& Sacroiliac Joint Infection in Children
- Pelvic osteomyelitis and septic sacroiliitis in children have a VAGUE, non-localising presentation - a limp or refusal to weight-bear, fever, and pain referred to the HIP, BUTTOCK, GROIN, THIGH or LOW BACK - so they are frequently MISDIAGNOSED or diagnosed LATE, mistaken for a septic hip, transient synovitis, discitis, a spinal problem or even an abdominal cause such as appendicitis.
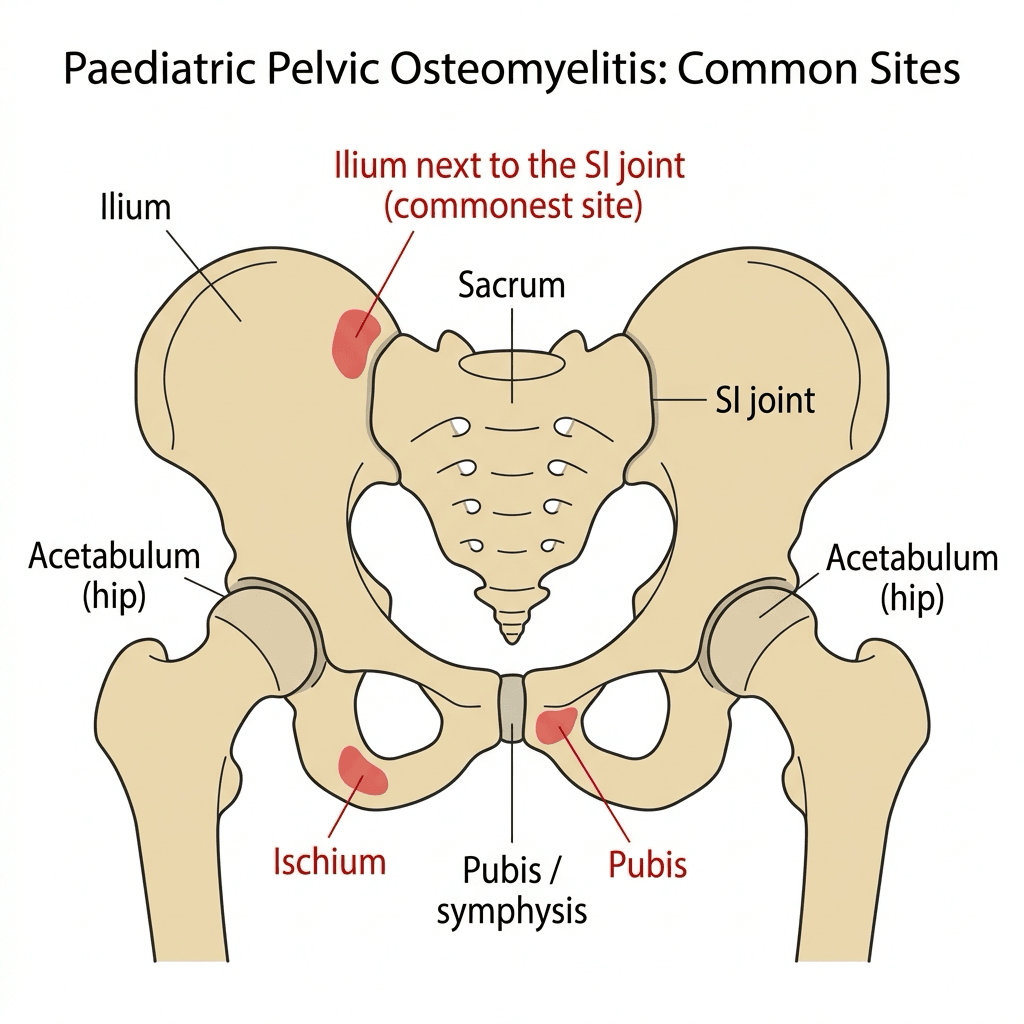
- Haematogenous osteomyelitis seeds 'METAPHYSEAL EQUIVALENTS' - portions of flat or irregular bone adjacent to cartilage with a similar sluggish vascular anatomy to a long-bone metaphysis; the pelvis has several, and the SACROILIAC JOINT region is the most frequently involved, with the ilium, pubis, ischium and the triradiate cartilage also affected - which is why pelvic infection often straddles bone and the adjacent SI joint (septic sacroiliitis).
- MRI is the KEY diagnostic test: it is sensitive early (showing bone-marrow oedema and surrounding soft-tissue change before plain radiographs become abnormal), it defines any abscess that would need drainage, and it distinguishes the diagnosis from the mimics; plain radiographs are often NORMAL in the early phase, and inflammatory markers (CRP/ESR) and blood cultures support the diagnosis.
