerated - rotation does not lengthen psoas much
- Septic arthritis of the hip
- Resisted and painful - rotation stresses the distended capsule. This is the single most useful bedside discriminator
- Psoas abscess
- The painful movement - it stretches the inflamed muscle (the psoas sign). Resisted active flexion also hurts
- Septic arthritis of the hip
- Painful, but not selectively more so than rotation
- Psoas abscess
- Flank, back, iliac fossa, groin; sometimes a tracking thigh swelling below the inguinal ligament
- Septic arthritis of the hip
- Anterior joint line and groin, with global irritability
- Psoas abscess
- Usually no effusion - but see the caveat below
- Septic arthritis of the hip
- Effusion present; aspiration confirms
The ultrasound caveat matters more than the rule. An absent hip effusion supports a psoas abscess, but it does not exclude a septic hip in the first hours, and - more importantly - a psoas abscess adjacent to the joint can produce a sympathetic effusion, and the two can coexist, because the abscess may decompress into the joint or the joint infection may track into the muscle. So an effusion does not exclude a psoas abscess either. Where the picture is not clean, the answer is cross-sectional imaging of the whole region rather than a decision made on the ultrasound alone.
The hip-specific rules do not settle this. The Kocher criteria were derived to separate a septic hip from transient synovitis, so a psoas abscess can score fully on them and still not be a joint infection - the same limitation that lets pelvic infection be missed, set out in Paediatric Pelvic Osteomyelitis. The joint itself is covered in Septic Arthritis of the Paediatric Hip.
Microbiology and Aetiology
The organism dictates empirical antibiotics, so the aetiological spectrum is high-yield.
- Typical organisms
- Staphylococcus aureus, including MRSA; occasionally Streptococcus
- Notes
- Otherwise-healthy child; the muscle is seeded from transient bacteraemia (often a skin/soft-tissue focus). Empirical cover must include MRSA where prevalent.
- Typical organisms
- Polymicrobial enteric Gram-negatives (E. coli) plus anaerobes
- Notes
- Add Gram-negative and anaerobic cover; treat the bowel source.
- Typical organisms
- Gram-negatives (E. coli, Proteus)
- Notes
- Consider urinary-tract imaging and culture.
- Typical organisms
- Mycobacterium tuberculosis
- Notes
- Tracks down from spinal Pott's disease; indolent and cool with little warmth/erythema; needs anti-tuberculous therapy; the spinal disease is developed separately (linked below).
A pyogenic psoas abscess (commonly S. aureus/MRSA) is acute, febrile and toxic, whereas the classic tuberculous ("cold") abscess is indolent with little warmth or systemic toxicity and tracks down from spinal Pott's disease. In the cited immunocompetent child the Mantoux was negative and culture grew MRSA, treated successfully with linezolid after open retroperitoneal drainage; but in TB-endemic regions tuberculosis must be actively excluded (it was historically the dominant cause). This MRSA pyogenic case (Keny 2025) recovered fully, walking by 6 weeks.
Antibiotic principle: begin IV empirical cover for S. aureus/MRSA (an anti-staphylococcal agent plus an MRSA-active drug such as vancomycin, clindamycin or linezolid), broaden to enteric Gram-negative and anaerobic cover if a GI source is suspected, then narrow to culture-directed therapy; switch IV-to-oral on clinical and CRP response, with a longer total course where there is associated osteomyelitis/discitis, and anti-tuberculous therapy if TB is confirmed.
Presentation, Investigation & Differential
A psoas (iliopsoas) abscess is pus within the psoas/iliacus muscle - primary (haematogenous, often S. aureus/MRSA) in healthy children, or secondary (from spine/bowel/kidney). It classically mimics hip septic arthritis: a febrile, toxic child holds the hip flexed, resists extension (positive psoas sign), limps and has flank/back/groin pain. Investigation shows raised white cells/CRP, usually normal plain radiographs, and MRI as the key diagnostic tool (defining the abscess and any spinal source), with ultrasound/CT as alternatives and cultures to guide antibiotics. The differential includes septic hip, transient synovitis, osteomyelitis/discitis, appendicitis and pyomyositis - so imaging is decisive.
- Antibiotics: empirical cover for S. aureus/MRSA, then culture-directed.
- Drainage: image-guided percutaneous drainage is the first-line approach for a drainable collection - aspiration or catheter placement under ultrasound or CT guidance. Open retroperitoneal drainage is the fallback, not the default.
- Find/treat any secondary source: spinal osteomyelitis/discitis, GI or renal infection.
- Monitor: clinical and inflammatory-marker response; watch for progression; prognosis good with timely treatment.
Which collections actually need draining, and by what route. The decision is not simply large-versus-small.