- STAPHYLOCOCCUS AUREUS is the predominant organism (consider Kingella kingae in younger children and Salmonella in sickle-cell disease); a tissue or blood diagnosis should be sought, and a subacute focus can present as a BRODIE'S ABSCESS in pelvic bone, which mimics infection, tuberculosis and benign or malignant bone tumours - so biopsy/curettage is sometimes needed to confirm the diagnosis and exclude tumour.
- MANAGEMENT is ANTIBIOTIC-led: appropriate empirical antibiotics (covering S. aureus, guided by local protocols and culture) started after attempting to obtain a microbiological diagnosis, with most children responding to antibiotics alone; SURGICAL DRAINAGE is reserved for a drainable ABSCESS, for septic arthritis of the SI joint not responding, or for failure to improve.
- Because the diagnosis is so easily missed, the practical rule is to keep pelvic/SI-joint infection in the differential of the LIMPING, FEBRILE CHILD - especially when the hip examination is relatively unremarkable or pain localises to the buttock/back - and to use MRI early; timely treatment usually gives an excellent outcome, whereas delay risks abscess, chronicity and growth disturbance.
- “Pelvic osteomyelitis/septic sacroiliitis = the GREAT MIMIC of the limping febrile child (hip/buttock/back pain) - frequently missed/delayed.
- “Metaphyseal-equivalent concept: SI joint region most common pelvic site (also ilium/pubis/ischium/triradiate). MRI is the key test; plain films often normal early.
- “S. aureus predominates; ANTIBIOTIC-led management, drainage only for abscess/non-response; a subacute focus = Brodie's abscess (exclude tumour/TB).
Limp/refusal to weight-bear + fever with pain in hip, buttock, groin, thigh or low back - and a relatively unremarkable hip exam. A great mimic, often diagnosed late.
Get an MRI early (plain films often normal); cover S. aureus; drain only an abscess.
Presentation, Sites & Diagnosis
Pelvic osteomyelitis and septic sacroiliitis present vaguely: a child with a limp or refusal to weight-bear, fever, and pain that may localise to the hip, buttock, groin, thigh or low back - so they are frequently mistaken for a septic hip, transient synovitis, discitis or even appendicitis, and diagnosis is often delayed. The reason the pelvis is involved is the metaphyseal-equivalent concept: flat/irregular bones have regions adjacent to cartilage with metaphysis-like vascularity that seed haematogenous infection, and the sacroiliac joint region is the most frequent pelvic site (with ilium, pubis, ischium and triradiate cartilage). MRI is the key test - sensitive early and able to define an abscess - while plain films are often normal early; Staphylococcus aureus predominates.
The Imaging and Laboratory Pathway
MRI is the key test and plain films are often normal early, but each investigation contributes something different, and knowing which question each one answers is what makes the pathway usable rather than a list.
Raised CRP and ESR (CRP rises and falls faster - better for monitoring response), a raised white-cell count, and blood cultures taken before antibiotics (positive in a proportion). Image-guided aspiration/biopsy gives the organism for a localised or atypical focus.
- Plain radiograph first but often normal early (lysis/sclerosis/periosteal reaction lag by about one to two weeks); helps exclude other causes.
- MRI is the gold standard - marrow oedema, the SI joint, and any abscess needing drainage; image the whole pelvis.
- Bone scintigraphy / SPECT-CT when MRI is unavailable or to survey for multifocal disease.
- CT for bony detail and to guide biopsy; ultrasound for an SI/soft-tissue effusion or abscess and to guide aspiration.
Bloods (CRP/ESR + cultures) plus MRI is the workhorse; plain films lag (often normal early), bone scan/SPECT-CT surveys for multifocality when needed, and CT/ultrasound guide sampling/drainage. Use CRP to track the response.
Organisms & Management
- Get a diagnosis where possible. Inflammatory markers (CRP/ESR), blood cultures, and - for a localised or atypical focus - image-guided aspiration/biopsy; a subacute pelvic focus may be a Brodie's abscess that mimics tuberculosis and bone tumours, so biopsy/curettage is sometimes needed to confirm and exclude tumour.
- Cover the likely organism. S. aureus predominates; consider Kingella kingae in younger children and Salmonella in sickle-cell disease. Start empirical antibiotics per local protocol after sampling.
- Antibiotics are the mainstay. Most children respond to appropriately chosen antibiotics alone. Switch
from intravenous to oral once the child is afebrile with a falling CRP - typically after 3 to 5 days
- and complete a total course of 3 to 6 weeks, around 3 weeks usually sufficing for uncomplicated disease. Track the CRP weekly.
- Drain when needed. Surgical drainage is reserved for a drainable abscess, for SI-joint sepsis not responding, or for failure to improve on antibiotics.