- Approach
- Antibiotics alone, with imaging repeated if the response stalls
- Why
- Not every collection needs a needle; phlegmon without organised pus will not yield
- Approach
- IMAGE-GUIDED percutaneous drainage - ultrasound or CT guided, catheter left for larger cavities
- Why
- Avoids an open retroperitoneal approach and its morbidity, and yields the organism, which is often the only positive culture
- Approach
- OPEN retroperitoneal drainage
- Why
- Septations defeat a single catheter
- Approach
- Address the source, with the abscess drained at the same time
- Why
- Draining the collection while leaving the source guarantees recurrence
- Approach
- NOT through the hip joint
- Why
- The collection is retroperitoneal; crossing the joint contaminates a clean space
Duration follows the same rules as osteomyelitis elsewhere, so one set of figures applies: intravenous until the child is afebrile with a falling CRP - typically 3 to 5 days - then oral to complete a total of about 3 to 6 weeks, with CRP tracked weekly. A CRP that plateaus or climbs means an undrained or re-accumulating collection and should prompt repeat imaging rather than a longer prescription. Associated vertebral osteomyelitis or discitis lengthens the course - see Paediatric Acute Osteomyelitis and Pyogenic Discitis and Osteomyelitis.
Look for a vein thrombosis in the sick child. The abscess sits directly on the iliac vessels, and severe staphylococcal infection - particularly PVL-positive strains - is associated with septic thrombophlebitis and pulmonary emboli. In a child who is toxic, has a very high CRP or develops chest signs, image the veins.
The central safety point in the paediatric psoas abscess is that it masquerades as hip septic arthritis: the child is febrile and toxic with a flexed, irritable hip that is painful on extension and refuses to weight-bear, exactly the picture that prompts a hip ultrasound and possible arthrotomy. Recognising that the psoas, not the hip joint, is the source matters because the treatment differs - drainage of the psoas collection (image-guided or open retroperitoneal) plus antibiotics, rather than hip arthrotomy - and this distinction is made by imaging, with MRI the key modality, which also reveals a spinal osteomyelitis/discitis source if present. The two errors to avoid are dismissing the child as transient synovitis (delaying treatment of a true abscess and ongoing sepsis) and overlooking a secondary source. With prompt imaging, appropriate antibiotics covering S. aureus/MRSA, and timely drainage, the prognosis is good and children typically recover full function.
Mnemonics & Memory Aids
PSOAS
Hook:PSOAS: Pus in psoas (primary/secondary), Septic-hip mimic, On extension hurts (psoas sign), Assess with MRI, Solution = antibiotics + drainage + find Source.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A febrile child holds the hip flexed and screams on extension, refusing to walk. The hip ultrasound shows no effusion. What are you thinking, and how do you proceed?”
What it is
- Pus within psoas/iliacus muscle
- Primary: haematogenous (often S. aureus/MRSA), healthy child
- Secondary: from spine (osteomyelitis/discitis), bowel, kidney
Presentation (mimics septic hip)
- Fever, toxic child; hip held flexed, painful on extension (positive psoas sign)
- Limp/refusal to weight-bear; flank/back/groin pain
- Raised WCC/CRP; plain radiographs usually normal
Diagnosis & management
- MRI = key diagnostic tool (defines abscess + any spinal source); US/CT alternatives; cultures
- Antibiotics (cover MRSA), then culture-directed; IV until afebrile + falling CRP (~3-5 days), then oral; total ~3-6 weeks; CRP weekly
- Drainage: image-guided percutaneous FIRST-LINE; open retroperitoneal if multiloculated or percutaneous fails; NEVER through the hip joint
- Rotation of the flexed hip relatively spared (vs septic hip); an absent effusion does not exclude either, and they can coexist
- Find/treat secondary source; image the veins in the toxic child (septic thrombophlebitis)
Evidence & Key Studies
Primary pyogenic psoas abscess in an immunocompetent child
- Pyogenic psoas abscess is a rare but severe condition; once linked mainly to tuberculosis, it now has diverse causes, and can present in healthy (immunocompetent) children, initially suspected to be a hip problem.