"Antibiotic-led" needs a regimen attached to it. The course follows the same principles as acute haematogenous osteomyelitis elsewhere, and the figures below are taken from Paediatric Acute Osteomyelitis so that one set of numbers applies wherever in the skeleton the infection sits:
- What is done
- Blood cultures, and image-guided aspiration or biopsy of a localised or atypical focus
- The criterion for moving on
- Sampling first - unless the child is septic, in which case treat and sample what you can
- What is done
- Empirical cover for S. aureus per local protocol, refined to culture
- The criterion for moving on
- Typically 3 to 5 days - until AFEBRILE and the CRP is falling from its peak. The CRP does not have to be normal to switch
- What is done
- Culture-directed oral agent at appropriate dose
- The criterion for moving on
- Continues to complete the total course
- What is done
- 3 to 6 weeks; around 3 weeks is usually sufficient for uncomplicated disease
- The criterion for moving on
- Longer for abscess, delayed presentation, MRSA/PVL disease or a slow CRP response
- What is done
- CRP - it rises and falls faster than ESR, so it is the marker that tracks response; check weekly through the course
- The criterion for moving on
- A CRP that normalises within about 7 to 10 days marks the group that does well; a CRP that plateaus or rises means re-image for an undrained collection
Kingella kingae has to be actively looked for, not merely "considered". It is the leading organism in children aged roughly 6 to 48 months when PCR is used, and the reason for that qualifier is that it grows poorly on routine plates - a child with genuine Kingella infection frequently has negative conventional cultures. Inoculating samples into blood-culture bottles and requesting PCR, including oropharyngeal PCR, is what converts a culture-negative case into a diagnosis. The clinical picture is often milder, with lower fever and a lower CRP than staphylococcal disease, which is itself a reason the diagnosis gets missed twice over.
A subset of these children are not simply unwell but dangerously so, and the pattern is recognisable. Virulent Staphylococcus aureus - particularly community-acquired MRSA carrying the Panton-Valentine leukocidin (PVL) toxin - produces a far more aggressive illness: high fever and very high CRP, large and often multifocal abscesses, associated myositis, and a markedly higher requirement for surgery.
The complication to hunt for is venous. Severe PVL-positive staphylococcal osteomyelitis is associated with adjacent deep vein thrombosis and septic pulmonary emboli - and in the pelvis the veins concerned are large. So in a child who is toxic, whose CRP is very high, who has multifocal disease, or who develops chest signs or hypoxia: obtain venous Doppler imaging, look for pulmonary emboli, broaden to cover MRSA, and get source control. Treating this phenotype as though it were ordinary osteomyelitis is how these children deteriorate.
The recurring lesson of pelvic osteomyelitis and septic sacroiliitis is that they are MISSED because the presentation is non-specific and the hip examination can be relatively unremarkable, so a limping, febrile child with buttock or back pain - or a 'septic hip' that does not quite fit - should keep pelvic/SI-joint infection in the differential and prompt an EARLY MRI rather than waiting for plain films to change (which they often do not early). Equally, do not assume a destructive pelvic lesion is infective: a subacute focus can mimic, and be mimicked by, tuberculosis and bone tumours, so obtain tissue when the picture is atypical. Early diagnosis and antibiotic-led treatment usually give an excellent outcome; delay risks abscess, chronic infection and growth disturbance.
What Growth Disturbance Actually Means Here
Delay is said to risk growth disturbance, and in the pelvis that phrase has a specific and consequential meaning worth spelling out, because it determines how long the child is followed.
The triradiate cartilage is the acetabulum's growth plate. It is the Y-shaped physis where the ilium, ischium and pubis meet, and it is what expands the acetabulum to keep pace with the enlarging femoral head until it closes in early adolescence. It also sits on the list of pelvic metaphyseal equivalents, so it is a site infection reaches.
Damage to it does not declare itself at the time. The infection is treated, the child recovers, and the consequence appears over the following years as the acetabulum fails to grow: a progressively shallow, dysplastic acetabulum, with lateralisation and subluxation of the femoral head, and the secondary problems that follow from an incongruent hip. A premature partial closure can also produce asymmetrical growth and acetabular deformity rather than simple shallowness.
So the follow-up outlasts the infection. Where imaging showed involvement of the triradiate cartilage or the acetabulum, the child needs radiographic surveillance of the hip through skeletal maturity, not discharge once the CRP has normalised - because the treatable window for developing acetabular dysplasia is long before the hip becomes symptomatic. Tell the family this at the outset, so that years of appointments after an apparently cured infection make sense to them.
The same logic, less commonly, applies to infection crossing into the proximal femoral physis from a septic hip, which is covered in Septic Arthritis of the Paediatric Hip.
Localising the Source: the SI/Pelvic Exam and Why the Hip Misleads
A hip that examines relatively well in a febrile, limping child is reassuring only if the hip is the thing wrong with them. The signs that point instead to the pelvis and sacroiliac joint, and the reason the familiar hip rule does not apply to them, are what separate the two.