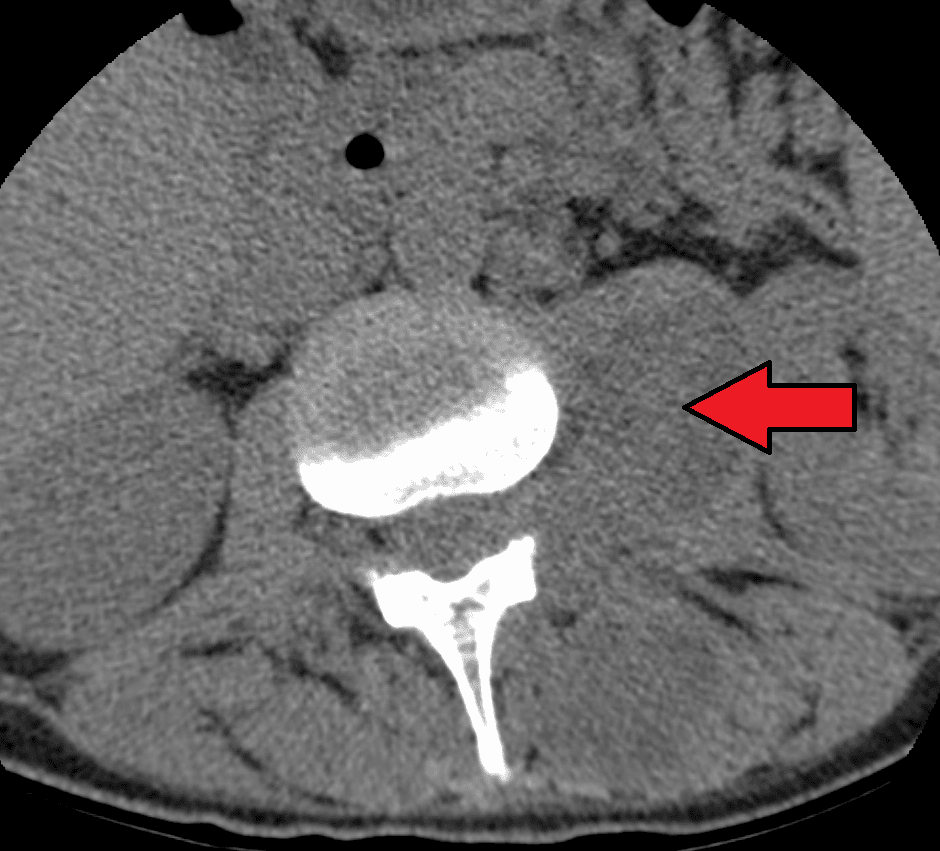
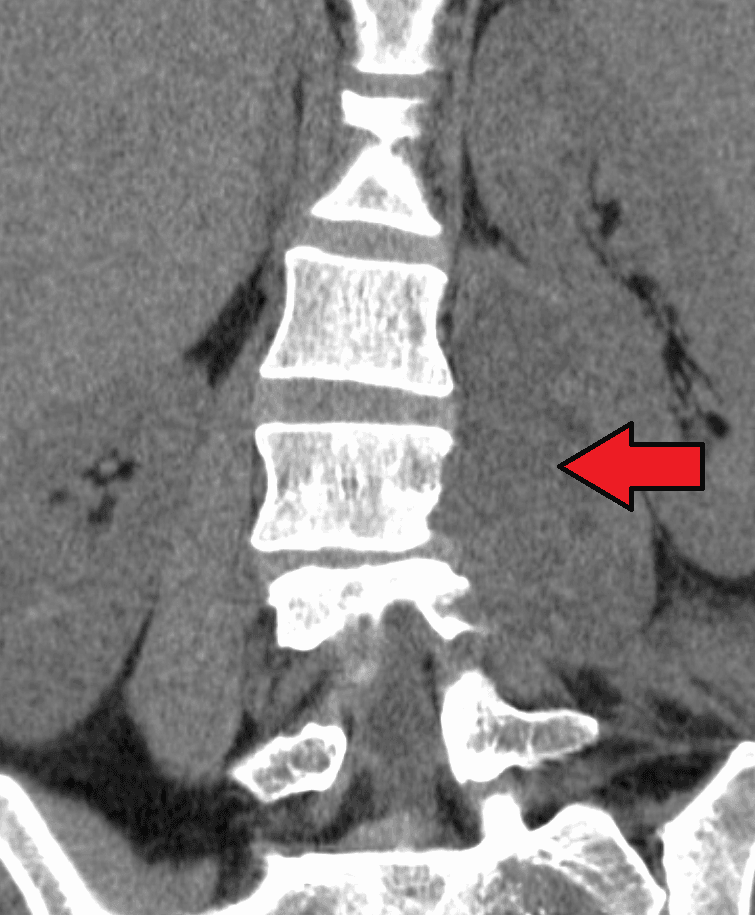
- The child was febrile and toxic with the hip held flexed and painful/restricted movement, raised white cells and inflammatory markers, and normal lumbosacral radiographs; MRI demonstrated a large psoas/iliacus abscess, and culture grew MRSA.
- Open retroperitoneal drainage plus antibiotics led to full recovery; the case emphasises a high index of suspicion (it mimics septic arthritis) and the importance of timely imaging and drainage-plus-antibiotic treatment.
The presentation of a paediatric pyogenic psoas abscess as a mimic of hip pathology (febrile, toxic child with a flexed, restricted hip), the normal plain radiographs with MRI demonstrating the abscess, the MRSA aetiology, and the management by drainage (open retroperitoneal) plus antibiotics with full recovery come from the cited Keny report. The primary (haematogenous) vs secondary (spinal/GI/renal) classification, the psoas sign, the differential with septic arthritis/transient synovitis/osteomyelitis, and image-guided versus open drainage are standard, well-established teaching. Note that the cited case was drained openly, which is a single report and not an argument for open drainage as the default - image-guided percutaneous drainage is first-line where the collection is accessible. The antibiotic durations, the IV-to-oral criterion and the CRP monitoring follow Paediatric Acute Osteomyelitis, so the same figures apply wherever the infection sits. (See also Septic Arthritis of the Paediatric Hip, Paediatric Pelvic Osteomyelitis, Pyogenic Discitis and Osteomyelitis, Pyomyositis and Tuberculosis of the Spine (Pott's Disease).)