The Kocher criteria (fever, non-weight-bearing, raised ESR, raised WCC) were derived to separate a septic hip from transient synovitis - they are hip-specific and do NOT capture pelvic/SI-joint infection. So a child who does not fit Kocher, or who has a comparatively comfortable hip, can still have pelvic sepsis - which is exactly how the diagnosis is missed.
- Hip rotation/log-roll relatively preserved and not agonising (unlike the held, irritable hip of septic arthritis).
- Direct tenderness over the SI joint / posterior pelvis / pubis.
- Positive SI provocation tests - FABER (Patrick's), pelvic compression/distraction, Gaenslen's, and the flamingo/single-leg stand - reproduce buttock/SI pain.
Kocher is for the hip, not the pelvis. A febrile, limping child with a comfortable hip on log-roll but SI/buttock tenderness and positive SI provocation tests (FABER, pelvic compression) has pelvic/SI infection until MRI proves otherwise.
Mnemonics & Memory Aids
PELVIS
Hook:PELVIS: referred Pain, Easily missed, Limp+fever, View on MRI, Infection (S. aureus), SI joint + antibiotics.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child presents with a limp, fever and buttock pain, but the hip examination is relatively unremarkable. What are you worried about and how do you investigate?”
“How would you manage confirmed pelvic osteomyelitis or septic sacroiliitis in a child?”
Recognition
- Limp/refusal to weight-bear + fever; pain in hip/buttock/groin/thigh/low back
- Relatively unremarkable hip exam; a great mimic, often diagnosed late
- Differential: septic hip, transient synovitis, discitis, appendicitis
Sites & concept
- Metaphyseal equivalents (flat/irregular bone adjacent to cartilage) seed infection
- SI joint region most frequent; also ilium, pubis, ischium, triradiate cartilage
- Septic sacroiliitis straddles bone and joint
Diagnosis
- MRI is the key test (sensitive early; defines abscess)
- Plain films often normal early; CRP/ESR and blood cultures support
- S. aureus predominates (Kingella younger; Salmonella sickle cell)
Management
- Antibiotic-led after sampling; most respond to antibiotics alone
- IV until afebrile with falling CRP (~3-5 days), then oral; total 3-6 weeks (~3 uncomplicated); CRP weekly
- Drainage for abscess / non-responding SI sepsis / failure to improve
- Biopsy an atypical/destructive focus (Brodie's abscess mimics TB/tumour)
Don't miss
- Kingella (6-48 months) grows poorly - request PCR incl. oropharyngeal, or it stays culture-negative
- PVL-positive S. aureus: high CRP, multifocal abscesses - hunt for DVT (Doppler) and septic pulmonary emboli
- Triradiate involvement -> acetabular dysplasia years later; follow the hip radiographically to skeletal maturity
Evidence & Key Studies
Osteomyelitis of a sacral neurocentral synchondrosis: another pelvic metaphyseal equivalent
- Pelvic osteomyelitis occurs in 'metaphyseal equivalents' - portions of flat or irregular bone adjacent to cartilage.
- The pelvic bone has several metaphyseal equivalents, of which the sacroiliac joint is the most frequent site of involvement.
- Recognising additional metaphyseal equivalents (here a sacral neurocentral synchondrosis), especially in infants and younger children, aids diagnosis on MRI.
Brodie's abscess of the posterior ilium presenting as paediatric low back pain (gluteal syndrome)
- A Brodie's abscess (subacute osteomyelitis) of pelvic bone is rare and, in the posterior ilium, can present as low back pain and be easily missed or misdiagnosed.
- It resembles other pelvic and sacroiliac joint pathologies and the differential includes infection, tuberculosis and benign bone tumours - so biopsy/curettage may be needed; Staphylococcus aureus was cultured.
- Appropriate antibiotics (here six weeks after curettage) gave resolution without recurrence.
The metaphyseal-equivalent concept and the sacroiliac joint being the most frequent pelvic site come from the cited Miyazaki report; the vague, easily-missed presentation of a subacute pelvic focus (Brodie's abscess) with its differential of infection, tuberculosis and bone tumour, the role of biopsy, the S. aureus aetiology and antibiotic resolution from the cited Behera report. The general 'limping febrile child' presentation, the central role of early MRI, the Kingella/Salmonella considerations and the antibiotic-led (drainage-for-abscess) management are standard, well-established teaching. The antibiotic durations, the IV-to-oral criteria, the CRP monitoring thresholds, the Kingella PCR epidemiology and the PVL-positive severe phenotype with its DVT and septic pulmonary emboli are taken from Paediatric Acute Osteomyelitis so that the same figures apply wherever the infection sits. (See also Septic Arthritis of the Paediatric Hip, Septic Arthritis of the Paediatric Hip, Osteomyelitis Pathophysiology and Pyogenic Discitis and Osteomyelitis.)